


Abstract
Objectives: To analyze the prognostic value of serum presepsin value in community-acquired pneumonia focal sepsis using sepsis-3 criteria and its relationship with other biomarkers and clinical severity scores.
Methods: For this prospective observational study, 176 patients above 18 years old, diagnosed with community-acquired pneumonia, pneumonia focal sepsis and septic shock were included. It was performed in a tertiary hospital between May 2020 and December 2020. Blood samples were obtained from patients for presepsin levels at the time of diagnosis in the emergency room. The serum presepsin levels of 3 groups were statistically compared with each other.
Results: The sepsis group had significantly higher serum presepsin levels than the pneumonia group (p=0.004).
The septic shock group had serum presepsin levels than sepsis group; however, the difference was not statistically significant (p=0.25). Non survivor patients had significantly higher serum presepsin levels than survivors (p=0.001). Significant correlation determined between serum presepsin level and procalcitonin, C-reactive protein, lactate, pneumonia severity index, and quick sequential organ failure assessment (qSOFA).
Conclusion: Serum presepsin level is a new biomarker that can be used an indicator of sepsis and mortality in community-acquired pneumonia. However, for determining the prognosis of sepsis, there was no superiority detected over other biomarkers and clinical severity scores.
To improve survival, early diagnosis of sepsis and septic shock and then the application of an aggressive supportive treatment are mandatory.1-3 Anti-infection treatment should be started early and administered before definitive diagnosis. Blood culture results is the gold standard diagnostic method, but it requires several days and false negative results are frequent; however, microbial contamination can affect its diagnostic value to a large extent. In reality, microbiological information that is sufficient to ensure the appropriate treatment and to prevent needless or unnecessarily long-term treatment is missing in >50% of clinical cases. Early diagnosis and timely intervention are important for improving the prognosis of patients with sepsis.1,3,4
In recent years, focus has been on biomarkers for the early diagnosis of sepsis and the risk classification and evaluation of prognosis. New biomarkers have been developed to be used for this purpose and are extensively utilized in clinical environments. Presepsin, a new biomarker, has been reported to be closely related to monocyte-macrophage activation in infection response.1,2,5,6 Presepsin is secreted into plasma as a soluble subtype of CD14 when monocytes are activated by infectious agents.7 In the early phase of sepsis, increased presepsin levels are demonstrated in several studies and recommended as a biomarker of sepsis in clinical practice.1,5-8
In the conference of called sepsis-3, it was stated that quick sequential organ failure assessment (qSOFA) score can be used to identify patients with sepsis in the early period early, except in intensive care unit.9 This scoring system comprises criteria that can be easily determined at the bedside and is easy to use in the emergency room. Several studies have demonstrated that serum presepsin level could be used in the diagnosis and prognosis of sepsis.1,2,6,10,11 However, limited studies have been conducted based on the newly defined sepsis and septic shock criteria.
Inadequacies in early diagnosis and intervention for sepsis may occur in the emergency department (ED). The aim of this study is to investigate the role of serum presepsin level in determining the prognosis and mortality of community-acquired pneumonia-focused sepsis using new sepsis-3 criteria. In addition, it is to show the relationship between serum presepsin levels and other biomarkers and clinical severity scores.
Methods
This observational prospective study was carried out in compliance with the principles of the Declaration of Helsinki, with the ethics committee approval dated 07.05.2020 and No. 60007 from Istanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine dean’s office, in accordance with the research rules. It was performed between May 2020 and December 2020.
Patients older than 18 years of age, patients diagnosed with community-acquired pneumonia, patients with pneumonia-focused sepsis and pneumonia-focused septic shock were included in the study.
Three groups were created in the study: Group 1: patients with pneumonia (n=80), in addition to the newly developed pulmonary infiltration in radiological imaging (x-ray or tomography), patients with at least 2 of the following symptoms were included: dyspnea, cough, sputum production, fever, abnormal breathing sounds in auscultation. Group 2: patients with pneumonia focal sepsis (n=51): qSOFA criteria were used in sepsis diagnosis. The criteria used in this scoring system was as follow: respiratory count of ≥22/min, deterioration in the mental state Glasgow coma score (GCS) ≤13 and systolic blood pressure ≤100 mmHg. Each criterion was evaluated as one point and pneumonia patients with a score of ≥2 were included in the sepsis group. Group 3: patients with septic shock with pneumonia focus (n=45): in the septic shock group, pneumonia patients who required vasopressors to maintain average arterial pressure >65 mmHg and with lactate levels >2 mmol/L were included.
Patients without a definite diagnosis of pneumonia and doubtful infiltrates were excluded from the study. Pregnant women, patients with pulmonary tuberculosis, pulmonary thromboembolism, decompensated heart failure, acute attack of chronic obstructive pulmonary disease (COPD), patients using antibiotics, and patients hospitalized in the last 2 weeks were excluded from this study.
Chest x-ray or computed tomography (CT) was performed in all patients to detect pulmonary infiltration. Information about the study was given to the patients, and the informed consent was obtained. The medical histories, vital signs, demographic characteristics, additional diseases, examination findings, symptoms, imaging results and laboratory results of the patients were recorded. Pneumonia severity index (PSI) of patients were calculated and recorded.
At the time of diagnosis, ~5 mL of blood samples was obtained from the patients to analyze the level of presepsin. Measurement of serum presepsin levels was conducted in the biochemistry laboratory using the Human Presepsin ELISA kit with MBS766136 code (Mybiosource, USA), measuring within the range of 0.16-10 ng/mL with a sensitivity of <0.09 ng/mL.
Levels of other biomarkers were measured in the hospital laboratory with routine blood samples. C-reactive protein (CRP): 0-0.5 mg/dL) level was determined using the Beckman Coulter Image 800 device with the nephelometric method. Procalcitonin level was assessed using an AQT90FLEX radiometer device with the time-resolved fluorescence method (range 0 to <0.05 µg/L). Lactate levels were assessed using the radiometer ABL 800-flex blood gas analyzer. Patients were monitored for 30 days for mortality; patients with mortality within 30 days were then recorded.
Statistical method
The Statistical Package for Social Sciences (SPSS) program software for Windows version 24.0 (IBM Corp., Armonk, NY, USA) was used in the statistical analysis of the study. In the comparison of 2 groups, Mann-Whitney-U test was used for data that did not show normal distribution, and student’s t-test was used for those with normal distribution. The Kruskal Wallis test was used to compare the non-normally distributed septic shock, sepsis, and pneumonia groups. Correlation of serum presepsin levels with other biomarkers and clinical severity scores was evaluated by Spearman’s test. A p-value <0.05 was considered significant. Receiver operator characteristic (ROC) analyses for mortality and septic shock indication of biomarkers and clinical severity scores were conducted using MedCalc statistics program. Logistic regression analysis was performed for mortality determination.
Results
Eighty pneumonia, 51 sepsis and 45 septic shock patients with a mean age of 73.7±13.9 (24-103) years were included in this study. Men constituted 52.8% of the cases.
Significant difference was not determined between septic shock and sepsis groups in terms of vital signs except the systolic blood pressure. However, significant difference was determined between the pneumonia group and both the septic shock and sepsis groups in terms of vital signs (p=0.000; Table 1).
- Comparison of vital and laboratory values of 3 groups.
Significant difference was not determined in terms of routine blood values between sepsis and septic shock groups. The blood values of all 3 groups are shown in Table 1.
Significant difference was determined between pneumonia, sepsis and septic shock groups in terms of serum presepsin levels (p=0.000; Figure 1 & Table 1). Moreover, significant difference was determined between these 3 groups in terms of serum procalcitonin, CRP and lactate levels (Figure 1 & Table 1).

- Comparison of inflammatory biomarker levels between 3 groups. The figure shows that all biomarker levels were found to be significantly higher in the sepsis group than in the pneumonia group. However, there was no statistically significant difference between sepsis and septic shock in all biomarkers.
The serum presepsin levels of patients with sepsis were statistically significantly higher than those of patients with pneumonia (p=0.004). Patients in septic shock had higher presepsin levels than patients with sepsis, but the difference was not significant (p=0.25; Figure 1).
Significant difference was determined among the patients with pneumonia, sepsis, and septic shock in terms of their qSOFA and PSI scores. Unlike biomarkers, patients with septic shock had higher qSOFA and PSI scores than patients with sepsis (Table 1).
Moreover, 30-day mortality rate of patients was 45.5% (n=80). Non survivors had significantly higher presepsin levels than survivors (p=0.001). Non survivors had significantly higher procalcitonin, CRP and lactate levels than survivors (p<0.05). Non survivors had significantly higher qSOFA and PSI values than survivors (p=0.000; Table 2).
- Comparison of vital and laboratory values of the 3 groups for 30-day mortality.
Table 2 shows the comparison of vital signs and routinely studied blood parameters in terms of mortality.
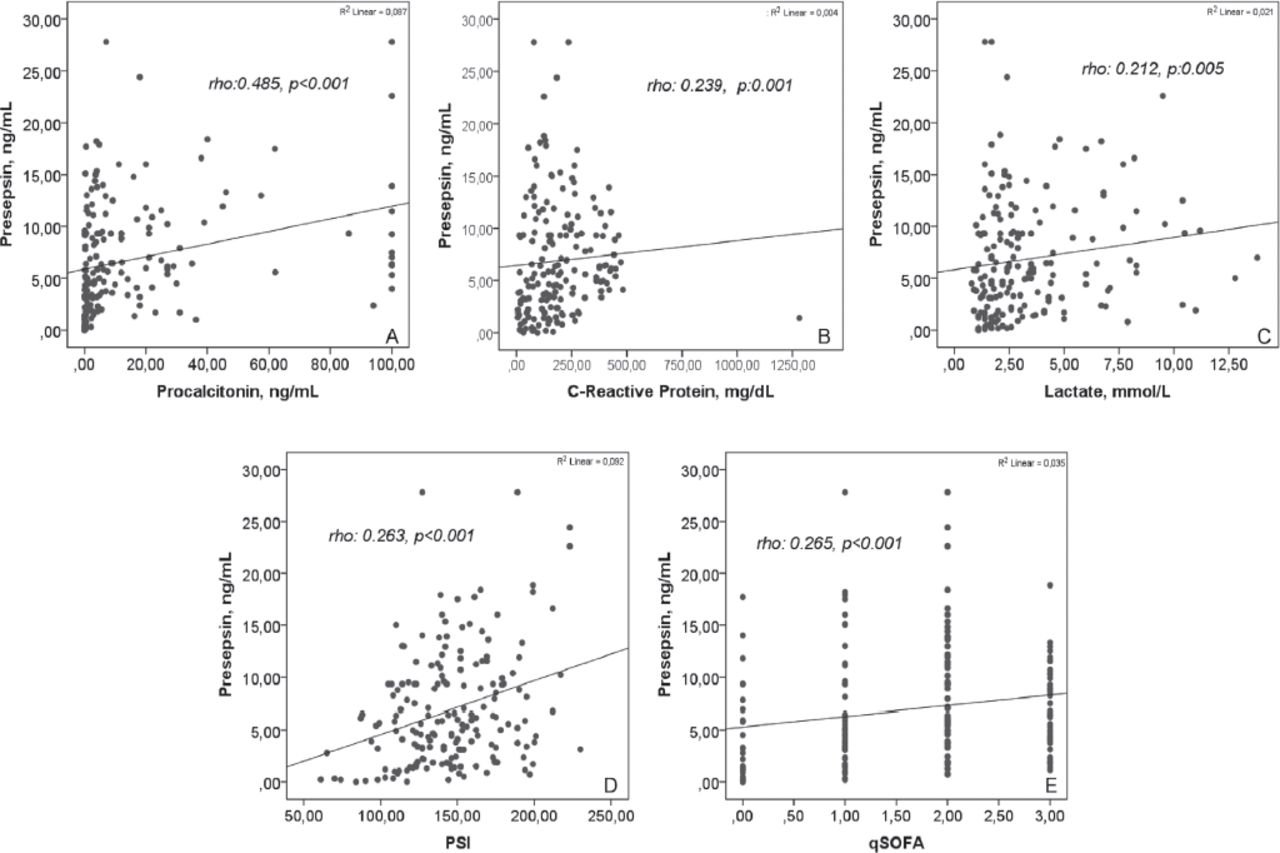
Statistically significant correlation between serum presepsin levels and procalcitonin, CRP, lactate, PSI and qSOFA was detected (Figure 2).
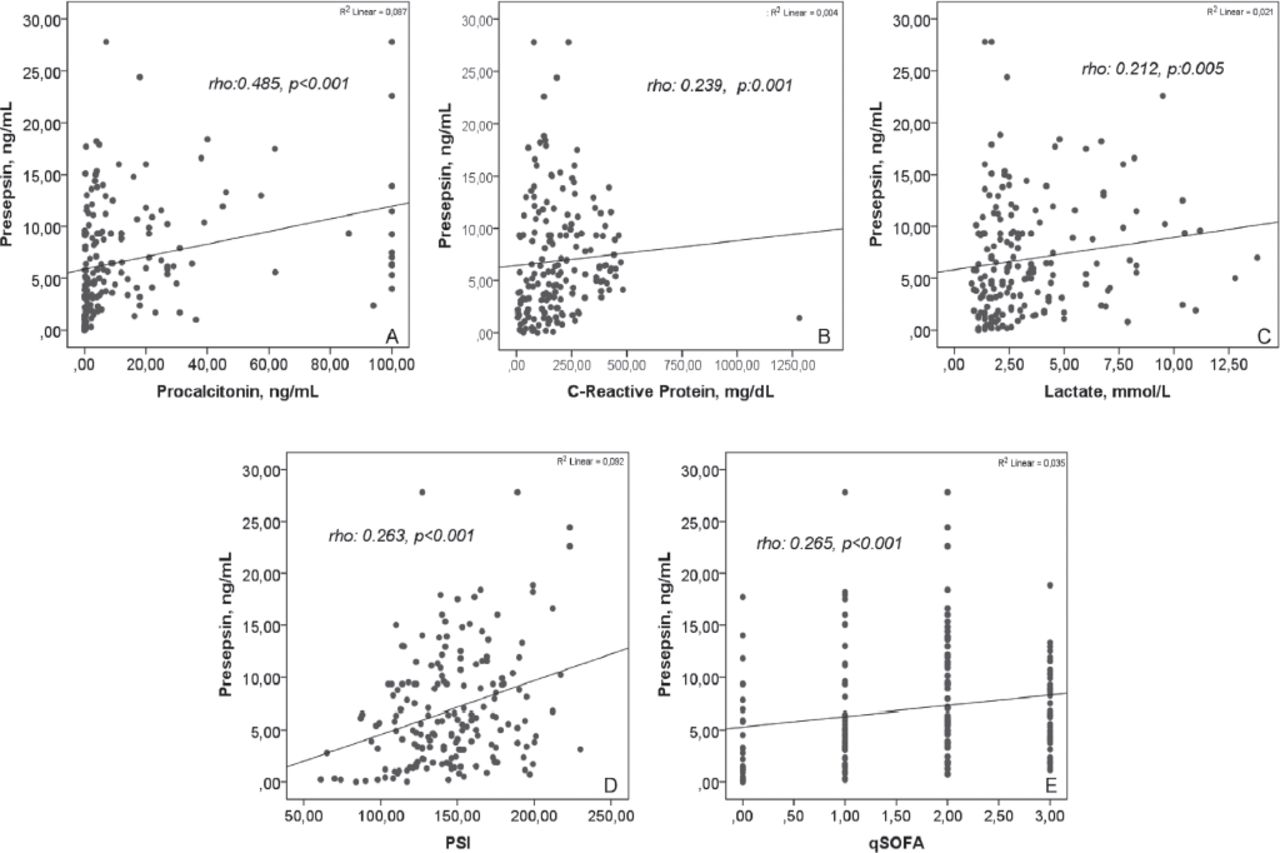
- Correlation of presepsin levels with other biomarkers and severity scores. The figure shows the significant correlation of plasma presepsin levels with procalcitonin, c-reactive protein, lactate, pneumonia severity index (PSI) and quick sequential organ failure assessment (qSOFA).
In the ROC analysis conducted for 30-day mortality indication, area under the curve (AUC) value of qSOFA was detected as 0.75. Quick sequential organ failure assessment was more successful compared to biomarkers in the indication of septic shock (Table 3).
- Receiver operator characteristic (ROC) analysis results for 30-day mortality determination and septic shock.
Pneumonia severity index and qSOFA were reported to be significant in logistical regression conducted for mortality (Table 4).
- Univariate and multivariate logistic regression analysis for 30-day mortality.
Discussion
Limited studies have been conducted based on the newly defined sepsis and septic shock criteria. Our purpose was to demonstrate the role of serum presepsin levels in the prognosis determination of patients with pneumonia focal sepsis diagnosed using the new sepsis-3 criteria.
In our study, sepsis group had significantly higher serum presepsin levels than pneumonia group. Klauche et al,1 demonstrated that presepsin levels in patients with pneumonia were higher compared to non-infectious respiratory failure patients. Also, serum presepsin levels are found significantly different between the septick shock, severe sepsis, sepsis and systemic inflammatory response syndrome (SIRS) groups according to former definitions.1 Moreover, presepsin levels increase with the severity of sepsis.1 Jereb et al,6 reported that patients with septic shock had higher presepsin levels than sepsis patients. However, in the study of Yamamoto et al,10 significant difference was not determined between septic shock and severe sepsis groups in terms of serum presepsin levels. In our study, septic shock patients had higher presepsin than sepsis patients. However, the difference was not statistically significant. In a study conducted using the new diagnostic criteria, there was no significant difference detected between sepsis (n=29) and septic shock (n=33) patient groups in terms of presepsin levels similar to our study.10 The difference of presepsin levels may be attributed to factors such as the differing number of patients and the difference in sepsis definitions.
Brodska et al,11 reported presepsin to be higher in patients with mortality. In another study, Kim et al,12 noted that mortality is higher at high levels of presepsin. Hassan et al,5 reported that the non survivors had significantly higher presepsin levels than survivors similar to our study. Presepsin has been reported to be successful in indication of mortality in all studies.
Nakamura et al,13 found that serum presepsin levels increased with the severity of injury in acute kidney injuries, independent of sepsis. They demonstrated that both sepsis and concomitant renal injury contribute to the increase in presepsin levels.13 Another study demonstrated that presepsin levels increase with a decrease in glomerular filtration rate (GFR).14 Patients with chronic renal failure were not included in our study. However, urea and creatine values were significantly different among the 3 groups in this study. Kidney function parameters were elevated because of both sepsis and septic shock. Acutely increased levels of urea and creatine may affect the increase of plasma presepsin levels.
Song et al,15 found that the AUC value of procalcitonin was 0.73, CRP was 0.53 and lactate was 0.85 for the indication of septic shock. Jereb et al,6 detected the AUC of serum presepsin levels to be 0.84 and that of serum procalcitonin values to be 0.74 for septic shock. In our study, the AUC value of serum presepsin levels was 0.65, the AUC value of procalcitonin was 0.68, CRP was 0.64 and lactate was 0.62. As per the results of our study, PSI and qSOFA were quite successful compared to the biomarkers in the prediction of septic shock.
In the study by Hassan et al,5 serum presepsin (AUC: 0.82) levels verified at the first day have higher prognostic accuracy compared to hsCRP (AUC: 0.58) in the determination of in-hospital mortality. Wen et al,2 detected the AUC value of presepsin as 0.70 and lactate as 0.71 for determining in-hospital mortality. They did not find significant difference between non survivors and survivors in terms of the serum procalcitonin levels. Kim et al,12 detected the AUC value of 0.83 for procalcitonin and 0.61 for CRP in the indication of mortality. In a study conducted by Klouche et al,1 on intensive care patients, no superiority of presepsin was noted compared with procalcitonin. Ugajin et al,16 reported that the AUC value of presepsin was determined as 0.74. Nevertheless, they only had included inpatients in the study. They reported the AUC value of serum CRP levels as 0.61. In our study, there was no significant superiority shown among presepsin (AUC: 0.64), procalcitonin (AUC: 0.67), CRP (AUC: 0.63) and lactate (AUC: 0.65) for 30-day mortality indication. There were outpatients in our pneumonia group. Profiles of patients included in the study affected the presepsin cut-off values and results.
In their study on pneumonia patients, Kim et al,12 detected the AUC value for 28-day mortality as 0.86 (sensitivity 100% and specificity 49%) according to PSI staging (cut-off ≥IV). By not using staging, we directly evaluated based on PSI results and identified the AUC value of PSI for mortality to be 0.69 (cut-off >131). Area under curve values may have been higher because Kim et al,12 used staging. They reported the AUC value of qSOFA (cut-off ≥2) for 28-day mortality as 0.81, sensitivity as 54% and specificity as 89%.12 In our study, AUC was reported as 0.75, sensitivity as 77% and specificity as 66% for qSOFA (cut-off ≥2). It is observed that severity scores in sepsis and septic shock caused by pneumonia were more successful in mortality determination compared to biomarkers. According to logistic regression analysis, PSI and qSOFA were significant as independent factors in mortality indication.
Study limitations
In our study, we could only measure the serum presepsin levels of the patients at the time of diagnosis in the ED. This situation limited our study. Serial measurement of serum presepsin levels (such as on days 3, 5, and 7) and comparison with other biomarkers could increase the power of the study.
In conclusion, this study is one of the few studies investigating the effect of presepsin levels on prognosis according to newly defined sepsis and septic shock criteria. According to the results of the study, serum presepsin level is a new biomarker that can be used for sepsis and mortality indication in community-acquired pneumonia. However, it was not reported to have superiority over other biomarkers and clinical severity scores in determining the prognosis of sepsis.
Acknowledgment
The authors gratefully acknowledge Enago (www.enago.com) for English Language Editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 9, 2021.
- Accepted July 28, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.