


Abstract
Objectives: To describe the surgical approach to the treatment of iatrogenic gynecomastia via peri-areolar incision.
Methods: In this study, we describe our experience in the surgical management of iatrogenic hormonal gynecomastia with our technique described for idiopathic gynecomastia. We treated 70 patients with gynecomastia at a plastic surgery unit between 2000 and 2016. Ten of these patients had a painful hypertrophic mammary gland with grade III gynecomastia secondary to hormone therapy after prostate cancer.
Results: The presence of a very discreet scar around the areola often has very interesting aesthetic results. Areolar tissue sensation was completely preserved in 40% of patients. No short-term complications were observed; in follow-up, only one case of keloid scars was noted on a patient with dark skin, and only one case of areolar necrosis on a patient with critical breast ptosis.
Conclusion: This technique is feasible. It restores almost normal anatomy structure with minimal scarring and preserves good regional neurovascular supply, with only 60% altered areolar sensation.
Gynecomastia is an excessive development of breast tissue in men. These changes in the morphological structure of the mammary region are due to a hormonal imbalance in the concentration of estrogen and androgen that has lowered the testosterone-estrogen ratio. From a histopathological perspective, the lesions have edematous connective tissue, stoma hypertrophy, epithelial cells and galactophoric duct proliferation. At a later stage, there is a regression in cell proliferation and peri-canalicular fibrosis; thus, the lesions are persistently fixed. From a surgical perspective, the structure of the mammary region has hypertrophy of the subcutaneous tissue and malformation of the overlying skin.
The clinical classification proposed by Simon1 in 1973 divides gynecomastia into 3 grades: Grade I: small visible breast enlargement without skin excess; Grade IIa: moderate breast enlargement without skin excess; Grade IIb: moderate breast enlargement, with extra skin; Grade III: marked breast enlargement with significant extra skin, simulating mammary ptosis.
The risk factors for gynecomastia include age, medications, testosterone deficiency due to congenital or acquired gonadal deficiency, excess estradiol production, Leydig-like cell tumors, testicular cancer, para-neoplastic syndrome, and idiopathic gynecomastia.
In urology, significant gynecomastia is frequently encountered in the context of complications of hormone therapy for prostate cancer.2 Its pathophysiology is explained by a hormonal imbalance of androgen and estrogen caused by the inhibition of androgen. This condition is frequently associated with breast pain.
The literature includes 3 main modalities for gynecomastia management:2,3 radiotherapy,4 medical treatments,5 and surgery.1
We describe our technique which we used it initially for idiopathic form of gynecomastia6 and we considered it in the correction of iatrogenic gynecomastia following hormonal therapy in 10 patients.
Methods
The current study was carried out at the plastic surgery unit of Bichat-Claude Bernard Hospital, Paris, France between 2000 and 2016. During this period we have treated 70 patients who presented with gynecomastia. We have included 10 patients that had a painful hypertrophic mammary gland with grade III gynecomastia secondary to hormonal therapy, the other 60 patients had either idiopathic or obesity related gynecomastia which are excluded from the study.
All 10 included patients underwent endocrine workup and a breast ultrasound, both of which were within normal limits and presented an important grade 3 glandular gynecomastia. The mean age was 65 years (60-78) and the mean BMI was 29.
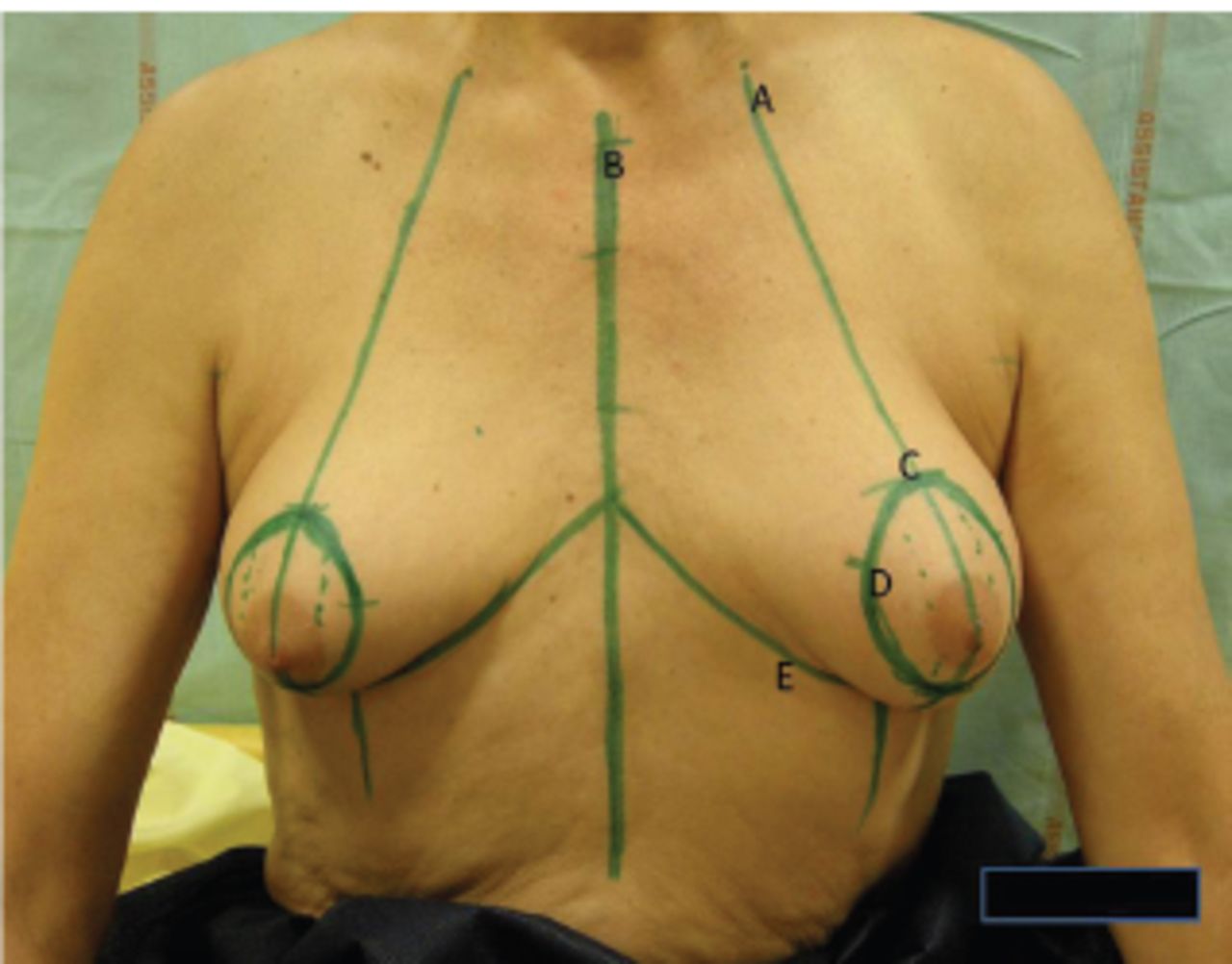
Our surgical approach and techniques in the management of gynecomastia are described below. Preoperatively, we identified and delineated the breast tissue’s peripheral boundaries in the upright position through slight pressure to the mammary region. We then made a reference point on the mid-clavicle about 6 cm from the medial clavicular end (Figure 1). We drew a line from the clavicle reference point down to the infra-mammary crease, passing through the nipples (Figure 1). The new nipple site, with a 3-cm (Figure 1) areolar diameter, was marked at 16 cm below the reference point on the vertical lines. Skin sensation in the peri-areolar area is evaluated using the pinch test technique.

- Hormonal therapy after prostate cancer of the 65 year old patient with gynecomastie grade 3. Preoperative marking: point A: reference point on the mid-clavicle about 6 cm from the medial clavicular end; point A-C: a line from the clavicle reference point down to the infra-mammary crease, passing through the nipples; point C: the new nipple site, with a 3-cm areolar diameter, was marked at 16 cm below the reference point on the vertical lines. Skin sensation in the peri-areolar area is evaluated using the pinch test technique; point D: a circular peri-areolar marking was performed, corresponding to the cutaneous region to be resected, a skin incision of about 3 mm was made at 3 o’clock and 9 o’clock. We used a 2-mm cannula to infiltrate the subcutaneous tissue with a mixture of one litre of normal saline, one milligram of adrenaline and 20 millilitres of 1% lidocaine.
A circular peri-areolar marking was performed (Figure 1), corresponding to the cutaneous region to be resected, a skin incision of about 3 mm was made at 3 o’clock and 9 o’clock. We used a 2-mm cannula to infiltrate the subcutaneous tissue with a mixture of one litre of normal saline, one milligram of adrenaline and 20 millilitres of 1% lidocaine (Figure 1).
In the first step, we carried out a liposuction of the adipose tissue at the periphery of the mammary region in a centripetal manner, using a 4-mm cannula through the cutaneous incisions at 3 o’clock and 9 o’clock. The objective was to delineate the glandular region in the retro-areolar zone. Then, we made a subcutaneous skin incision on the peri-areolar and intra-areolar markings. This delimited area was then de-epithelialized, being careful of the dermal neurovascular pedicles present at 6 o’clock and 12 o’clock.
The skin incisions previously made at 3 o’clock and 9 o’clock were then extended from 8 o’clock to 10 o’clock and from 2 o’clock to 4 o’clock, respectively, to allow for direct excision of retro-areolar glandular tissue. Excision of the gland at the superior and inferior pedicles (Figure 2) was performed carefully, leaving the adipose tissue adhered to the dermis. After checking for hemostasis, we left a Hemovac drain in place.

- Dermal incision after remove of fat by lipoaspiration. Point A-B: dermal areolar pedicle; point C: 2-4 o’clock dermal incision; point D: 8-10 o’clock dermal incision to made excision of the gland.
We closed the breast skin incision based on the Benelli tobacco purse6 suture technique, using a 2-0 Mersilene right-handed needle (Ethicon) and leaving an areolar circle with a diameter of about 3 cm. The areola suturing was completed via interrupted suture with 4-0 rapid vicryl (Ethicon). We then applied a compressive dressing to prevent postoperative hematoma or seroma. This work is approved by the surgical department at Bichat Claude-Bernard University, Paris, France. No statistical analysis is performed.
Results
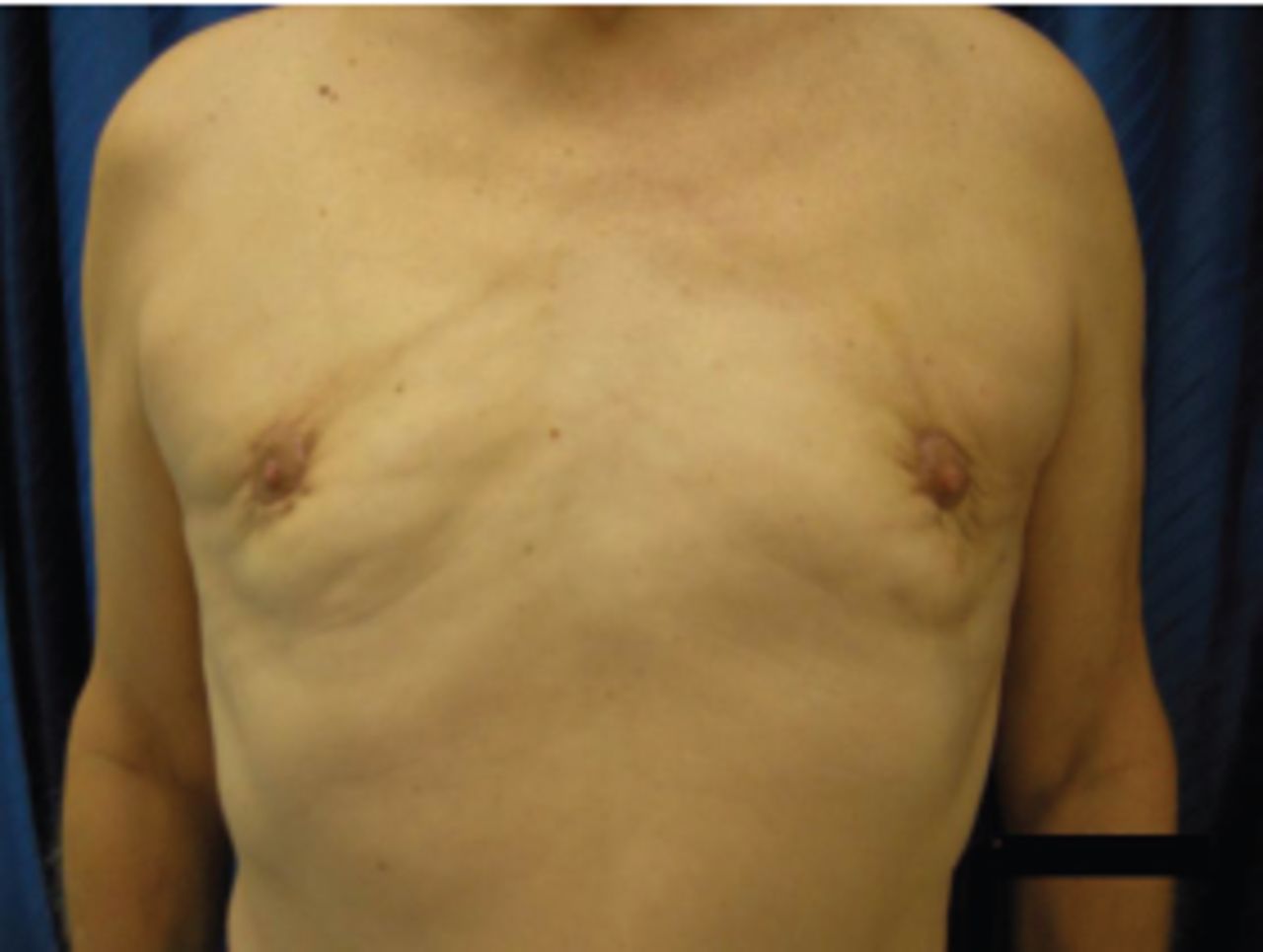
All 10 patients were admitted for 48 hours postoperatively; no short-term complications were recorded. Postoperative follow-up revealed correction of the morphological deformity with satisfactory cosmetic results beginning from the sixth month onwards (Figure 3). The surgical scar was almost undetectable, and it was masked by the natural hairiness of the area. Disappearance of the peri-areolar skin folds secondary to the tobacco purse suture was observed at six months postoperatively.
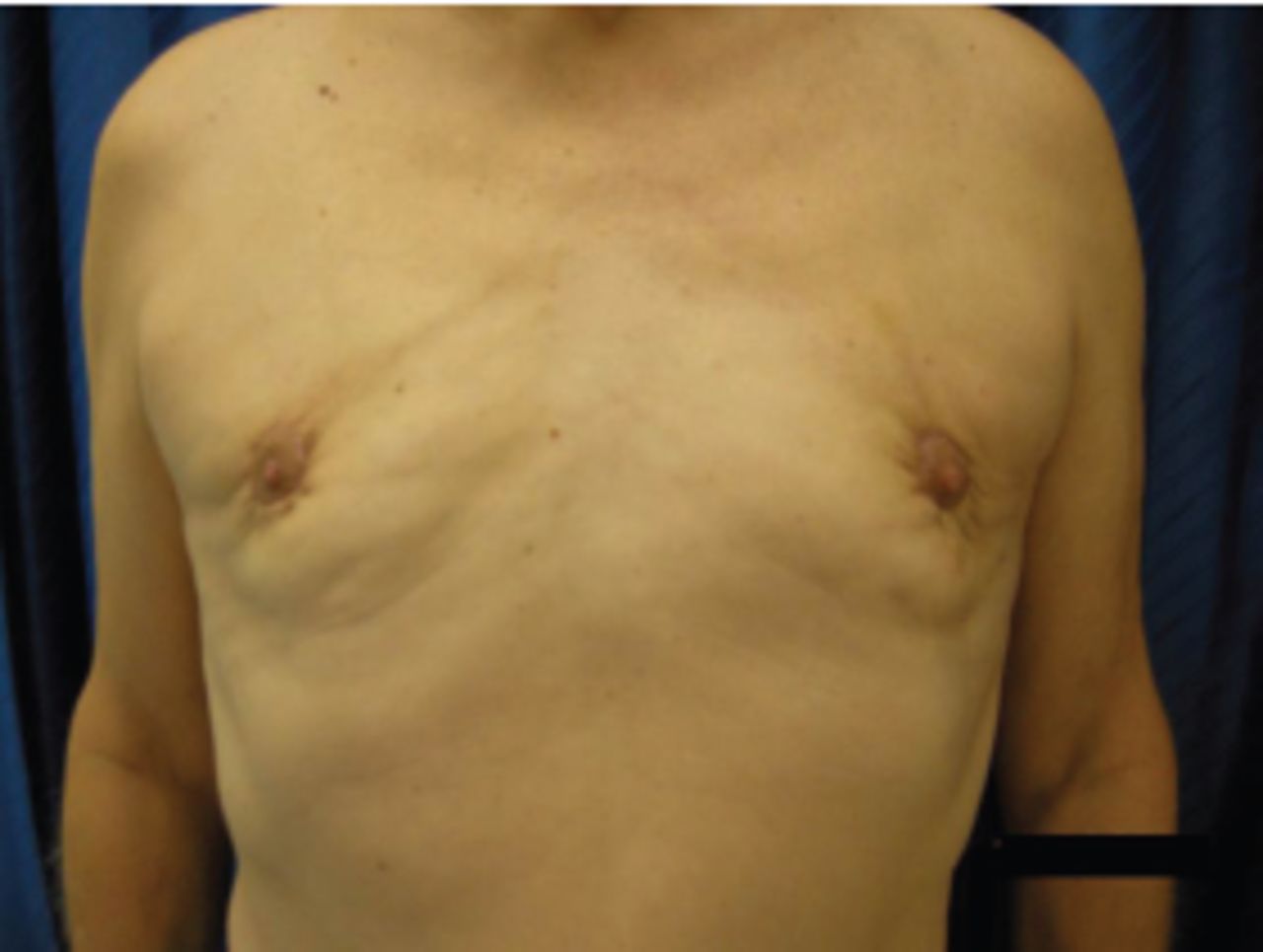
- Result after 6 months.
Out of 10 patients included in the study, we observed reduced sensation in the peri-areolar area in 6 patients (60%), while sensation was normal in 4 patients (40%). During the follow-up, only one keloid scar was recorded in a dark-skinned patient, and only one case of necrosis of the areola was seen in a patient with critical breast ptosis.
Discussion
The side effects of hormone therapy are well described in the literature,7-9 and these include hot flashes and gynecomastia, as well as sexual problems such as decreased libido and erectile dysfunction, bone demineralization, decreased muscle mass, increased fat mass, metabolic syndrome with altered lipid profile and insulin resistance. These complications can have a significant impact on quality of life.10
All types of hormone therapy are likely to cause gynecomastia. However, bicalutamide, which is a non-steroidal antiandrogen used in the management of prostate cancer, is more frequently associated with this side effect. According to See,11 gynecomastia associated with breast pain was more likely with bicalutamide than with a placebo (53.2% versus 2.9%, respectively). Though it caused mild to moderately severe pain in 90% of cases, the morphology of gynecomastia was responsible for discontinuation of bicalutamide in 15.6% of patients. Bicalutamide is more likely than surgical castration to cause gynecomastia and breast pain.11 The increase in breast volume is symmetrical in 25% to 75% of cases.
Although psychological management can be effective in helping some patients accept their new bodily appearance, gynecomastia is a physically uncomfortable and psychologically undesirable complication10 that may be a reason for discontinuation of treatment. The literature has described various approaches to skin incisions in the management of gynecomastia. In 635 d.C., Paulus Aegineta made a cutaneous incision below the breast in the inframammary crease lines. Then in 1946, Webster first proposed a semi-circular infra-areolar incision.6 Other authors have proposed peri-areolar de-epithelialization techniques followed by a transdermal peri-areolar semi-circular incision between 3 o’clock and 9 o’clock, with glandular excision through the same incision.12 Some surgeons have described a simple liposuction or a liposuction-glandular excision via a hemi-peri-areolar technique.13
Patients with iatrogenic hormonal gynecomastia are predominantly having glandular gynecomastia which is more difficult to treat due to reduce component of adipose tissues that cannot benefit from the lipoaspiration. The significant volume of glandular cutaneous tissue usually required a skin resection. If we do not want to carry out the areolar amputation and subsequent grafting,14 we are obliged to use a modification of the Benelli technique.6
In our experience, it is best to start this procedure with subcutaneous liposuction with the 4-mm cannula to facilitate the dissection of the glandular plane from the cutaneous plane. We do it centripetally, from the periphery to the nipple, to regulate the subcutaneous tissue of the breast on the periphery. We then excise the sub-areolar glandular component while causing less trauma to the areolar dermis.
According to Benelli,6 preoperative skin marking is very useful in this case. There is always a risk of neurovascular impairment during excision of excessive glandular tissues.
The transplantation of the nipple as proposed by some authors,14 in our opinion, is a traumatic technique. A hemi-peri-areolar transdermal incision between 3 o’clock and 9 o’clock restricts the blood supply from the areola to the superior neurovascular pedicle, thus increasing the risk of necrosis of the areolar complex. This risk increases when the peri-areolar zone of de-epithelialization is very aggressive because of the large pole of the areola.
In our technique, the excision of the residual glandular component in the retro-areolar after liposuction does not require extensive skin incision. The incisions in the de-epithelialized zone from 8 o’clock to 10 o’clock and from 2 o’clock to 4 o’clock facilitate excision of the gland with minimal risk of vascular impairment.
In addition, subcutaneous tunnelling with the cannula facilitates the identification of the dissection of the residual gland and reduces bleeding risk because the vessels are retracted secondary to cannula trauma. The periareolar desepidermization allows us to have enough space laterally and radially to the areola to work comfortably, safely and quickly.
We believe that it is not necessary to extend the dissection to the fascia of the pectoralis major muscle. We prefer to preserve the adipose tissues between the glandular component and the pectoralis major muscle to reduce the risk of retraction of the areola. Unlike other authors,12-15 we found that the infra-areolar neurovascular supply is more significant than the lateral. Thus, the preservation of double the neurovascular pedicles considerably reduces the risk areolar necrosis,9 at least in grade III gynecomastia.
In conclusion, in painful iatrogenic gynecomastia secondary to hormonal therapy of prostate cancer, prophylaxis radiotherapy and painkillers can be used, but neither modality treats excessive mammary glandular tissue. Our technique of surgical correction, which preserves double neurovascular pedicles, prevents areolar necrosis and retraction. It restores the male chest morphology with negligible surgical scarring. It is particularly useful in cases of massive and well-structured gynecomastia.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 18, 2020.
- Accepted February 21, 2021.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial License (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.