


Abstract
Objectives: To evaluate the role of adjuvant radiation therapy in patients with locoregionally recurrent (rpT4/N1b) papillary thyroid carcinoma (PTC).
Methods: The medical records of patients with rpT4/N1b PTC who were treated between January 2001 and December 2016 were reviewed. A total of 57 patients were analyzed, of which 24 patients were treated with adjuvant radiation therapy, and 33 patients did not receive adjuvant radiation therapy. Survival outcomes were compared between the 2 treatment groups. The primary endpoint was locoregional recurrence-free survival rate.
Results: The median follow-up period for all patients was 10.3 years (range, 2.8-19.2 years). The 15-year locoregional recurrence-free survival rate was 80.5% for those who received adjuvant radiation therapy and 28.1% for those who did not (p<0.001). The 15-year distant metastasis-free survival rate was 48.8% for those who received adjuvant radiation therapy and 33.4% for those who did not (p=0.906). The 15-year overall survival rate was 69.7% for those who received adjuvant radiation therapy and 53.1% for those who did not (p=0.921).
Conclusions: Adjuvant radiation therapy ensured favorable locoregional recurrence-free survival in patients with rT4/N1b PTC and might contribute to improving patients’ quality of life by reducing the need for additional salvage surgery and the economic burden of other salvage treatments, such as surgery or radioactive iodine therapy.
Surgical resection is considered standard treatment for locally or regionally recurrent papillary thyroid carcinoma (PTC). As an adjuvant treatment, radioactive iodine (RAI) therapy may be administered. In selected cases, radiation therapy (RT) can be employed either as a definitive or adjuvant modality. Definitive RT can be recommended for patients with surgically unresectable non-RAI avid lesions, and adjuvant RT (ART), as a treatment option, can be recommended for patients with a high-risk factor associated with locoregional recurrence (LRR), as well as those with residual disease for which additional RAI treatment or surgery is judged to be ineffective.1-4
Several studies have been conducted on the clinical benefits of ART for locoregionally advanced PTC. Adjuvant RT has proven effective in reducing LRR in patients who have high-risk factors, such as locally invasive tumors, multiple lymph node (LN) metastases, and microscopic or macroscopic residual disease.4-9 However, only a few studies have reported the survival benefits of ART for recurrent PTC.10 The difference in survival outcomes between patients with locoregionally recurrent PTC who received ART and those who did not receive ART after salvage surgery has not been well-studied.
Based on our previous clinical experience that RT was effective in lowering LRR after surgery, we selected patients with LRR (rpT4/N1b) PTC and compared survival outcomes between patients who were treated with ART and those who were not.4 We aimed to evaluate the role of ART for rpT4/N1b PTC through a comparative analysis.
Methods
Medical records between January 2001 and December 2016 were reviewed. The eligibility criteria included PTC confirmed by pathological diagnosis, rpT4/N1b, absence of distant metastasis (DM), and absence of history of other malignant diseases. Tall-cell variants of PTC were excluded. Patients with macroscopic residual disease were excluded. A total of 57 patients were found to be eligible. Twenty-four patients who received ART were classified into the RT group, and 33 patients who did not receive ART were classified into the non-RT group. Recurrences were diagnosed by preoperative imaging studies or histological confirmation. For this study, the American Joint Committee on Cancer (AJCC) staging manual, 8th edition, was used for stage grouping and tumor-node-metastasis (TNM) classification. This study was approved by the Institutional Review Board of the Korea University, College of Medicine (approval number: 2020AN0168).
All patients included in the analysis were those who underwent total thyroidectomy at initial diagnosis and underwent a salvage surgery after LRR was diagnosed.4,11 The extent of the salvage surgery was decided according to the location of the recurrent lesion. For the RT group, the median dose of 61.6 Gy (range: 57.6-70.4 Gy) in daily fractions of 1.8-2.0 Gy was delivered. The initial clinical target volume (CTV) encompassed regional LN area, superior mediastinum, and tumor bed. The high-risk CTV included areas of resected disease with margins, and the boost CTV included areas of microscopic residual tumor. The planning TV (PTV) was contoured by adding 3-5 mm CTV to PTV expansion in all directions. The PTV was cropped 2-3 mm from the body cntour.
Statistical analyses
Categorical variables are presented as number and percentage. To determine whether there was a non-random correlation between categorical variables of the 2 groups, the Pearson’s Chi-squared test or Fisher’s exact test were used. All LRR-free survivals (LRRFS) were measured from the date of surgery to first relapse. If no recurrence was documented, survival rate was measured from the date of salvage surgery to the last follow-up or death, whichever came first. The survival function from time to event data was computed using a Kaplan-Meier estimator. Statistical differences between both groups were compared using the log-rank test. The association between survival outcomes and variables was investigated using a Cox proportional hazard model. A p-value <0.05 was considered significant. IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses.
Results
Table 1 presents the patient characteristics of each treatment group. The median age of all patients at the time of salvage surgery was 52 years (range: 20-82 years). In the RT group, 23 (95.8%) received RAI treatment, while in the non-RT group, 32 (97%) received RAI treatment. Two patients, classified as RAI-refractory, did not receive RAI treatment. Iodine-131 whole-body scans were performed in 51 (89.5%) patients; 22 (91.7%) in the RT group, and 29 (87.9%) in the non-RT group, with no abnormal uptake in any patient. There were no significant differences in age, gender, pathological stage, resection margin status, or histologic variant between the RT and non-RT group. Among patients in the RT group, 18 (75%) were treated using the 3-dimensional conformal RT (3D-CRT) and 6 (25%) were treated using intensity-modulated RT (IMRT). All patients in the RT group completed the planned course of RT as scheduled.
- Comparison of patients and tumor characteristics between the RT and non-RT groups (N=57).
Survival outcomes and failure patterns
The median follow-up periods of the overall study population was 10.3 years (range: 2.8-19.2 years), RT group was 10.8 years (range: 3.3-19.2 years), and non-RT group was 9.3 years (range: 2.8-18.3 years). Nine (37.5%) patients in the RT group experienced treatment failure; 3 (12.5%) had only LRR, 5 (20.8%) had only DM, and one (4.2%) had both. All 4 patients with LRR had in-field recurrence. In the non-RT group, treatment failure was observed in 22 (66.7%); 12 (36.4%) had only LRR, one (3%) had only DM, and 9 (27.3%) had both. Eight (14%) patients died owing to DM at the time of analysis, of which 5 patients belonged to the non-RT group and 3 belonged to the RT group.
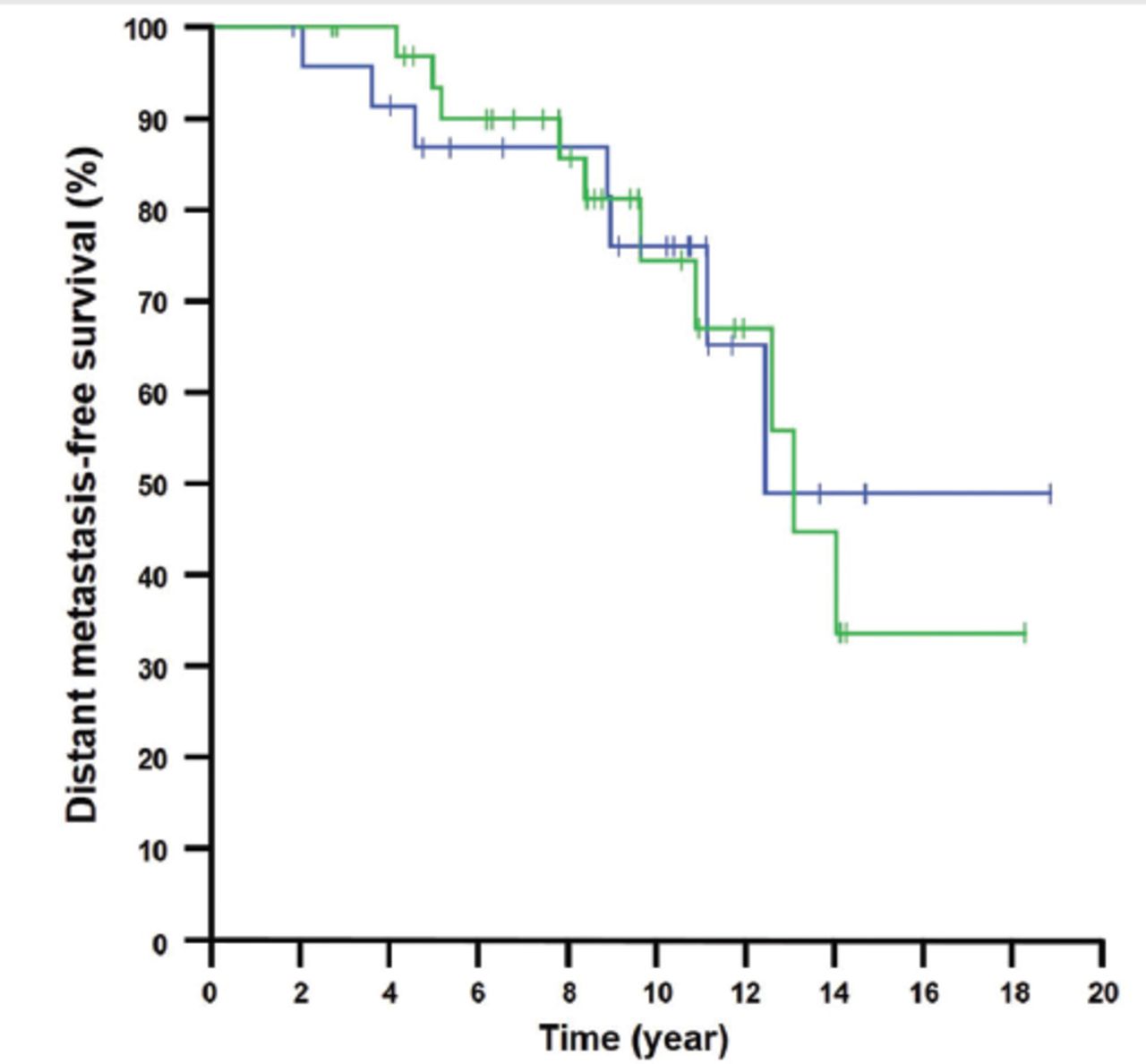
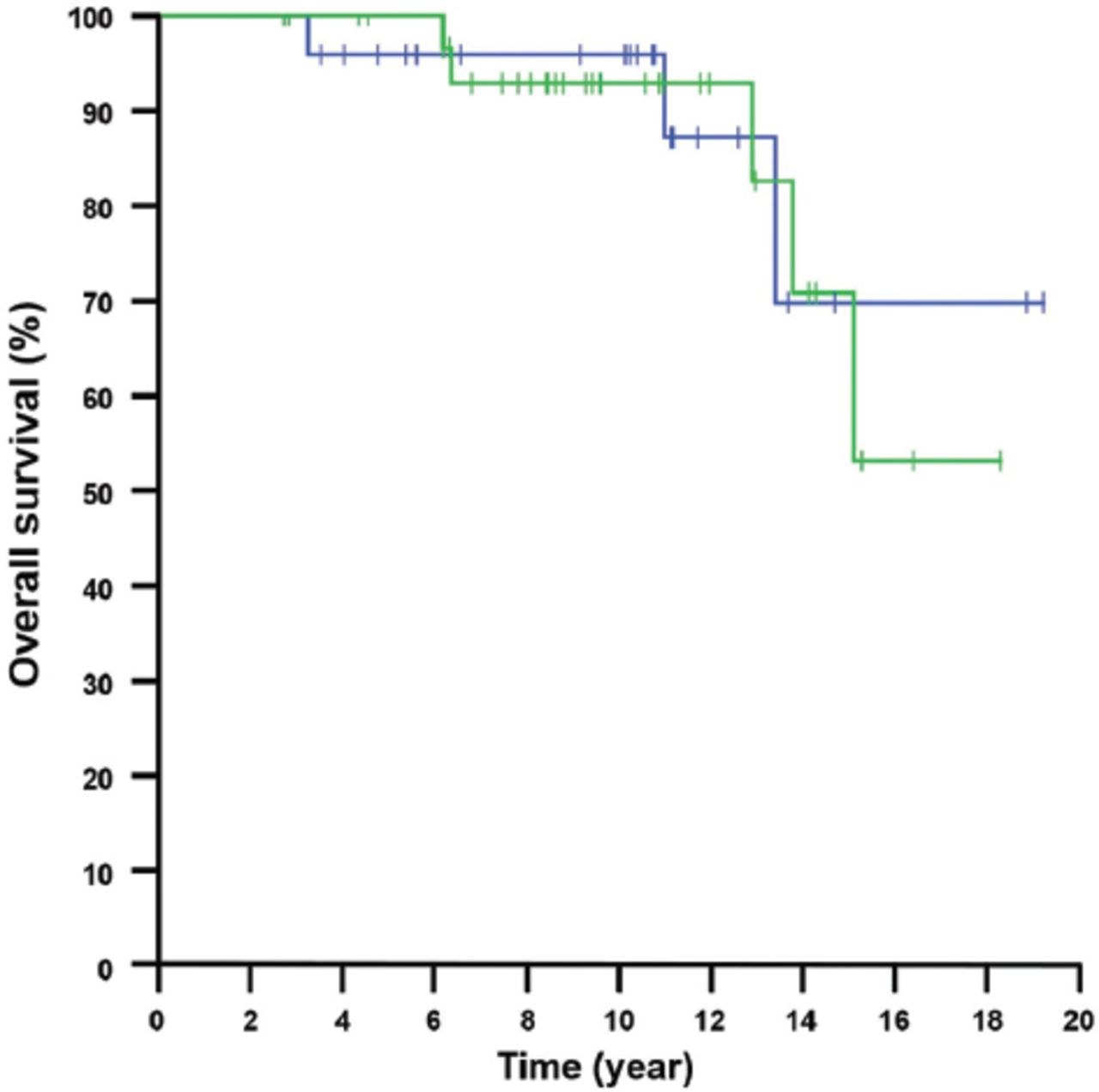
The 15-year LRRFS, DMFS, and overall survival (OS) rates for the RT group compared with the non-RT group were 80.5% vs. 28.1% (p<0.001; Figure 1), 48.8% vs. 33.4% (p=0.906; Figure 2), and 69.7% vs. 53.1% (p=0.921; Figure 3), respectively.

- Locoregional recurrence-free survival curves in patients with locoregionally recurrent papillary thyroid carcinoma in the radiation therapy (RT) group (blue) and non-RT group (green) (p<0.001).
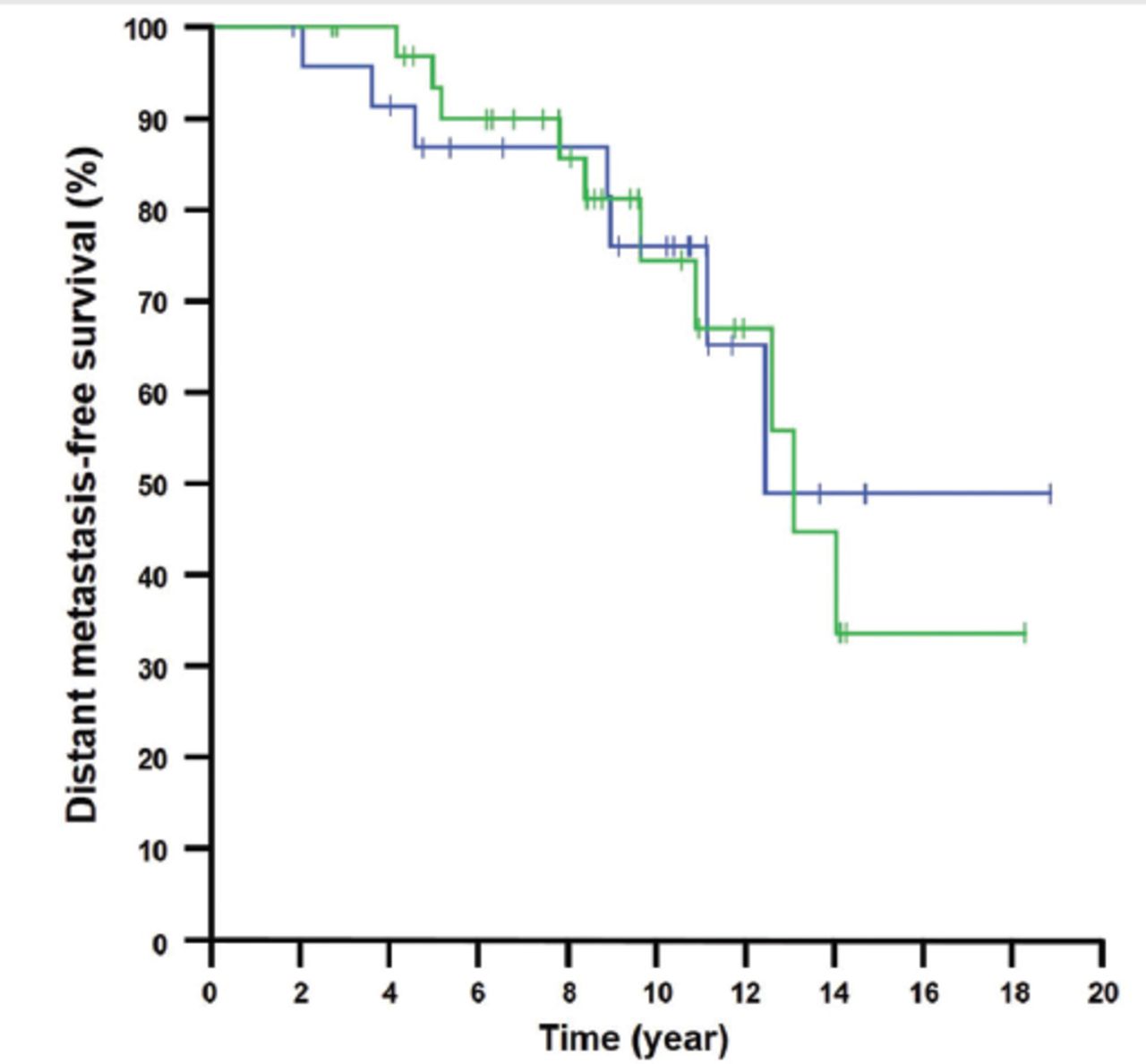
- Distant metastasis-free survival curves in patients with locoregionally recurrent papillary thyroid carcinoma in the radiation therapy (RT) group (blue) and non-RT group (green) (p=0.906).
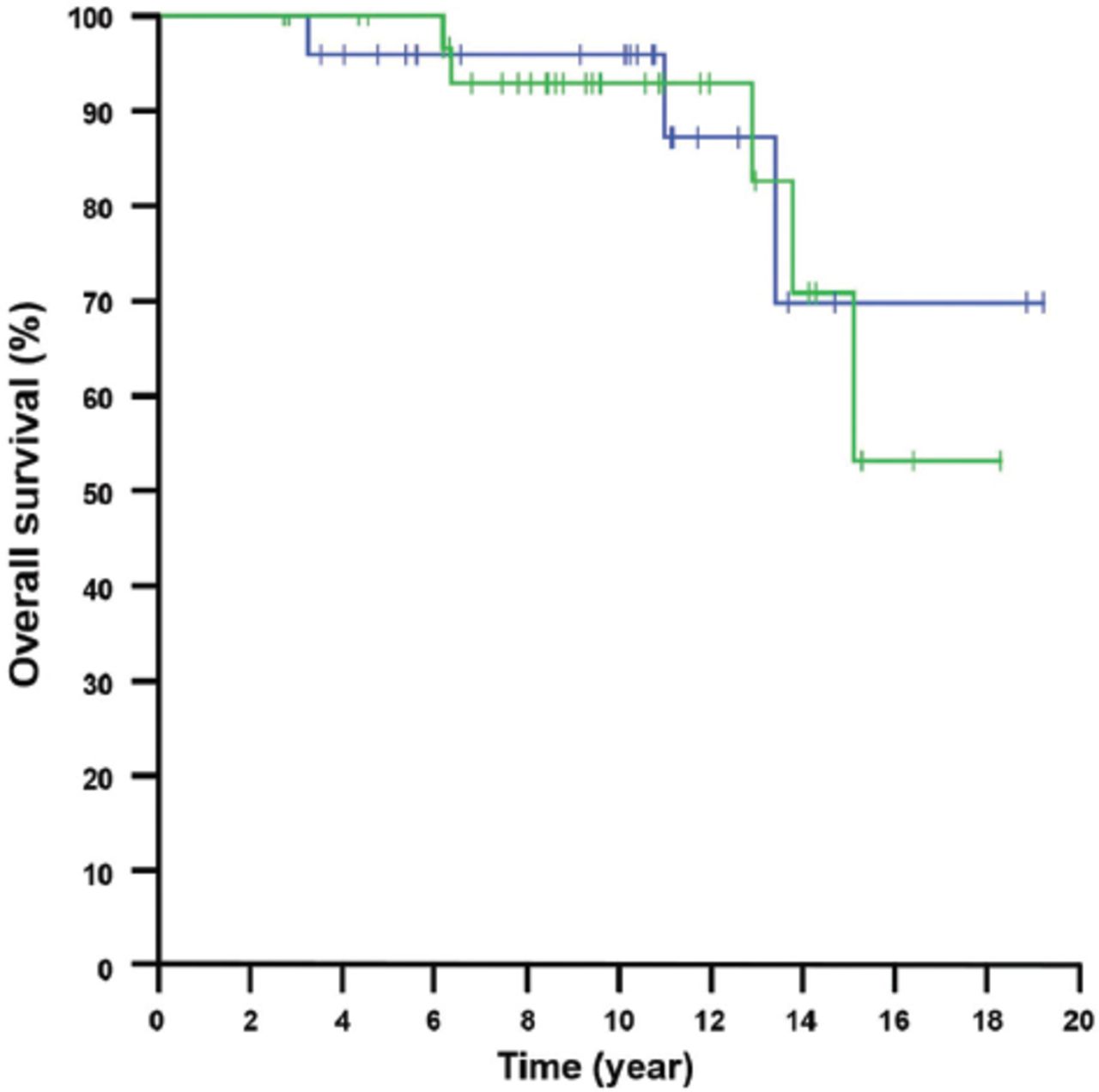
- Overall survival curves in patients with locoregionally recurrent papillary thyroid carcinoma in the radiation therapy (RT) group (blue) and non-RT group (green) (p=0.921).
Factors affecting locoregional recurrence-free survival rates
Table 2 shows the results of univariate analysis to identify the variables associated with LRRFS in the study population. Male gender (p=0.008) and the non-RT group (p<0.001) were strongly correlated with poor LRRFS in univariate analyses. Neither histologic variant, age group, nor resection margin status were significantly correlated with LRRFS.
- Univariate analysis of the 15-year locoregional recurrence-free survival in all patients (N=57).
Table 3 shows the final multivariate Cox proportional hazard model with LRRFS. On multivariate analysis, the non-RT group and male gender were independent factors associated with poor LRRFS. The odds ratio (OR) of the non-RT group relative to the RT group was 8.291 (95% confidence interval [CI]= [2.722-25.254]; p<0.001). The OR of male patients relative to female patients was 3.523 (95% CI= [1.531-8.110]; p=0.003).
- Multivariate cox proportional hazard model of variables contributing to locoregional recurrence-free survival rate.
Acute and late complications of RT
Among the 24 patients in the RT group, all patients experienced grade one or 2 acute complications affecting the skin, pharynx, and esophagus. Grade one acute skin complications included follicular or dull erythema in 17 (70.8%) patients and dry desquamation in 4 (16.7%) patients. Grade 2 acute skin complications presented as tender erythema or wet desquamation (n=3, 12.5%). Eleven (45.8%) developed mild dysphagia and 13 (54.2%) developed moderate dysphagia and were treated with narcotic analgesics. Three (12.5%) developed mild mouth dryness, and dysgeusia developed in one (4.2%). Grade 3 or higher acute complications were not observed. Dry mouth persisted in one (33.3%) of the 3 patients with grade one xerostomia during the follow-up period. All complications were scored according to the Radiation Therapy Oncology Group (RTOG) and European Organization for Research and Treatment of Cancer (EORTC) radiation morbidity scoring criteria.12
Discussion
We evaluated the role of ART for rT4/N1b PTC by comparing survival outcomes according to whether ART was administered or not. We found that the non-RT group strongly correlated with poor LRRFS and that male gender was an independent predictor of worse LRR.
The current indications for ART for locoregionally advanced PTC are not clearly defined. However, ART has shown to have a therapeutic benefit in patients with advanced PTC in several studies.4-9 Moreover, recent systematic reviews have published evidence supporting the use of ART for high-risk differentiated thyroid carcinoma (DTC) patients to improve the LRRFS rates.13,14 Although it is clear that RT is effective in reducing LRR, the reasons for its limited indications are that RT may not have any effect on OS and may cause site-specific acute and late complications. The absence of OS benefits may be associated with the relatively favorable prognosis of PTC and, even if recurrence occurs, most recurrences can be effectively treated without ART.2,14 The most common acute complications include dermatitis, mucositis, xerostomia, and dysgeusia. Late complications, although rare, include xerostomia, fibrosis, atrophy of skin and muscles, and stenosis of the trachea and esophagus. Therefore, RT should be performed with caution in selected patients where the benefits of the therapy outweigh treatment-related complications.
In recent years, modern RT including volumetric-modulated arc therapy (VMAT) and IMRT, are preferred over 3D-CRT for the treatment of any type of malignancies. These high-precision RT techniques are capable of achieving more homogeneous and highly conformal dose distributions to the PTV while delivering a reduced dose to surrounding critical organs and tissues as compared to that when using conventional 2D or 3D-CRT techniques.15,16 Therefore, our opinion is that if LRR can be lowered through IMRT or VMAT, without severe treatment-related complications, the need for repeated surgeries and consequent surgical morbidity can be reduced, thereby improving the quality of life. However, we did not describe the results of a subgroup analysis comparing 3D-CRT and IMRT techniques because only a few patients received IMRT. We thought that a relatively small sample size would fail to demonstrate a clinically significant difference. The irradiated volume of salivary glands is affected by the upper level of the target volume in RT, as well as the treatment technique used. The effectiveness of IMRT can be demonstrated if sufficient data of patients treated using this technique can be accumulated.
Adjuvant RT should be considered for selected patients with high-risk factors for LRR as well as those with residual disease for which additional surgery or RAI treatment is judged to be ineffective.1-4 Radiation therapy is recommended in many centers for patients with soft tissue infiltration of the neck or extracapsular extension of metastatic LNs.2 Although RT might be a valuable treatment option to reduce LRR, to date, limited studies have reported on the treatment outcomes of recurrent PTC.10,17 Recently, Shokoohi et al18 presented the results of survival analyses of 93 patients with recurrent DTC who had undergone salvage treatment for LRR after primary treatment. Twenty-three (24.7%) experienced local recurrence and 4 (4.3%) experienced DM. However, direct comparison with the above results is difficult because the aforementioned study included patients with carcinomas of all stages, as opposed to rpT4/N1b alone as in our study. In addition, DM might have been underestimated owing to the short follow-up time (4.1 years) considering the clinical course of DTC. Long-term follow-up is essential because thyroid cancer may recur even 10 years after initial treatment.19,20
In the present study, male gender was an independent predictor of worse LRR. Guo et al21 conducted a systemic review of risk factors affecting the recurrence of PTC. Thirteen articles were analyzed and a forest plot for recurrence revealed that male gender was related to an increased risk of recurrence (OR=1.53; 95% CI: [1.28-1.84], p<0.00001). Recently, Zahedi et al22 analyzed 2595 patients with DTC and confirmed that males had a higher risk for recurrence than females. In a multivariate analysis adjusted for AJCC stage group, male gender was linked to a 2.72-fold higher risk of recurrence (95% CI: [1.78-4.20]; p<0.001) and a 2.31-fold increased risk of recurrence when adjusted for TNM classification (95% CI: [1.48-3.60]; p<0.001). On the contrary, some studies reported that male gender was not an independent predictor for PTC relapse.20,23,24 As such, the prognostic significance of male gender remains controversial.
Study limitations
First, medical records between 2001-2016 were collected retrospectively. At that time, we did not have clearly defined institutional criteria for recurrent PTC, and the treatment of recurrent PTC may have differed from that recommended in recent guidelines such as those by the American Thyroid Association. Second, the sample size was small, which weakened statistical power. Third, the acute and late complications could have been over- or underestimated, this is because adverse events were evaluated solely based on medical records, which were subject to patient awareness. For a more accurate evaluation, objective indicators and verified evaluation methods, such as salivary function tests, will be necessary.
In conclusion, ART ensured favorable LRRFS in patients with rT4/N1b PTC and might contribute to improving patients’ quality of life by reducing the need for additional salvage surgery and the economic burden of other salvage treatments, such as surgery or RAI.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.co.kr) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was supported by the Korean University Grant.
- Received February 24, 2021.
- Accepted June 15, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.