


Article Figures & Data
Figures
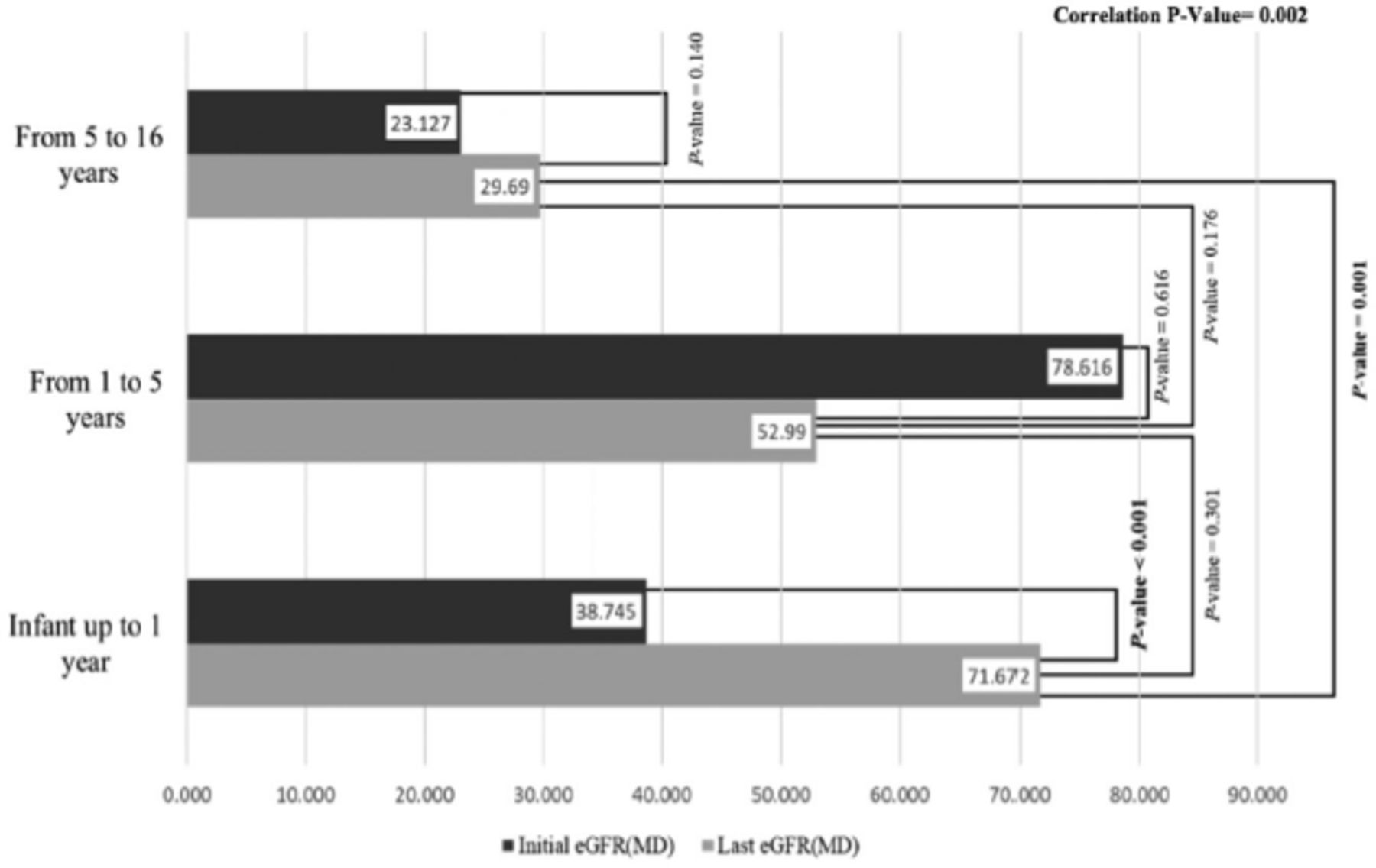
- Figure 1
- Comparison between age at presentation and initial and last estimated glomerular filtration rate test.
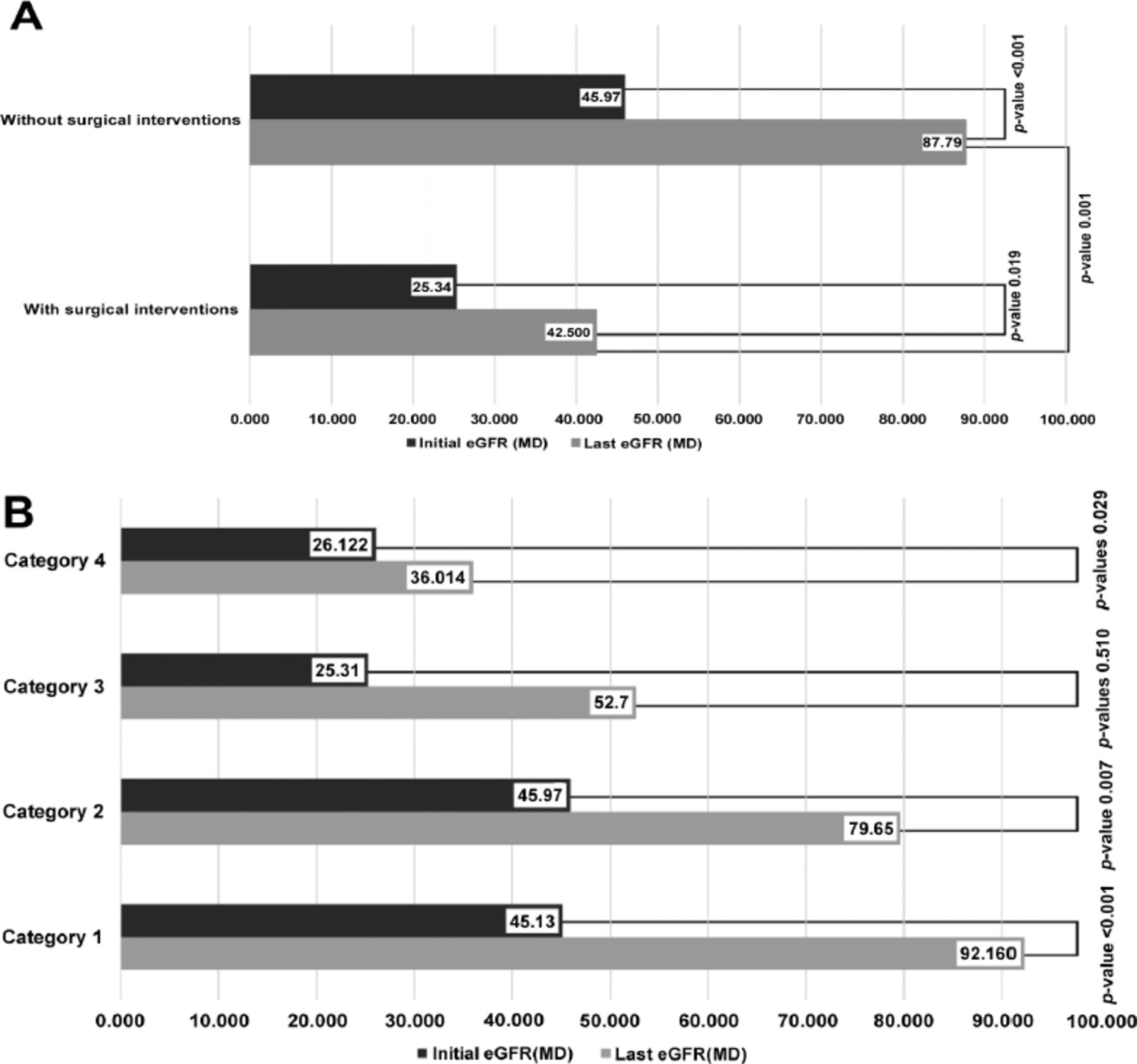
- Figure 2
- A) Comparison between the median of estimated glomerular filtration rate test (eGFR) for the surgical and non-surgical patient’s group. B) Comparison between the initial and last follow up median eGFR with regards to different management. Category 1: 62 children who did not need clean intermittent catheterization (CIC) or surgery, Category 2: 50 children who needed CIC but did not need surgery, Category 3: 25 children who have surgery but they did not need CIC, Category 4: 62 children who did need both CIC and surgery. *significant value (p<0.05).
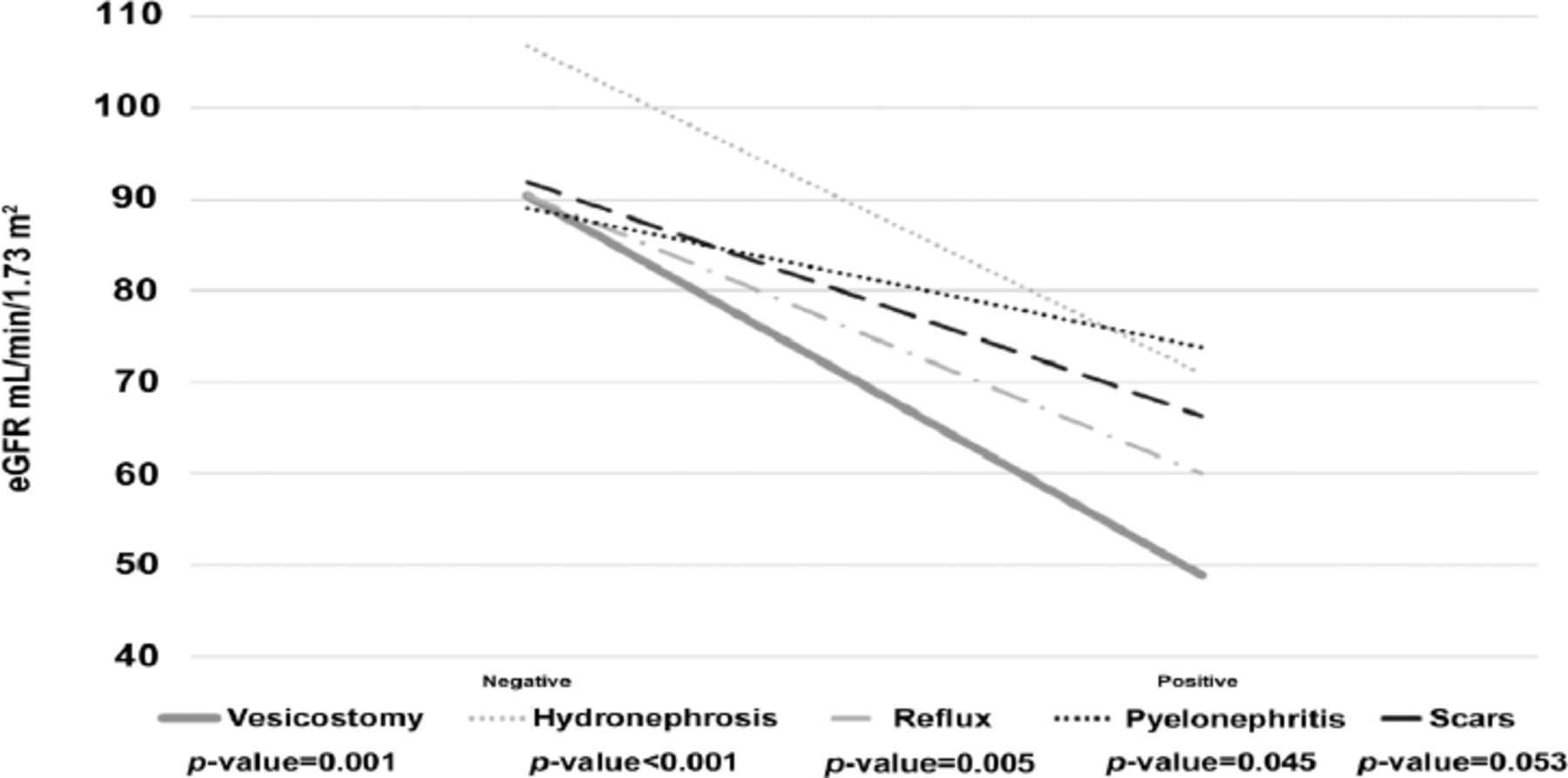
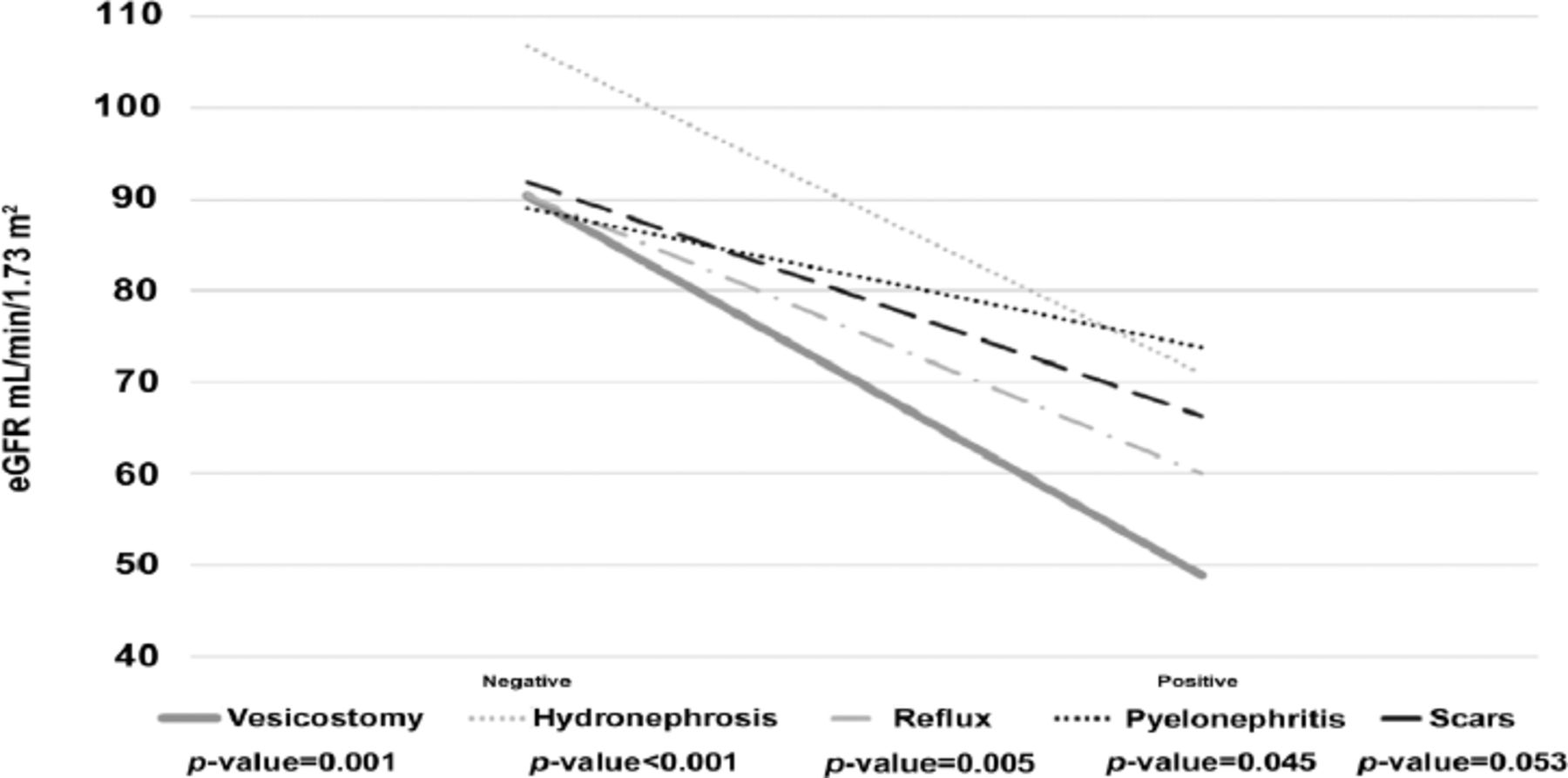
- Figure 3
- Comparison of different variables depends to the last follow up estimated glomerular filtration rate test.
Tables
Baseline demographics Total DVS (n=75) NB (n=64) VBS (n=60) n (%) Male 134 (67.3) 44 (58.6) 30 (46.8) 60 (100) Age at presentation (month) Median (range) 24 (192) 48 (192) 24 (168) 9 (156) Min (max) 0.024 (192) 0.024 (192) 0.024 (168) 0.024 (156) Mean±SD 43.9±49.6 60.1±6.32 43.5±6.21 24.1±4.37 Age at last follow-up (month) Median (range) 108 (252) 120 (252) 120 (238) 88 (192) Min (max) 12 (264) 12 (264) 14 (252) 12 (204) Mean±SD 114.7±65.2 124.9±8.5 122.1±7.7 94.0±6.7 Follow-up duration by month median (range) 72 (180) 72.0 (156) 72.0 (180) 78.0 (144) Groups of age at presentation Infancy up to 1 year 91 (45.7) 25 (33.3) 30 (46.9) 36 (60.0) Toddler (1-5 years) 52 (26.1) 20 (26.7) 17 (26.6) 15 (25.0) School age (5-16 years) 56 (28.1) 30 (40.0) 17 (26.6) 9 (15.0) Categories of management Category 1 62 (31.2) 25 (33.3) 14 (21.9) 23 (38.3) Category 2 50 (25.1) 15 (20.0) 19 (29.7) 16 (26.7) Category 3 25 (12.6) 11 (14.7) 4 (6.3) 10 (16.7) Category 4 62 (31.2) 24 (32.0) 27 (42.2) 11 (18.3) Surgical intervention Negative 112 (56.3) 40 (53.3) 33 (51.6) 39 (65.0) Positive 87 (43.7) 35 (46.7) 31 (48.4) 21 (35.0) Surgical intervention types Vesicostomy 40 (20.1) 16 (21.3) 10 (15.6) 14 (23.3) Iliocystoplasty 33 (16.5) 14 (18.7) 14 (21.9) 5 (8.3) Ureterostomy 20 (10.0) 9 (12.0) 9 (14.1) 2 (3.3) Botox 4 (2.0) 1 (1.3) 3 (4.7) 0 (0.0) Mitrofanoff/monti 6 (3.0) 3 (4.0) 1 (1.6) 2 (3.3) DVS: dysfunction voiding syndrome, NB: neurogenic bladder 2ry to spinal lesion, VBS: valve bladder syndrome, SD: standard deviation, Max: maximum, ESKD: end stage kidney disease, Botox: botulinum toxin injection into the bladder wall, Mitrofanoff: appendicovesicostomy, Monti: ileovesicostomy. Category 1: 62 children who did not need CIC or surgery, Category 2: 50 children who needed CIC but did not need surgery, Category 3: 25 children who have surgery but they did not need CIC. Category 4: 62 children who did need both CIC and surgery, CIC: clean intermittent catheterization
Baseline clinical data Total DVS (n=75) NB (n=64) VBS (n=60) P-value n (%) Initial eGFR mL/min/1.73 m2 Median (range) 39.61 (135.4) 45.15 (134.3) 66.2 (134.3) 23.1 (106.3) Min (max) 3.2 (138.6) 3.6 (129.7) 4.3 (138.6) 3.2 (109.5) 0.001 Mean±SD 50.1±2.77 49.8±36.9 66.2±44.04 33.1±27.9 Last follow-up eGFR mL/min/1.73 m2 Median (range) 59.97 (137.3) 55.0 (136.0) 90.8 (136.7) 37.7 (135.6) Min (max) 3.1 (140.4) 4.2 (140.2) 3.7 (140.4) 3.1 (138.7) 0.000 Mean±SD 66.4±3.3 65.1±46.1 84.9±46.1 48.2±40.6 Comparison median initial eGFR: last eGFR, p-value <0.001 <0.001 0.002 0.021 Hydronephrosis Negative 38 (19.1) 8 (10.7) 21 (32.8) 9 (15.0) Positive 161 (80.9) 67 (89.3) 43 (67.2) 51 (85) 0.002 Unilateral 49 (30.4) 14 (20.9) 22 (51.2) 13 (25.5) Bilateral 112 (69.6) 53 (79.1) 21 (48.8) 38 (74.5) VUR Negative 105 (52.8) 34 (45.2) 46 (71.9) 25 (41.7) Positive 94 (47.2) 41 (54.7) 18 (28.1) 35 (58.3) 0.618 Unilateral 79 (84.0) 33 (80.5) 15 (83.3) 31 (88.6) Bilateral 15 (16.0) 8 (19.5) 3 (16.7) 4 (11.4) Scars on DMSA Negative 37 (38.1) 18 (47.4) 11 (28.9) 8 (38.1) Positive 60 (61.9) 20 (52.6) 27 (71.1) 13 (61.9) 0.657 Unilateral renal scars 34 (56.7) 10 (50.0) 17 (63.0) 7 (53.8) Bilateral renal scars 26 (43.3) 10 (50.0) 10 (37.0) 6 (46.2) Obstruction on DTPA/MAG3, n=144 65 (45.1) 20 (35.1) 22 (48.9) 23 (54.8) 0.125 CIC 113 (56.8) 40 (53.3) 46 (71.9) 27 (45.0) Oxybutynin 123 (61.8) 48 (64.0) 48 (75.0) 27 (45.0) Comorbidity Pyelonephritis 102 (37.2) 44 (58.7) 33 (51.6) 25 (41.7) 0.145 Hypertension 42 (15.3) 24 (32.0) 10 (15.6) 8 (13.3) 0.013 Proteinuria 24 (8.8) 13 (17.3) 1 (1.6) 10 (16.7) 0.007 Hematuria 5 (1.9) 5 (6.7) 0 (0) 0 (0) 0.012 Progressive CKD 61 (22.2) 22 (29.3) 17 (26.6) 22 (36.7) 0.452 End Stage CKD 40 (14.6) 14 (18.7) 9 (14.1) 17 (28.3) 0.132 RRT 23 (11.5) 11 (14.6) 4 (6.25) 8 (13.3) Non 176 (88.4) 64 (85.3) 61 (95.3) 52 (86.7) Hemodialysis 11 (5.5) 6 (8.0) 1 (1.6) 4 (6.7) Peritoneal 11 (5.5) 5 (6.7) 1 (1.6) 4 (6.7) Transplantation 1 (0.5) 0 (0.0) 1 (1.6) 0 (0.0) Mortality Mortality secondary to ESKD 8 (4.02) 4 (5.3) 4 (6.2) 0 (0.0) Proteinuria ≥300 mg/L. Hematuria >10 HPF. Hypertension >95th percentile for age, gender, and height; CKD, worsening eGFR <60 ml/min/1.73 m2; end stage kidney disease, eGFR <15 ml/min/1.73 m2. DVS: dysfunction voiding syndrome, NB: neurogenic bladder due to spinal dysraphisim, VBS: valve bladder syndrome, SD: standard deviation, Max: maximum, eGFR: estimated glomerular filtration rate, RRT: renal replacement therapy, VUR: vesico-ureteral reflux, DMSA: di-mercapto-succinic acid, DTPA: diethylenetriamine penta-acetic acid, MAG3: technetium 99 mercapto-acetyl-triglycine scan, CIC: clean intermittent catheterization, CKD: chronic kidney disease
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.