


Abstract
Objectives: To investigate the effect of virtual reality (VR) on anxiety, stress, and hemodynamic parameters during cesarean section (CS).
Methods: This is a randomized controlled clinical trial conducted at the operating theatre / Maternal and Children Hospital, Najran, Saudi Arabia from February to October 2021. The study comprised a random sample of 351(176 study and 175 control) low-risk pregnant women undergoing elective CS with regional anesthesia. Data collection was carried out using 5 instruments. Basic and clinical data sheet, maternal hemodynamic parameters assessment sheet, brief measure of preoperative emotional stress, a novel visual facial anxiety scale, and maternal satisfaction scale. Virtual reality group exposed to 3D natural videos associated with calm Quran or music voices via phone using VR glasses immediately after anesthesia until completion of skin suture. The control group left for routine hospital care.
Results: The VR group showed significantly lower stress and anxiety levels immediately after skin suture and 2h postoperative (p=0.000). Maternal satisfaction 2 hours after CS showed that 58% of the VR group were completely satisfied compared to 11.3% of the control group (FET=135.359 p=0.000). Virtual reality have an impact on hemodynamic parameters at some time points while peripheral oxygen saturation did not differ significantly (p>0.05).
Conclusion: Virtual reality significantly reduced anxiety and stress among women undergoing CS under regional anesthesia. Virtual reality may be added to the routine intraoperative techniques that help induce patient relaxation and increase satisfaction.
Cesarean section (CS) prevalence has significantly increased in developed and developing countries.1,2 Preceding reports from various regions of the Kingdom of Saudi Arabia (KSA) have shown an alarming increase in the CS rate of more than 80% from 10.6% in 1997 to 19.1% in 2006.3 Furthermore, in 2018 the CS rate significantly increased to 27.5%, according to a recent study carried out in the King Abdulaziz Medical City, Jeddah, KSA4 which exceeds the acceptable and recommended rate (10-15%) by the World Health Organization (WHO).5 Hence, it is the most popular abdominal surgery and one of the most popular operations in general.
Cesarean section is mainly performed using regional anesthesia, without preoperative sedatives, to facilitate the mother’s conscious birth experience, reduce the need for neonatal resuscitation, and promote skin-to-skin contact immediately after birth between the mother and newborn.6
Although CS is considered a relatively popular method of childbirth, more than 80% of women experience a significant level of anxiety and stress before and during surgery, which leads to physiological and psychological risks. The previous study has indicated that CS-related anxiety and stress are associated with an increased risk of postpartum depression.7 Furthermore, excessive stress and anxiety before and during surgery may increase anesthesia related complications during the operation, increase postoperative analgesic requirement, prolonged recovery, and delayed lactation.8 It is essential to reduce CS-related stress and anxiety because lower preoperative/intraoperative stress and anxiety lead to better maternal satisfaction and a more positive birth experience.9
In light of the limited pharmacological choices for pregnant women during CS, there is a need for alternative and low-risk options that positively affect intraoperative anxiety and stress, especially if performed under regional anesthesia.8 An alternative non-pharmacological stress reduction method is the use of virtual reality (VR). VR is a computer-assisted technology that simulates a real-life environment by integrating 3D virtual objects to create a completely virtual environment surrounding the user’s eyes to replace the natural environment.10 The VR can be designed to be an interacting and emotionally engaging environment that can stimulate emotionally related hormones. In stressful situations as CS, VR can generate a relaxation state that improves the surgery outcomes.11
The application of VR varies widely according to the purpose of its use. It is widely used for medical education, pain relief, posttraumatic stress,gait rehabilitation in Parkinson’s disease patients, anxiety, and stress.10-15 The promising VR effect makes it suitable for non-pharmacological stress reduction methods in different stressful situations during surgical procedures. In addition, it needs no or little control or preparation on the patient and the health care practitioner. Therefore, the current study investigates the effect of VR on anxiety, stress, and hemodynamic parameters during CS.
Methods
A randomized controlled clinical trial was followed in this study. It was conducted at the operating theatre (OT) / Maternal and Children Hospital (MCH), Najran, Saudi Arabia. It was carried out from February to October 2021. The trial was registered in the Iranian Registry of Clinical Trial with the number IRCT20210131050192N2. The effect of an independent variable (virtual reality) on dependent variables (maternal anxiety, stress, satisfaction, and hemodynamic parameters) were investigated. The study comprised a random sample of 351 low-risk pregnant women undergoing elective CS with regional anesthesia. Inclusion criteria were parturient with normal vision and hearing abilities, no history of generalized anxiety disorder or mental illness, free from serious obstetrics complications (according to the obstetrician evaluation), no increased intraoperative risk (such as, placental disturbance) that identified in the preoperative period and accepted to participate on the study. Any woman who developed intraoperative complications was excluded from the study.
The sample size was calculated using Yamane’s formula to make the maximum representation of the study population. According to the hospital statistical center, the sample size was calculated based on the number of CS performed at MCH hospital from January to December 2020, which was 2721 cases. Based on Yamane’s 16 formula, the sample size was calculated as the following:

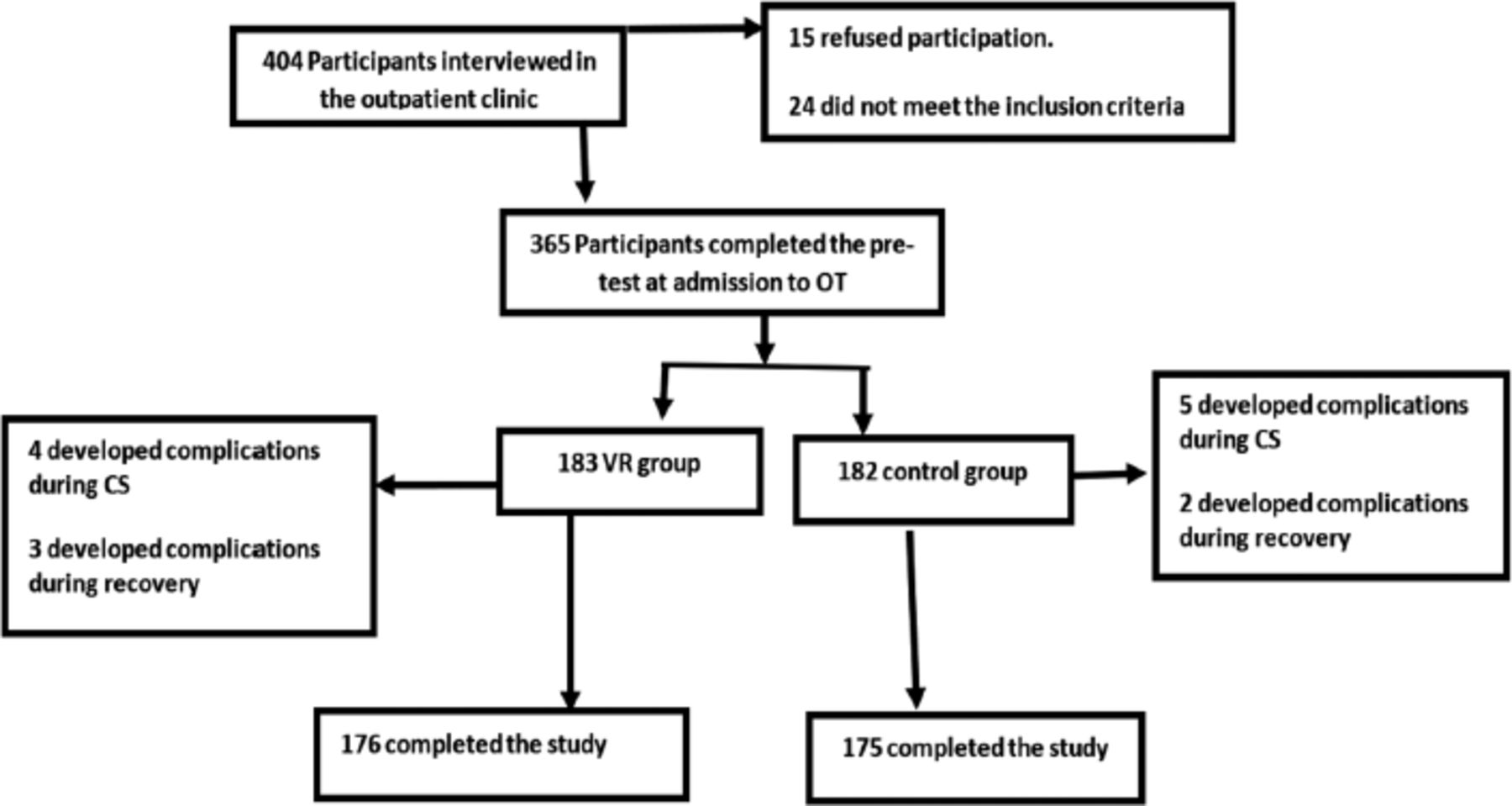
Where: n=sample size, N=total population number (2721), e=margin error (0.05). The participants were included in the study according to the following followchart (Figure 1).

- Participant’s flowchart. CS: cesarean section, OT: operating theater
A total of 351 participants were included in the study. Computer-assisted randomization was carried out to randomly assign 176 participants for the intervention group and 175 participants for the control group.
Data collection was carried out using 5 instruments after reviewing the related research on PUBMED website. Instrument I - basic and clinical datasheet: The researchers developed it to collect basic data such as age, weight, height, gestational age, gravity, parity. It also includes basic CS data, such as the number of previous CS, duration of current CS, amount of intravenous fluids, and blood loss during CS. Instrument II - Maternal hemodynamic parameters assessment sheet (objective parameters): This part was used to register the heart rate (HR), systolic blood pressure (SBP) and diastolic blood pressure (DBP), and peripheral oxygen saturation (SpO2) at patient admission OT, immediately after anesthesia, skin incision, delivery of the baby, skin suture and 2 hours (h) postoperative. Instrument III: - The brief measure of emotional preoperative stress (B-MEPS): The brief version of B-MEPS was modified by Wolmeister et al17 to measure preoperative emotional stress. The tool comprises 12 items; 3 of them are rated on a 4-point Likert scale, 6 are rated on a 3-point Likert scale, and the remaining 3 have 2 answers. The high score indicates high stress, and the total scale score ranged from 12-36. Instrument: IV: A novel visual facial anxiety scale (NVFAS): Cao et al18 developed a self-reported scale to assess acute (state) anxiety during clinical practices. It is composed of 11 faces that asses different degrees of anxiety from (0) no anxiety to (10) the highest anxiety level. Instrument V: The Birth Satisfaction Scale-Revised (BSS-R): It is composed of 10 statements rated on a 5-points Likert scale ranging from strongly disagree (1) to strongly agree (5). The patient was considered to be completely unsatisfied (10-18), unsatisfied (19-26), neutral (27-34), satisfied (35-42), and completely satisfied (43-50) based on her total satisfaction score.19
An official permission was obtained from the deanship of scientific research at Najran University, Najran, KSA. Another official approval was obtain from the health affairs administration at Najran. Ethical approval number (IRB Log Number 2021-29). After approval of the health affairs to conduct the study, official permission was obtain from the MCH director. Written informed consent was taken from each participant at the beginning of the study. The participants had the right to refuse participation or withdraw at any time. Furthermore, all the participants’ data were treated confidentially.
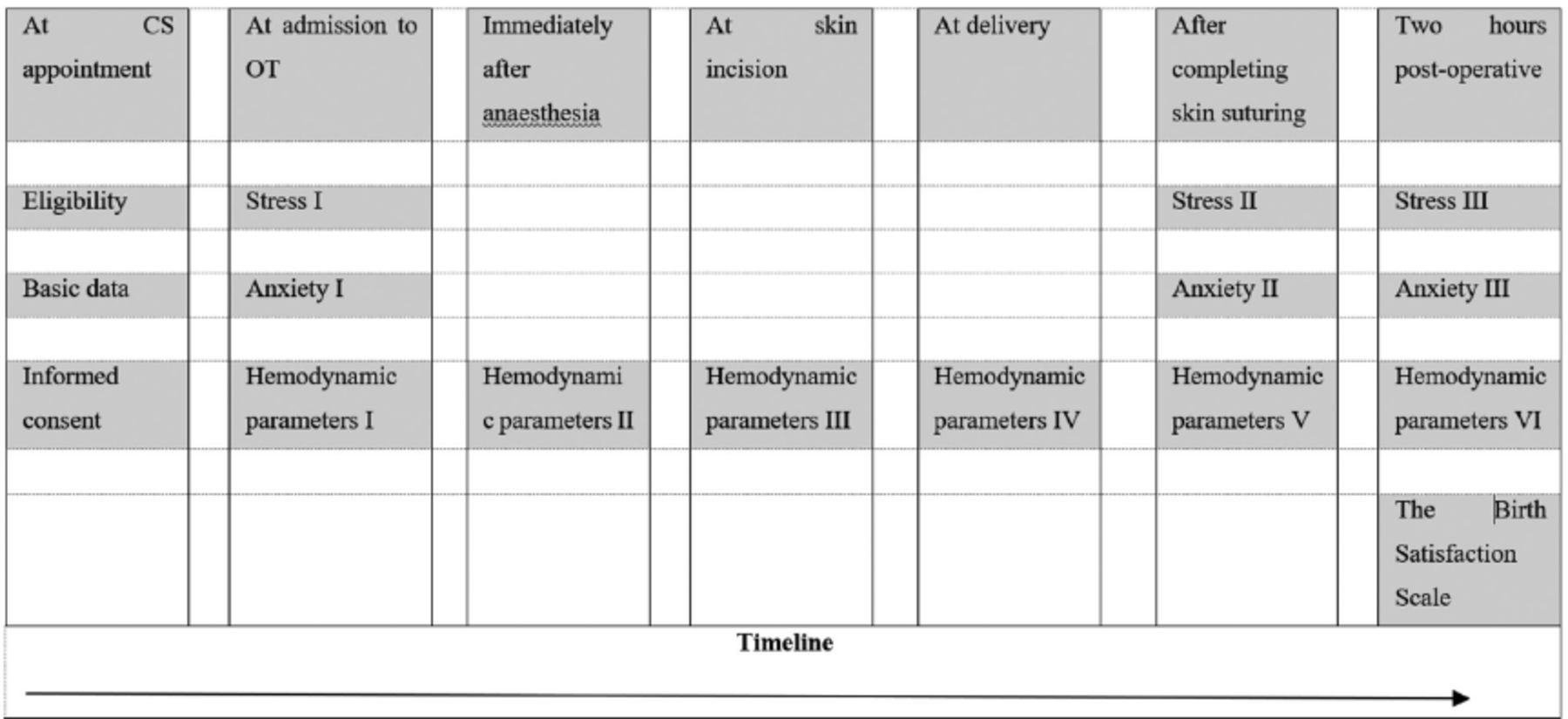
The instruments were translated to the Arabic language and tested for content validity by a jury of 5 nursing experts and reliability by Cronbach’s alpha test. A pilot study was performed on 10% of the participants (excluded from the main sample) to ascertain the instruments’ clarity and applicability; then, the necessary changes were undertaken. Each woman was interviewed individually at the outpatient clinic at the CS appointment time to ensure eligibility for the study, collect basic data, and take informed consent to participate. On admission to the OT, all women in the VR and control group were evaluated for stress, anxiety, and hemodynamic parameters using the pre-described instruments (Figure 2).

- Filed workflow chart.
For the VR group, the VR glasses were applied after regional anesthesia and during the whole operation time till completing skin suturing. The used VR glasses is Oculus Rift S PC-Powered VR Headset made in China. Every participant has to choose between listening to a Holy Quran in a sweet voice with natural landscapes and spiritual places or listening to calm, relaxing music with beautiful landscapes during surgery. Hemodynamic parameters were assessed before the intervention, immediately after anesthesia, skin incision, delivery of the baby, skin suture, and 2h postoperative. Anxiety was reassessed after completing skin suture and 2h postoperative. Brief measure of emotional preoperative stress and NVFAS were reassessed after completing skin sutures and 2 hours postoperative. In addition, patient satisfaction was assessed using a BSS-R 2h postoperative.
For the control group, they were left for routine hospital care. The same measurement timing for B-MEPS and NVFAS, hemodynamic parameters, and BSS-R were followed.
Data analysis were performed using the SPSS, version 23 (IBM Corp., Armonk, N.Y., USA)’. Before sending data to the statistician, a code was given to each group to ensure blind data analysis. To control the environmental confounding factors that may contaminate the results, only elective CS performed during the morning shift were included. In addition, the basic clinical data among the 2 groups were compared using an independent sample T-test to ensure the homogeneity of the study participants. To analyze the subjective variables of stress and anxiety at the day of CS 2X3 mixed-factorial ANOVAs between subjects’ factor group (VR versus control) and within-subject factor measurement times (at admission to OT, after completing skin suturing, and 2h postoperative) was performed. For analyzing the objective variables (SBP, DBP, HR, and SpO2), 2x6 mixed-factorial ANOVAs were utilized between-subjects factor group (VR versus control) and within-subject factor measurement times (at admission to OT, immediately after anesthesia, at skin incision, at delivery, after completing skin suture, and 2h postoperative). The adjusted Bonferroni was used to compare between VR and control group at each time point. The 2 groups’ maternal satisfaction was compared using Fisher exact test. Correction of the degree of freedom according to Greenhouse-Geisser was carried out if the sphericity was not assumed. The results were assessed within the 95% confidence interval (CI), and the p-value was considered significant at <0.05.
Results
A total of 404 participants were screened at CS appointments; among them, 351 completed the study (Figure 1). Analysis of the basic and clinical data showed homogeneity of the 2 groups (p>0.05). The mean age was 31.20 years in the VR group compared to 32.28 years in the control group. Body mass index was 32.65±4.47 among the VR group Compared to 33.61±5.89 in the control group. The mean gravidity, parity, and gestational age were 4.25±2.36, 3.63±2.49 and 38.53± 1.12 among the VR group compared to 4.68±2.20, 3.86±2.02 and 38.43±1.01 among the control group, respectively. The previous CS mean was 2.28±1.70 among the VR group compared to 2.59±1.73 in the control group. In addition, the mean duration of CS was 46.88 and 48.16 minutes among VR and control groups, respectively. The mean amount of blood loss among the VR group was 601.13 ml compared to 585.42 ml in the control group. Finally, the mean of received IV fluid was 1226.13 and 1190.28 ml among VR and control groups, respectively.
Mixed factorial ANOVAs for subjective parameters (B-MEPS and NVFAS) (Table 1)
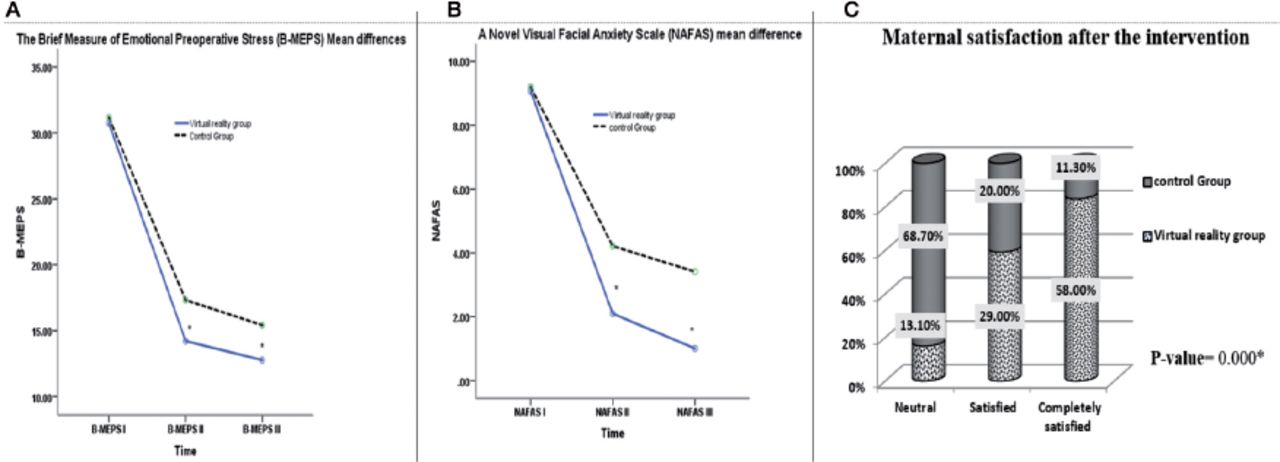
For B-MEPS, the 2×3 mixed factorial ANOVAs showed significant differences between the VR and control group [F(1)=109.511, p=0.000] with significant mean effect for time factor [F(1.438)=1284.153, p=0.000] and significant time group interaction [F(1.438)=61.307, p=0.000]. An adjusted Bonferroni comparison throughout each time point showed no significant difference between the 2 groups regarding the stress level at admission to OT [F(1)=1.784, p=0.183, mean differences= 0.427, 95% CI for d= -1.056, 0.202], while, after completion of skin suturing the VR group showed significantly lower stress level [F=(1)173.579, p=0.000, mean differences= -3.109, 95% CI for d= -3.57,-2.646]. In addition, 2h post-operative the VR group had significantly lower stress mean score [F(1)=273.635, p=0.000, mean differences= -2.65, 95% CI for d= -2.96,-2.33]. Regarding the NVFAS, mixed factorial ANOVAs showed significant differences between VR and control group in relation to time [F(1.898)=1454.845, p=0.000], group [F(1.898)=292.192, p=0.000] and for time group interaction [F(1.898)=396.826, p=0.000]. The adjusted Bonferroni comparison between the 2 groups showed no significant difference in the anxiety levels at admission to OT [F(1)=1.791, p=0.182, mean differences= -0.126, CI 95% for d= -0.311, 0.059]. After skin suturing, VR group showed significantly lower anxiety level compared with control group [F(1)=330.417, p=0.000, mean differences= -2.115, CI 95% for d= -2.344, -1.886]. Again, 2h post-operative the VR group had significantly lower anxiety level [F(1)=580.417, p=0.000, mean differences= -2.406, CI 95% for d= -2.602, -2.209](Table 1).
- Mixed factorial ANOVAs for subjective parameters (B-MEPS and NVFAS).
Mixed factorial ANOVAs for objective parameters (maternal hemodynamic variables) (Table 2)
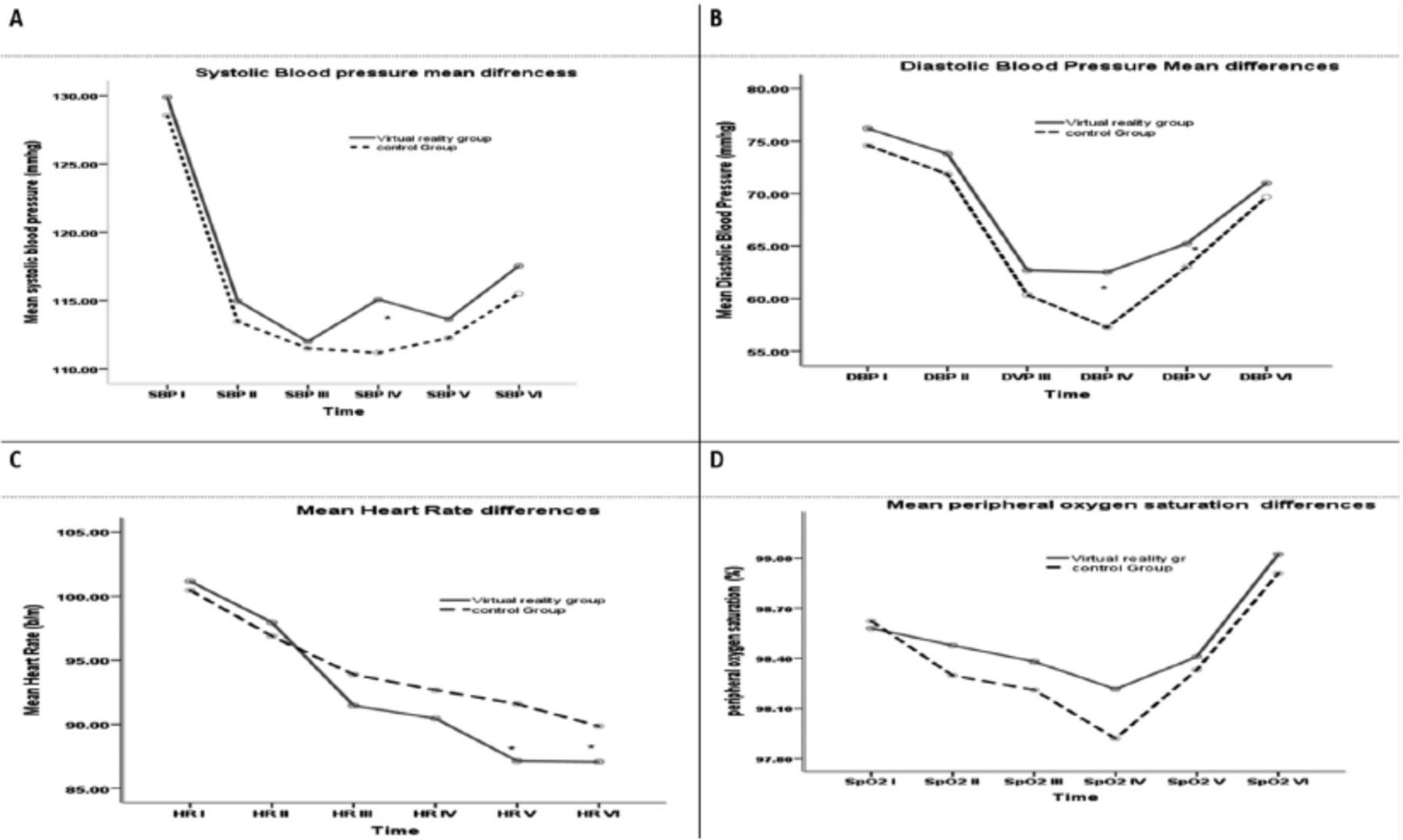
The SBP changed significantly with time factor based on the result of 2×6 mixed factorial ANOVAs [F(3.626)=86.957, p=0.000], while, no significant differences for group factor and group time interaction [F(3.626)=2.217, p=0.137 and F(3.626)=0.672, p=0.597], respectively. The adjusted Bonferroni comparison between the 2 groups showed no significant difference in the SBP at any time point except at delivery of the baby where the VR group had higher SBP compared to the control group [F(1)=5.331, p=0.022, mean differences=3.891, CI 95% for d=0.576, 7.205]. The DBP changed significantly with time and group factor [F(4.017)=145.611, p=0.000 and F(1)=8.678, p=0.003], respectively. No group time interaction was observed [F(4.017)=1.809, p=0.124]. The adjusted Bonferroni comparison between the 2 groups showed no significant difference in the DBP at any time point except at delivery and after skin suture [F(1)=14.211, p=0.000, mean differences= 5.248, CI 95% for d=2.510, 7.986 and F(1)=4.413, p=0.036, mean differences= 2.227, CI 95% for d= 0.142, 4.313], respectively. The HR changed significantly with time and group time interaction [F(2.821)=65.847, p=0.000 and F(1)=3.254, p=0.024], respectively. No significant difference in group factor found [F(2.821)=1.854, p=0.174]. The adjusted Bonferroni comparison between the 2 groups showed no significant difference in the HR at any time point except after skin suture and 2h postoperative [F(1)=13.166, p=0.000, mean differences= -4.440, CI 95% for d = -6.847, -2.033 and F(1)=9.145, p=0.003, mean differences= -2.771, CI 95% for d= -4.574, -0.969], respectively. The SpO2 changed significantly with the time factor [F(3.643)=29.329, p=0.000]. There is no significant difference in group factor or time group interaction were recorded [F(1)=2.389, p=0.123 and F(3.643)=1.010, p=0.397], respectively. The adjusted Bonferroni comparison between the 2 groups showed no significant difference in the SpO2 at any time points (Table 2)(Figure 4).
- Mixed factorial ANOVAs for objective parameters (maternal hemodynamic variables).

- The subjective parameters (B-MEPS [emotional preoperative stress], novel visual facial anxiety scale [NVFAS], and Birth Satisfaction Scale-Revised [BSS-R] among the 2 groups). A) For B-MEPS score the virtual reality (VR) group showed significantly lower stress levels immediately after skin suture and 2hours (h) postoprative compared to the control group. B) Regarding the NVFAS, the score decreased significantly in the VR group compared to the control group immediately after skin suture and 2h postoprative. C) The BSS-R 2h after CS showed that 58% of the VR group were completely satisfied compared to 11.3% of the control group with statistically significant difference (FET= 135. 359 p-value= 0.000)*p<0.05.

- The objective variables (maternal hemodynamic parameters among the 2 groups. A) The systolic blood pressure at the delivery time was significantly higher in the virtual reality [VR] group than the control group. B) The VR group showed significant increase in diastolic blood pressure at delivery and after skin suture. C) HR was decreased significantly in the VR group than the control group after skin suture and 2 hours postoperative. D) SpO2 did not differ significantly among VR and control groups at any time point. *p<0.05
Discussion
Managing stress and anxiety associated with surgical interventions is a complex and challenging process. Incorporating non-pharmacological strategies has been one of the priorities of medical care reform in the past decades. After searching international data base, this study used an experimental design to determine the effectiveness of VR as a non-pharmacological approach in reducing stress and anxiety during CS, and with the assessment of subjective and objective parameters. In the current study, although patients in both groups demonstrated lower stress and anxiety scores across 2-time points (immediately after skin suture and 2h postoperative), results revealed that patients in the VR group obtained significantly lower stress and anxiety scores when compared to the control group. The results illustrate the effectiveness of VR technologies in reducing the stress and anxiety levels among patients undergoing CS using regional anesthesia. The current results suggested that the VR technique may generate positive feelings and mood improvements to decrease the patient’s anxiety before, during and after invasive procedures. In addition, VR glasses reduce the exposure of patients undergoing regional anesthesia to visual and auditory stimuli inside the OT and generate distractions that help to reduce stress and anxiety.
These findings are in accordance with a recent randomized controlled trial carriedout by Turan et al.20 The researchers indicated that VR was effective in reducing anxiety levels during surgical intervention under spinal anesthesia.20 Also, Frey et al21 reported that the anxiety score was significantly reduced in the VR group compared to the control group during unmedicated contractions in the 1st stage of labour. A systematic review of 23 studies by Ioannou et al22 found that VR effectively decreases symptoms of stress and anxiety in various contexts and diseases.A similar positive effect of VR technology in reducing stress and anxiety in other medical procedures have been reported by prior studies.23,24 In addition, VR distraction has also been shown to control stress and anxiety in patients undergoing dental treatment.25-28 Besides, VR technology is most frequently used in the management of anxiety disorders and other psychiatric diseases.29,30
On the contrary, Walker et al31 & Glennon et al32 reported no significant difference between the VR and control groups regarding anxiety scores among patients undergoing cystoscopy and bone marrow aspiration, respectively. The difference may be attributed to the different technological factors and the audiovisual material provided through the VR glasses, which may improve the degree of VR distraction to reduce stress and anxiety.
Nowadays, data collection on patient’s satisfaction is significant for assessing and improving the quality of medical care; therefore, the maternal satisfaction assessment took place in the current study. The present study results demonstrated that maternal satisfaction regarding the overall delivery process was significantly higher in the VR group than in the control group. More than half of the patients were completely satisfied in the VR group compared to around one-tenth of the control group. This result is in line with Alaterre et al,33 they reported that the satisfaction scores in the VR group were significantly higher than those of the control group in patients undergoing regional anesthesia. Moreover, Dumoulin et al34 found that children satisfaction concerning needle-related procedures was significantly higher in the VR group than TV group. Also, Tharion et al35 stated that the postoperative satisfaction score in the VR group was significantly higher than the midazolam group.
Regarding the hemodynamic parameters, the present study results showed no significant difference in the SBP at any time point except at delivery, where the VR group had higher SBP compared to the control group. The DBP does not change significantly among the 2 groups at any time point except at delivery and after skin suture. Furthermore, HR decreased significantly among the VR group compared to the control group after skin suture and 2h postoperative. Although the SpO2 changed significantly with the time factor, there is no significant difference in the 2 groups at any time point.
In line with the current study, Baytar and Bollucuoğlu conducted a quasi-experimental study to investigate the effect of VR glasses on preoperative anxiety before septorhinoplasty. They illustrated that HR significantly decreased after VR glasses use, while SpO2 did not differ significantly.36 Also, Tharion et al35 explored the effectiveness of VR on reducing anxiety in patients undergoing surgery under spinal anesthesia. They reported that VR did not significantly affect SpO2 or the other hemodynamic parameters except for respiratory rate. However, all the hemodynamic parameters were stable among both groups throughout the surgery. In addition, Sahin et al37 stated that VR utilization during surgery could help hemodynamic stabilization due to the stress reduction mechanism. The benefits of VR in pain reduction and physiological parameters among non-medicated labouring women was examined by Frey et al21 and found that VR significantly reduced HR and pain. Also, Hua et al38 reported that VR significantly decreased heart rate among children during dressing on chronic lower limb wounds. They added that SpO2 did not differ significantly among VR and control groups.
On the contrary to the present study, Baytar and Bollucuoğlu reported that VR significantly decreased SBP and DBP among their participants. The differences between the current study results and that of Baytar and Bollucuoğlu may be attributed to the different situations of data collection.36 The present study data were collected in OT, and the patient received regional anesthesia, which is known to be associated with hypotension and increasing HR.39 Therefore, stabilizing the patient’s hemodynamic state requires a slight elevation of SBP and DBP. Baytar and Bollucuoğlu36 collected their data before operation inside the patient room; therefore, the relaxation induced by using VR leads to a reduction in SBP and DBP, which were already elevated due to the physiologic mechanism of preoperative stress and anxiety.
Study limitations and strengths
Blindness cannot be applied in this study at the data collection because of the procedure nature. There are some contributing factors to stress and anxiety that we could not control, such as religion, education, period of waiting before the operation, social support system and previous experience with OT. Both primiparous and multiparous women were included in the current study due to limited number of elective CS for primiparous. Strengths of this study include enough sample size (351) and repeated measurement at different time points. Also, we used standardized tools for data collection.
In conclusion, VR significantly reduced anxiety and stress among women undergoing CS under regional anesthesia. This safe, cheap, harmless, and easy to use method of stress reduction has a positive impact on some hemodynamic parameters and significantly increased patients’ satisfaction. Virtual reality may be added to the routine intraoperative techniques that help to induce patient relaxation and help to increase satisfaction. However, numerous studies are needed to confirm the benefit of VR intraoperative for primiparous women.
Acknowledgment
The authors are thankful to the Deanship of Scientific Research at Najran University for funding this work under the General Research Funding program grant code (NU/-/MRC/10/323). Also, we would like to thank Grammarly Inc (https://www.grammarly.com/) or English language editing.
Footnotes
Disclosure. This study was funded by the Deanship of Scientific Research, Najran University, Najran, Kingdom of Saudi Arabia. Grant No.: NU/-/MRC/10/323.
- Received December 23, 2021.
- Accepted March 21, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.