


Abstract
Objectives: To evaluate serum neutrophil gelatinase-associated lipocalin (NGAL) concentrations of pregnant women complicated with coronavirus disease 2019 (COVID-19) and investigate its diagnostic value for the severity of COVID-19.
Methods: Of the 46 pregnant women with COVID-19 included in the study, we further classified these women into 2 subgroups: the non-severe COVID-19 group (n=25) and the severe COVID-19 group (n=21).
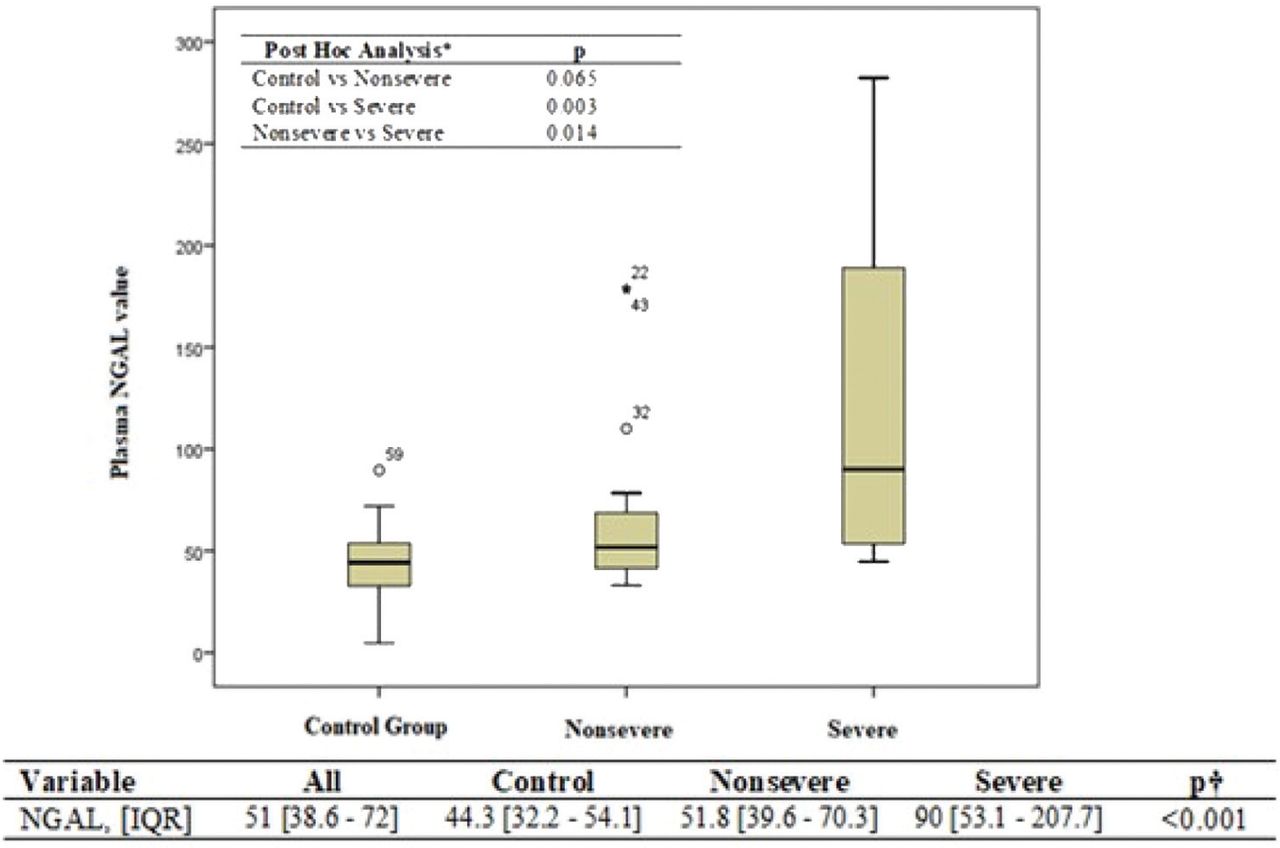
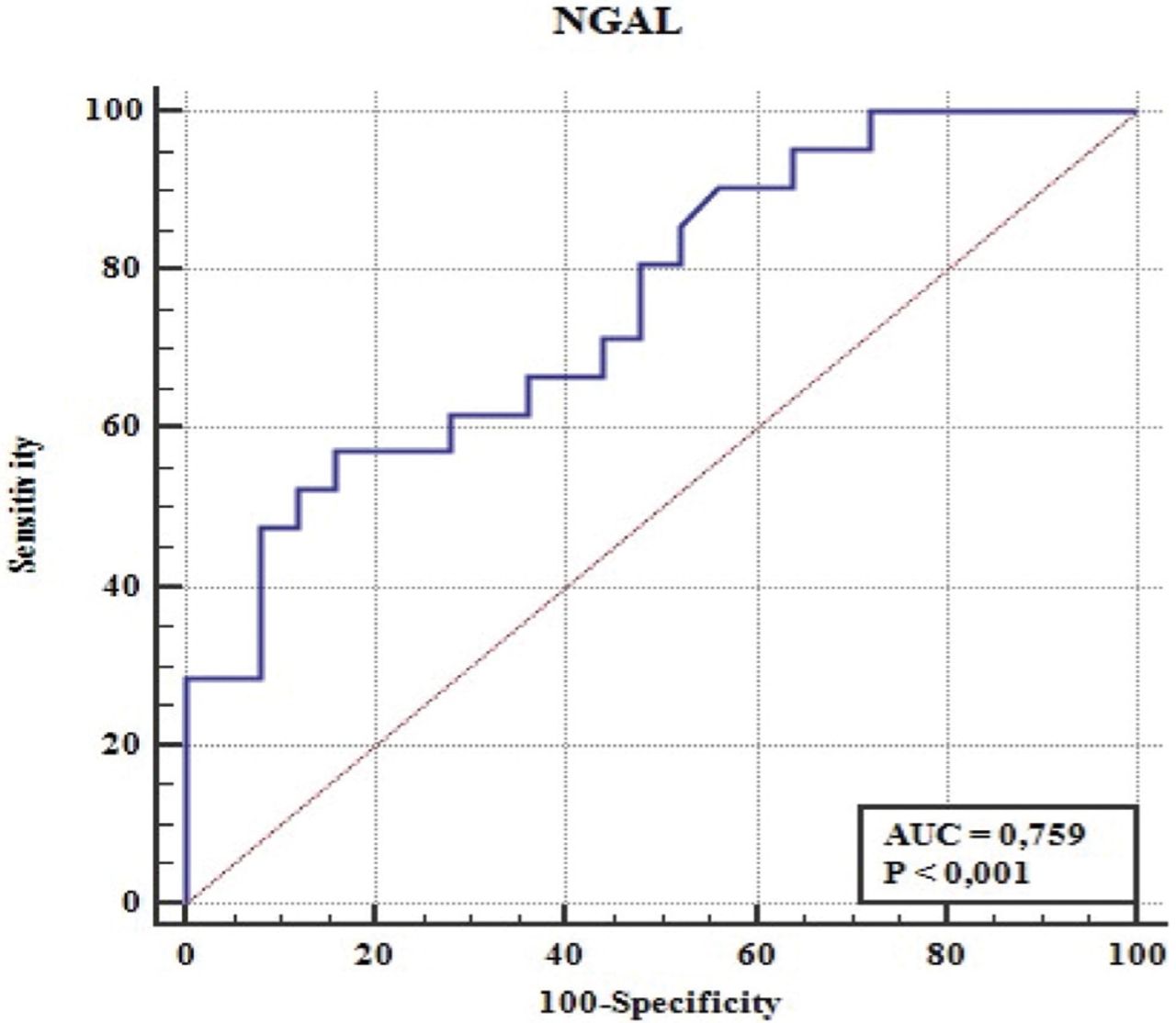
Results: Neutrophil gelatinase-associated lipocalin plasma concentrations were significantly higher in pregnant women complicated with severe COVID-19 (90 [53.1-207.7] ng/ml) compared to those from pregnant women with non-severe COVID-19 (51.8 [39.6-70.3] ng/ml) and healthy pregnant women (44.3 [32.2-54.1] ng/ml, p<0.001). Also, at a cutoff value of 72 ng/ml, NGAL predicted severe COVID-19 with a sensitivity rate of 57% and a specificity rate of 84%. Serum NGAL level (adjusted hazard ratio [aHR]=1.020, 95% confidence interval [CI]= [1.006-1.035], p=0.007), and D-dimer level (aHR=2.371, 95% CI= [1.085-5.181], p=0.030) were the variables that were revealed to be significantly associated with the disease severity.
Conclusion: We demonstrated that NGAL was highly associated with COVID-19 severity. We consider that NGAL might be a useful biomarker to diagnose the disease severity in patients with COVID-19.
Coronavirus disease -2019 (COVID-19) is a respiratory infectious illness, which was recorded firstly in central China and recognized to be caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1-3 With the rapid evolution of the outbreak, which spread indiscriminately and sustainably across continents, this disease has become more common in pregnant women across all trimesters of gestation.4
Coronaviruses may cause a wide variety of respiratory diseases varying from the flu to fatal pneumonia.5 Severe acute respiratory syndrome coronavirus 2 shares a 50% similarity of the genome sequence with Middle East respiratory syndrome coronavirus (MERS-CoV) and 79% with human SARS-CoV-1, and are classified in the same betacoronavirus subgroup.6 During previous outbreaks of coronavirus, pregnant patients were more vulnerable to infection and these cases resulted in a higher proportion of severe disease and adverse obstetric outcomes, including maternal morbidity and mortality than non-pregnant patients.7,8 Pooled data revealed a maternal mortality rate of 25% for MERS-CoV and 18% for SARS-CoV-1.4 The majority of initial investigations indicated that pregnant women with COVID-19 experienced less severe illness and adverse maternal outcomes than the previous coronavirus pandemics. Moreover, the course of the disease has been stated to be identical in both non-pregnant and pregnant women.9,10 However, recent studies suggested that pregnant women suffered from more severe illness and higher hospitalization rates compared to non-pregnant women.11,12 Thus, additional diagnostic hallmarks need to be identified to improve the understanding of the virus’s accurate extent, develop prediction abilities of the disease severity, and reduce its morbidity and mortality.
Since neutrophils are the first immune responders to the viral invasion site, a substantial rise in their numbers within the regional microenvironment subsequently after viral infection is identified.13 It was proposed that these cells improve antiviral defenses by interplay with diverse cells of the immune system, virus internalization and cell death process, degranulation, cytokines release, and neutrophil extracellular traps (NETs).14 Neutrophil gelatinase-associated lipocalin (NGAL) structurally exists in the peroxidase negative granules of neutrophils.15 Neutrophil gelatinase-associated lipocalin was also expressed in alveolar type II pneumocytes and bronchial epithelial cells, and this expression was reported to be significantly upregulated during lung inflammation.16 A recent study proposed that urinary NGAL levels could manifest the lung injury severity in COVID-19 patients.17
This study assesses maternal serum NGAL concentrations of pregnant women complicated with COVID-19 and investigate its diagnostic value for the severity of COVID-19.
Methods
This prospective case-control study was carried out in the isolation ward of Istanbul Kanuni Sultan Süleyman Training and Research Hospital, Istanbul, Turkey, from May 2020 to September 2020. We included 46 pregnant women with confirmed COVID-19 diagnoses. All cases had a history of exposure and clinical evidence of COVID-19. Cases were diagnosed with COVID-19 based on the World Health Organization (WHO) definition.18 Ethical approval was obtained from the Ethics Committee of the same hospital (2020.06.65). This study took place consistent with the Declaration of Helsinki Ethical Principles.
We used real-time reverse transcription-polymerase chain reaction on nasopharyngeal swab specimens of the patients to detect SARS-CoV-2 nucleic acid and to confirm the clinical diagnosis. Pregnant women with COVID-19 underwent clinical examination of symptoms and vital signs, laboratory test results, and radiologic chest examination at admission. Achest x-ray or thoracic computed tomography (CT) was carried out for the diagnosis of pneumonia. Before these radiologic procedures, all pregnant women were informed regarding the requirement, benefits, and probable adverse outcomes of chest x-ray and thoracic CT scan by the attending clinician, and signed an informed consent form.
Of the 46 patients with COVID-19 included in the study, we further classified these cases into 2 subgroups: the non-severe COVID-19 group (n=25) and the severe COVID-19 group (n=21). Mild and moderate cases were categorized as the non-severe COVID-19 group, and severe and critically ill cases were defined as the severe COVID-19 group. Pregnant COVID-19 cases were classified into mild, moderate, severe, or critically ill cases in line with the findings from symptoms, clinical findings, and lung imaging at admission to the hospital.9,19 We defined cases with mild symptoms with or without mild changes on chest radiography as mild cases. Patients with respiratory manifestations, fever, and radiological findings indicative of pneumonia were considered moderate cases. We defined severe COVID-19 cases as the existence of one or more of the following findings: shortness of breath (respiration rate: ≥30/minute), hypoxia (resting: oxygen saturation [SaO2] ≤93%), and arterial oxygen partial pressure (PaO2/FiO2) of ≤300 mmHg in arterial blood. Critically ill patients were defined as a respiratory failure that requires mechanical ventilation, respiratory or other organ failure event that needs intensive care unit (ICU) admission, or shock.
We excluded patients with known malignancy, infected with respiratory viruses other than SARS-CoV-2, infected with human immunodeficiency virus, Hepatitis B virus, Hepatitis C virus, and using immunosuppressant drugs. Patients who had mild or moderate diseases at the time of admission and blood collection, but developed severe illness during the course of infection were also excluded. Serum samples collected from 30 healthy pregnant volunteers were served as a control group for serum NGAL value.
We extracted all demographic features, laboratory values, and clinical outcomes from the hospital records of the patients. We carried out the baseline laboratory examinations, including NGAL examination, within 2 days of admission before the initiation of treatment. Patients were discharged when the temperature of the body returned to normal for at least 3 days with substantially improved respiratory symptoms and significant resolution of inflammation in pulmonary imaging.
We collected the blood samples in tubes containing heparin by venipuncture. We removed serum samples by centrifugation for 10 at 3000 x rpm and maintained them at -80°C before carrying out assays. Samples were dissolved and Human NGAL (Catalog No: E1719Hu, Bioassay Technology Laboratory, China) levels were measured in serum samples. Briefly, we added the standards and samples to proper wells which are pre-coated with Anti-Human monoclonal antibodies prior to incubation. We added biotin to all wells and combined it with Streptavidin-HRP to form an immune complex; then carry out incubation and washed to remove the uncombined enzyme. Then, we added Chromogen Solution A, and B for the liquid color to change into blue. The color finally turns yellow due to the effect of acid. We read the optical density on an automated plate reader at 450 nm (Thermo Scientific Microplate Reader, USA). The kit has an efficient range of 5-600 ng/mL and a sensitivity of 2.01 ng/mL.
Statistical analysis
The categorical variables were presented as a percentage. We presented the continuous variables as median (interquartile range [IQR]), if not normal distribution, and mean ± standard deviation (SD), if normal distribution. We utilized the Chi-square (χ2) test to compare the categorical variables between the groups. We utilized the Shapiro-Wilk test to evaluate whether the variables were normally distributed. The Mann-Whitney-U test or Student’s t-test was utilized to compare the continuous variables between the groups based on whether these variables were normally or non-normally distributed. One-way ANOVA (Brown-Forsythe) was utilized to compare >2 groups. Post hoc multiple comparison analysis was carried out by using the Games-Howell test. To determine the independent predictors for COVID-19 severity, the variables, which were detected to be related to it at a p-value of <0.05 level as a consequence of univariate analysis, were entered in the multivariate logistic regression analysis where the Enter method is utilized. We determined the capacity to discriminate between the cases with and without severe COVID-19 using the receiver operating characteristic (ROC) curve and area under the curve (AUC), accompanied by a 95% confidence interval (CI). Discriminatory power was classified as ‘good’ if AUC was ≥0.70 and inadequate was <0.70. We calculated the optimal cutoff value from the point of maximal specificity and sensitivity by utilizing Youden’s index. All statistical analyses were carried out using the Statistical Package for the Social Sciences, version 24.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 53 pregnant women who experienced COVID-19 were admitted to our hospital. After dropping participants meeting the exclusion criteria, the final sample size of this study was 46. We classified these patients into 2 subgroups: the severe COVID-19 group (n=21) and the non-severe COVID-19 group (n=25). In the non-severe group, 19 patients had mild COVID-19 and 6 cases suffered from moderate COVID-19. In the severe group, 19 patients were described as severe COVID-19 and 2 patients were defined as critically ill cases. No patient experienced acute kidney injury (AKI) or died in our study population.
We presented the demographic features and obstetric outcomes of the study cohort in Table 1. The groups were comparable concerning maternal age, gravidity, body mass index (BMI), cesarean section rates, the gestational week at delivery, and length of hospital stay. When we evaluated the laboratory findings of the cases, the median C-reactive protein value was significantly higher in the severe COVID-19 group (43.4 [18.9-63.7] mg/L) than in the non-severe group (p=0.005). Severe COVID-19 cases had significantly higher procalcitonin values than the non-severe cases (p=0.007). The median D-dimer value tended to be significantly higher in pregnant women who suffered from severe COVID-19 than that of the non-severe COVID-19 patients (p=0.009).
- Demographic characteristics and obstetric outcomes of the study cohort (N=46).
We demonstrated the serum NGAL values of the study cohort in Figure 1. We found significantly higher NGAL values in the severe COVID-19 cases than those of the non-severe COVID-19 patients, and healthy pregnant women (p<0.001). We investigated the diagnostic value of serum NGAL levels regarding the COVID-19 severity (Figure 2). The optimal cutoff value for NGAL is set at 72 ng/ml with a specificity of 84% and a sensitivity of 57% for diagnosing severe COVID-19.

Plasma neutrophil gelatinase associated lipocalin (NGAL) levels of patients with or without severe coronavirus disease -19 survivors. IQR: interquartile range
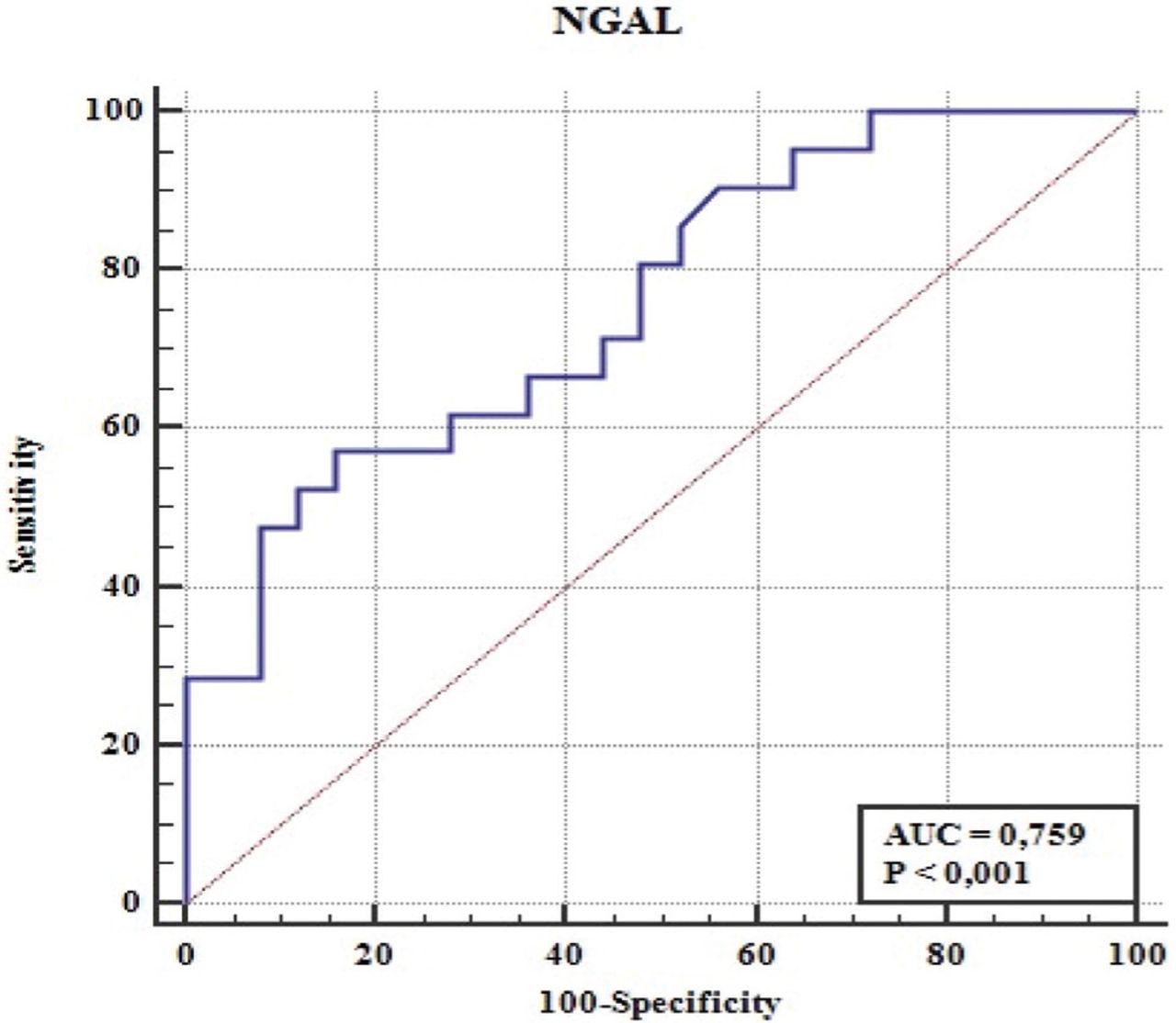
Discriminatory ability of neutrophil gelatinase associated lipocalin (NGAL) in determining the severity of pregnant patients with coronavirus disease -19. AUC: area under the curve
Univariate analysis and multivariate cox regression analysis were carried out to describe variables independently connected with the COVID-19 severity (Table 2). Serum NGAL level (adjusted hazard ratio [aHR]=1.020, 95% CI= [1.006-1.035], p=0.007), and D-dimer level (aHR=2.371, 95% CI= [1.085-5.181], p=0.030) were the variables that were revealed to be significantly associated with the disease severity.
- Factors that were found to be independently associated with the severity of coronavirus disease -19 in a univariate anaylsis and in a multivariate logistic regression analysis.
Discussion
The current study intended to assess the maternal serum NGAL concentrations in pregnancies complicated with COVID-19 regarding the severity of the disease. We found that NGAL showed significantly elevated levels in the serum of pregnant women suffering from severe COVID-19 than the non-severe group and the healthy pregnant women. Also, the factors that were found to be independently connected with the COVID-19 severity were serum NGAL and D-dimer levels.
Physiological respiratory changes throughout pregnancy, including diaphragm elevation and reduced functional residual volume in the lungs, lead to an increased risk of maternal susceptibility to viral infections and worsen maternal outcomes.20 Also, pregnancy induces a shift from T-helper-1 (Th-1) to T-helper-2 (Th-2) associated immunity, which may also enhance the risk of vulnerability to viral infections.9 Pregnancy is a unique immunological condition that is modulated since the immune system is influenced by signals derived from the placenta.21-26 According to this knowledge and previous experiences with coronavirus epidemics, it was proposed that pregnant women could be more severely influenced than the non-pregnant cases by COVID-19. Nonetheless, the vast majority of initial reports of pregnancies with COVID-19 have demonstrated an asymptomatic or mild disease course, with only few patients requiring ICU admission or mechanical ventilation. Also, these data have been mainly limited to a few series of cases.9,10,20 Recently, Ellington et al11 suggested that pregnant women (31.5%) are more probably to be hospitalized, and an elevated possibility of ICU admission compared to the non-pregnant individuals (5.8%) among young women with COVID-19. Also, COVID-19 manifests specific difficulties in pregnancy management and adverse pregnancy outcomes. Therefore, the definition of potential markers that predict the disease severity may be extremely useful for medical staff to effectively prioritize patients, individualize medication, and observe clinical progress at all care levels to reduce adverse pregnancy outcomes.27
The underlying cause for elevated risk of severe illness and mortality remains unclear for COVID-19.
Since COVID-19 may induce a cytokine release syndrome and cytokines perform a vital function in initiating the inflammatory response, it was anticipated that the disease severity has linked to alterations in the immune response.27,28 Coronavirus disease -19 patients admitted to ICU had higher serum levels of several pro-inflammatory cytokinesthan non-ICU cases, and these cytokines modulate the course of the disease.29 However, it was still poorly understood what initiates and propagates the cytokine storm syndrome. Barnes et al30 concluded that the exacerbated host response in severe COVID-19 patients was related to the aberrant neutrophil activation. Also, emerging studies showed neutrophilic mucositis, neutrophil extra vasation into the alveolar space, acute capillarities with fibrin deposition, and infiltration of neutrophils in pulmonary capillaries in lung autopsies of COVID-19 cases.30,31 Neutrophil gelatinase associated lipocalin is produced in the granules of neutrophils. Also, NGAL is synthesized in alveolar type II pneumocytes, renal proximal tubular cells, and several healthy tissues.32 Although the function of NGAL remains unknown, it is considered to perform an essential role in the immune response to numerous diseases. An up-regulation in serum NGAL levels has been demonstrated in acute and chronic inflammatory diseases, pulmonary thromboembolism, acute and chronic renal failure, ischemic diseases, and solid tumors.16,32,33 In a recent study, Komaru et al17 revealed that urinary NGAL concentration at ICU admission was increased in cases who subsequently suffer from AKI during their stay in ICU. They suggested that urinary NGAL concentration was useful in predicting the development of AKI in these cases. Moreover, they stated that the maximum urinary NGAL level within the initial 48 hours from ICU admission was significantly associated with the mechanical ventilation dependency length. This association indicated that the NGAL level might reflect the lung injury severity in COVID-19 cases. In this study, NGAL plasma concentrations were significantly higher in pregnant women with severe COVID-19 (90.0 [53.1-207.7] ng/ml) compared to those from pregnant women with non-severe COVID-19 (51.8 [39.6-70.3] ng/ml) and healthy pregnant women (44.3 [32.2-54.1] ng/ml, p<0.001). Also, at a cutoff value of 72 ng/ml, NGAL predicted severe COVID-19 with a sensitivity rate of 57% and a specificity rate of 84%. No patients suffered from AKI in our study cohort. These results provided evidence that the serum concentrations of NGAL in pregnant women with severe COVID-19 are up-regulated and endorse the idea that NGAL is implicated in the development of severe lung infection.
The enhanced production of pro-inflammatory cytokines also ended in activation of the coagulation system and hypercoagulability, which can lead to arterial and microvascular thrombosis.34 Severe COVID-19 cases have increased microthrombi in their lungs and an extensive neutrophil infiltration has been demonstrated in the pulmonary microthrombi of these cases.30 Matrix metalloproteinase -9 (MMP-9), structurally presents in the granules of neutrophils, binds to NETs, induces endothelial dysfunction, and promotes neutrophil migration in the lungs as compensation for viral invasion.35 Neutrophil gelatinase associated lipocalin prevents the inactivation and increases the proteolytic activity of MMP-9.36 Petito et al35 reported that MMP-9 and its MMP-9/NGAL heterodimer were up-regulated in the plasma of COVID-19 cases and both markers were correlated with neutrophil counts in the circulation. They indicated that neutrophil activation more than platelet activation is related to thrombosis in COVID-19 cases. D-dimer value was detected as a powerful independent predictor of severe COVID-19.37 In this study, the median D-dimer value was significantly greater in the severe COVID-19 group (2.2 [1.5-4.8] μg/ml) than that of the non-severe cases (1.7 [1.3-2.3] μg/ml, p=0.009). Also, we found that NGAL and D-dimer levels were independently connected with the severity of COVID-19. We consider that NGAL is a novel and powerful circulating biomarker in predicting severe COVID-19.
Study limitations
We did not confirm the NGAL elevation with the histopathological examination. Larger investigations are needed in which clinical outcomes and maternal serum NGAL levels are proved by histopathological assessment.
In conclusion, we demonstrated that NGAL was highly associated with COVID-19 severity. We consider that NGAL might be a useful biomarker to diagnose the disease severity in patients with COVID-19.
Acknowledgment
The authors gratefully acknowledge Enago (www.enago.com.tr) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 24, 2022.
- Accepted May 17, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.