


Abstract
Objectives: To assess the effect of bupivacaine application following pulsed radiofrequency (PRF) ablation on trigeminal facial pain.
Methods: A total of 73 patients with trigeminal facial pain refractory to conservative therapy were randomized into 2 groups. Group I subjects underwent PRF ablation procedure, followed by the injection of 1 ml of bupivacaine. Whereas, Group II underwent the same procedure followed by the injection of 1 ml of normal saline. Pain relief duration, the time of onset of pain relief, and analgesic effect evaluated by numerical pain rating scale were considered as outcomes.
Results: Thirty-nine patients in Group I and 34 in Group II. The duration of pain relief in the 2 groups was comparable (5 months in Group I vs. 6 months in Group II, p=0.53). The onset of pain relief in the patients of Group I was shorter than Group II (0 days vs. 4.5 days, p<0.001). The binary logistic regression analysis revealed that the application of bupivacaine alone had a significant effect on the reduction of the intake of medications (p<0.05).
Conclusion: In situations involving patients who require rapid pain relief, bupivacaine injection following PRF ablation can be employed to provide immediate relief without subjecting the patients to the risks associated with major complications.
Trigeminal neuralgia (TN) is a rare disease manifested by sudden, recurrent, and short attacks of severe facial pain in relation to the sites of distribution of one or more divisions of the trigeminal nerve.1 The aforementioned episodes of severe pain may occur spontaneously or follow triggering stimuli, which include activities such as combing the hair, talking, brushing teeth, eating, shaving, or even touching the face.2-4 Previous epidemiological studies have reported that the estimated lifetime prevalence of TN ranges from 0.16-0.3%.5-7 The condition is more prevalent in females compared to males.5,6,8,9
The most frequently used medicine for the pharmacotherapeutic management of patients with TN is carbamazepine.10-12 In clinical scenarios wherein the drug therapy fails to provide pain relief or in case of intolerable adverse effects, TN can be treated by means of surgical interventions, such as microvascular decompression, balloon compression, continuous radiofrequency thermocoagulation (CRF), pulsed radiofrequency (PRF), radiosurgery, and other procedures.13-15 Among the aforementioned approaches, CRF is widely used in the treatment of patients with TN and the reported rate of pain relief is 90-100%.16 However, patients who undergo CRF may present with several procedure-related complications, such as facial numbness, penetration of the oral cavity, eyelash hypoesthesia, forehead numbness, corneal hypoesthesia, anesthesia dolorosa, and dysacousis, which are the sequelae of neuronal injury or the surgical procedure.17-21 Conversely, PRF was reported as a minimally invasive, safe, and effective therapeutic option that can be employed for the management of patients with TN.22-25 Pulsed radiofrequency uses the lower temperature generated by means of a radiofrequency generator and the energy is transmitted to the nerves in a pulsatile pattern, in order to generate a neuromodulatory effect, instead of a neurodestructive effect. However, the outcomes of the treatment remain controversial.26-28 In literature, some evidence suggested that microscopic changes occur on the axonal microfilaments and microtubules, which affect the C-fibers to a greater extent, compared to the A-beta or A-delta fibers.29
Moreover, several previous studies have reported the beneficial effects of the application of peripheral nerve blocks with local anesthetic agents to relieve the pain associated with TN.30-32
Furthermore, the authors have noted that in routine clinical practice, the injection of 1 ml of 0.5% bupivacaine after the completion of PRF therapy resulted in immediate pain relief. Literature review did not reveal any previous use of local anesthetic agent at the end of PRF therapy among trigeminal neuralgia patients to relieve their pain. The present prospective, randomized, and double-blind study aimed to assess the effect of bupivacaine injection after PRF therapy on the pain associated with TN. The current study assessed the time of onset and duration of pain relief after the performance of PRF, followed by the injection of bupivacaine.
Methods
Following the principles of the Declaration of Helsinki, a prospective randomized double-blind study was carried out at King Abdulaziz University Hospital, Jeddah, Saudi Arabia. The study protocol was approved by the research and ethics committee of the University Hospital (reference no. 214-20, Dated April 21, 2020). The current study involved the patients with TN who visited the pain clinic during the time period from January 2009 to December 2019. The inclusion criteria are stated as follows: i) patients with orofacial pain who underwent conservative treatment that failed to provide pain relief despite long trial period, or the medications adverse effects were intolerable by the patient, or the patient presented with refractory pain not responding to any pain relieving therapy; ii) age ≥18 years; and iii) diagnosed with trigeminal neuralgia with a neuropathic pain component. The present study excluded the patients who refused to participate in the trial and patients with coagulopathy, hemodynamic instability, tumor, sepsis, hepatic or renal failure, cardiopulmonary dysfunction, mental illnesses, or allergic reactions to the medicines used in the study.
The study design, technical part of the procedure, and possible complications were explained to all the patients prior to the commencement of the procedure and written informed consent was obtained. All patients were randomly assigned to one of the 2 groups by means of computer-generated randomization. The patients in Group I underwent PRF ablation procedure followed by the injection of 1 ml of 0.5% bupivacaine, whereas patients in Group II underwent the same PRF procedure followed by the injection of 1 ml of 0.9% normal saline (placebo). The medications used in the current study were prepared in the pharmacy and both the patient and the physician who administered the treatment were blinded to the details regarding the medicine injected. All the patients included in the current study were under follow-up for a duration of one year after the procedure and the assessment of pain was carried out by a trained research assistant on monthly basis via a phone call. A data sheet was developed to record the rate of change of the numerical pain scale after the procedure, the reduction in the used pain medications, and any complications related to the procedure. The current study employed an 11-degree numerical rating scale (NRS) to assess pain, wherein “0” indicated no pain and “10” indicated the worst imaginable pain.
All the procedures were carried out by the same physician in the operating room under aseptic conditions. The patients were positioned in the supine position with slight head elevation and neck extension. All patients were supplied with oxygen by way of a nasal cannula at the rate of 3 L/minute. Furthermore, intravenous (IV) access was established in all patients and standard monitors were applied. All subjects received 1-2 mg of midazolam IV as an anxiolytic agent. The grounding plate of the radiofrequency generator was placed beneath the ipsilateral shoulder. Subsequently, the skin at the angle of the mouth on the affected side was infiltrated with 1-2 ml of 1% lidocaine. A 10-cm long, 22 G radiofrequency needle with an insulated tip of 2 mm was introduced at a point 1 cm caudal and 1 cm lateral to the angle of the mouth on the ipsilateral side and advanced towards the foramen ovale under image intensifier guidance. The C-arm image intensifier was mobilized in the caudad and ipsilateral directions, in order to obtain a submental view. The location of the needle was confirmed by means of fluoroscopy using the anteroposterior and lateral fluoroscopic views. Subsequently, sensory stimulation of 50 Hz and 0.2 V was used to elicit any pain in the area related to the affected nerve, followed by motor stimulation of 2 Hz and 0.5-1.5 V to generate a muscle twitch of the ipsilateral muscle innervated by the mandibular branch of trigeminal ganglion. Successively, PRF ablation of the associated branch of trigeminal nerve was carried out at 43 °C for 4 minutes using a Neurotherm radiofrequency generator (NT2000, Neurotherm Inc, USA). After the completion of the procedure, 1 ml of bupivacaine/normal saline was administered as an injection.
The patients were kept awake or mildly sedated throughout the procedure, in order to ensure accurate neurological assessment and to confirm the position of the needle. After the completion of the procedure, all patients were transferred to a post-anesthesia care unit for monitoring and detection of any immediate complications.
The data regarding demographic features, disease, and pain score were obtained prior to the commencement of the procedure. The pain score, time of onset and duration of pain relief, and the incidence of any complications were recorded after the procedure. The current study documented any incidence of the following complications: blurred vision, dryness of the eyes, palpitation, vasovagal symptoms, hematoma, infection, fever, nausea and vomiting, dizziness, fainting, or collapse.
Statistical analysis
The data were extracted into an Excel sheet and analyzed using the Statistical Package for the Social Sciences, version 26.0 (IBM Corp., Armonk, NY, USA). All data analyses involved the data pertaining to the intent-to-treat population. The current study employed the last observation carried forward method to impute any missing data. The Kolmogorov-Smirnov test was used to determine if the data regarding outcomes were normally distributed. The Kaplan-Meier test was used to compare the duration of pain relief in the 2 groups and the data are presented as median and 95% confidence interval (CI). The Mann-Whitney U test was used to compare the variations in NRS scores (with p-value associated with the difference) and the time of onset of pain relief in the 2 groups. The data pertaining to the aforesaid outcomes are presented as the median and interquartile range (IQR). The present study employed the Chi-square test to assess and compare the number of patients who displayed post-procedure reduction in the intake of analgesics in each group. In the current study, a p-value of <0.05 was considered significant.
Results
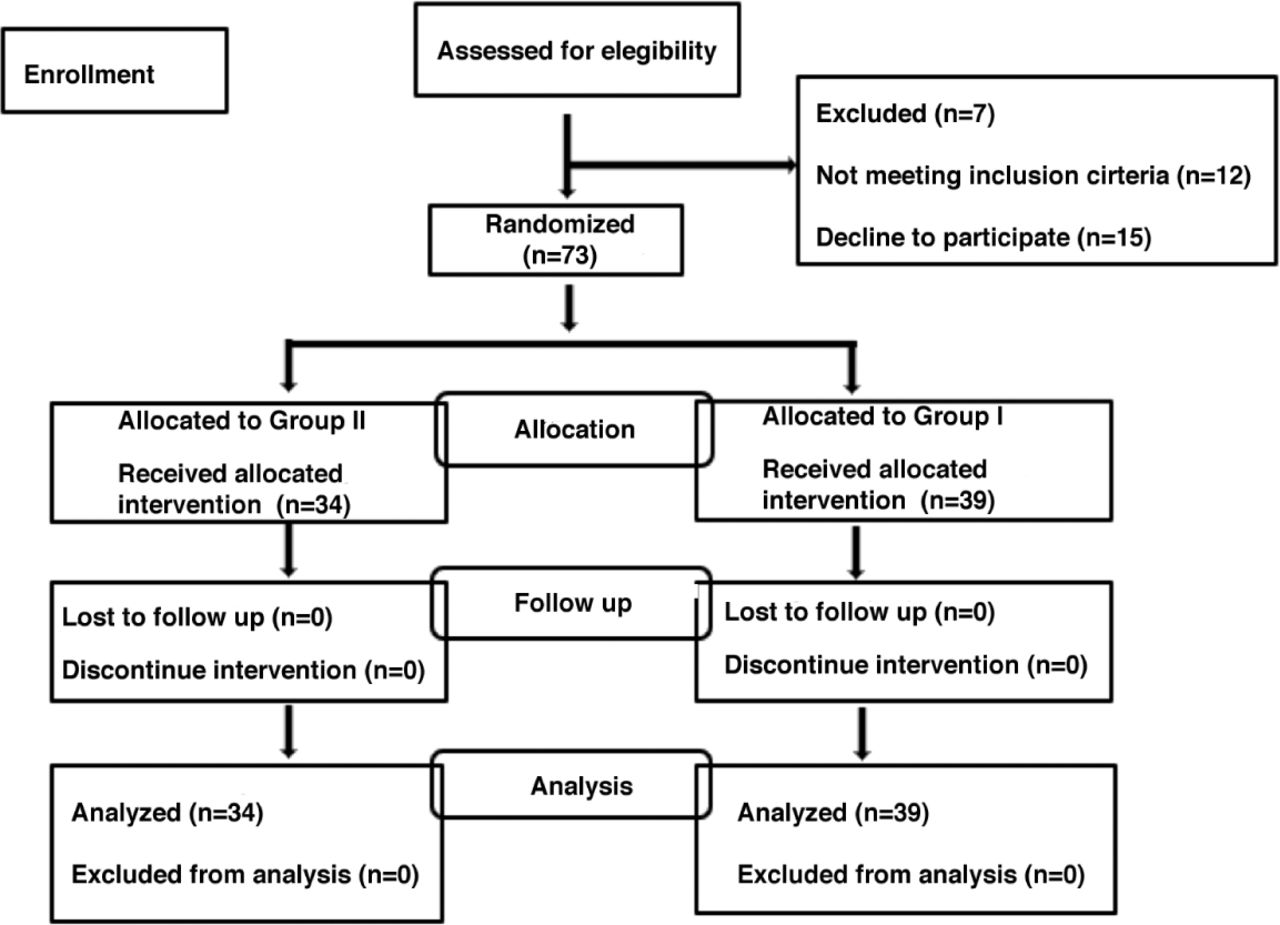
The present study approached a total of 90 potential participants, among which, 12 patients did not meet the inclusion criteria and 5 refused to participate in the study. After the exclusion of the aforesaid 17 patients, 73 patients remained, among which, 39 underwent PRF ablation followed by bupivacaine injection (Group I), and 34 underwent PRF ablation followed by normal saline injection (Group II). All randomized patients were included in the final analysis. A summary of the patient enrollment and study flow is shown in Figure 1.
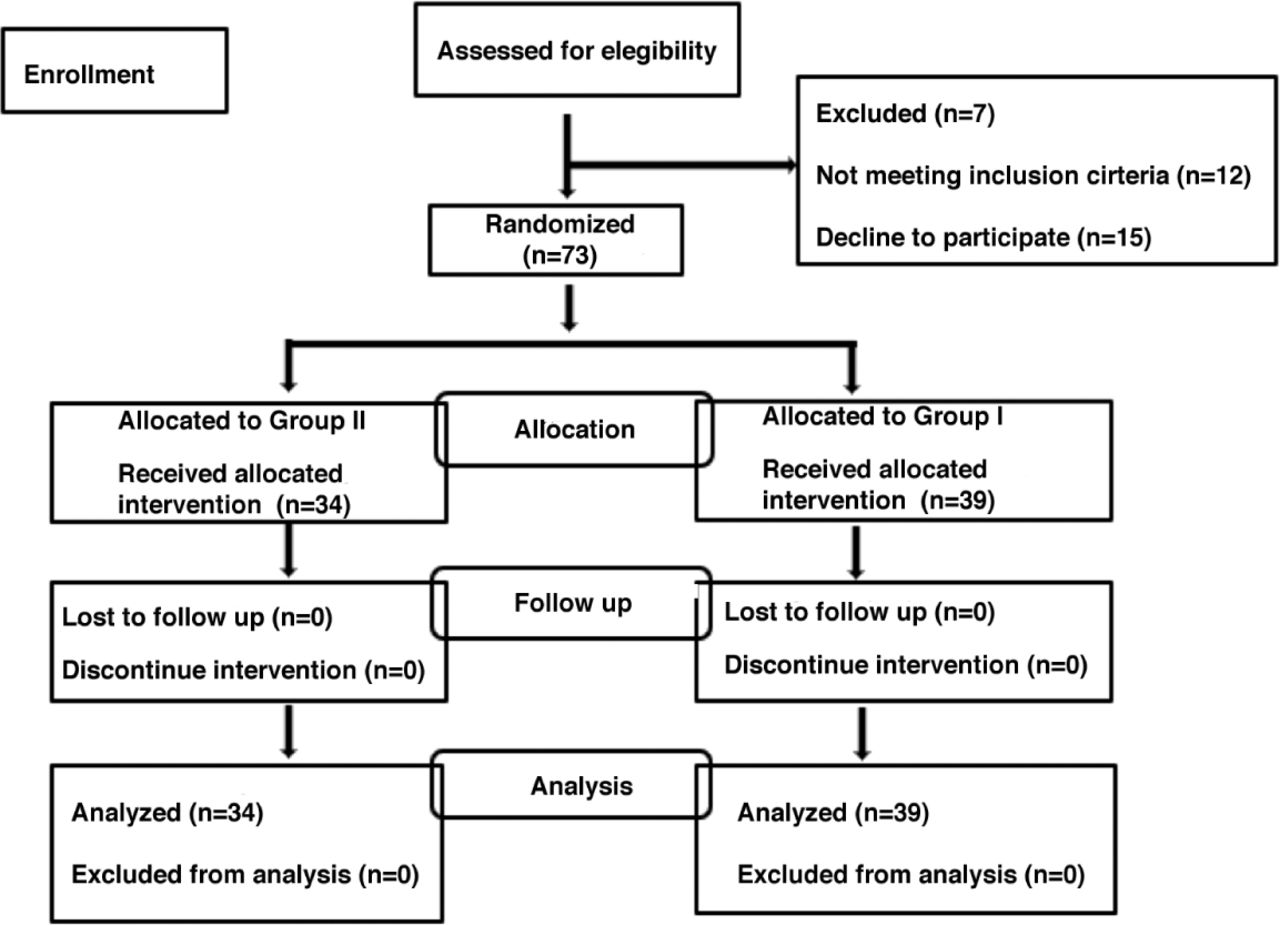
- Consolidated standards of reporting trials (CONSORT) diagram of the trial showing the process of patient enrollment and study flow.
The mean age was 61.33±13.093 years, the mean height was 156.82±13.481 cm, and the mean weight was 68.247±19.282 kg. Female subjects comprised 64.4% of the study population. Among the study subjects, 6 were smokers, 59 were non-smokers, and 8 were ex-smokers. Furthermore, 24 patients had a history of diabetes mellitus, 37 were diagnosed with hypertension, 19 had ischemic heart disease, and 19 had psychiatric disorders. Among the study subjects, 42 patients had undergone dental procedures (Table 1).
- Characteristics pertaining to the patients in both groups.
In the current study, a majority of the subjects were diagnosed with trigeminal neuropathic pain (90.4%), while the remaining patients (9.6%) were diagnosed with trigeminal neuralgia. Moreover, the condition affected the right side in most of the patients (53.4%). In a majority of the patients, both the V2 and V3 divisions of the trigeminal nerve were observed to be affected (43.8%), whereas the V2 division alone was affected in 35.6%, and V3 division alone was affected in 16.4% of patients (Table 2).
- The features of pain pertaining to all the subjects.
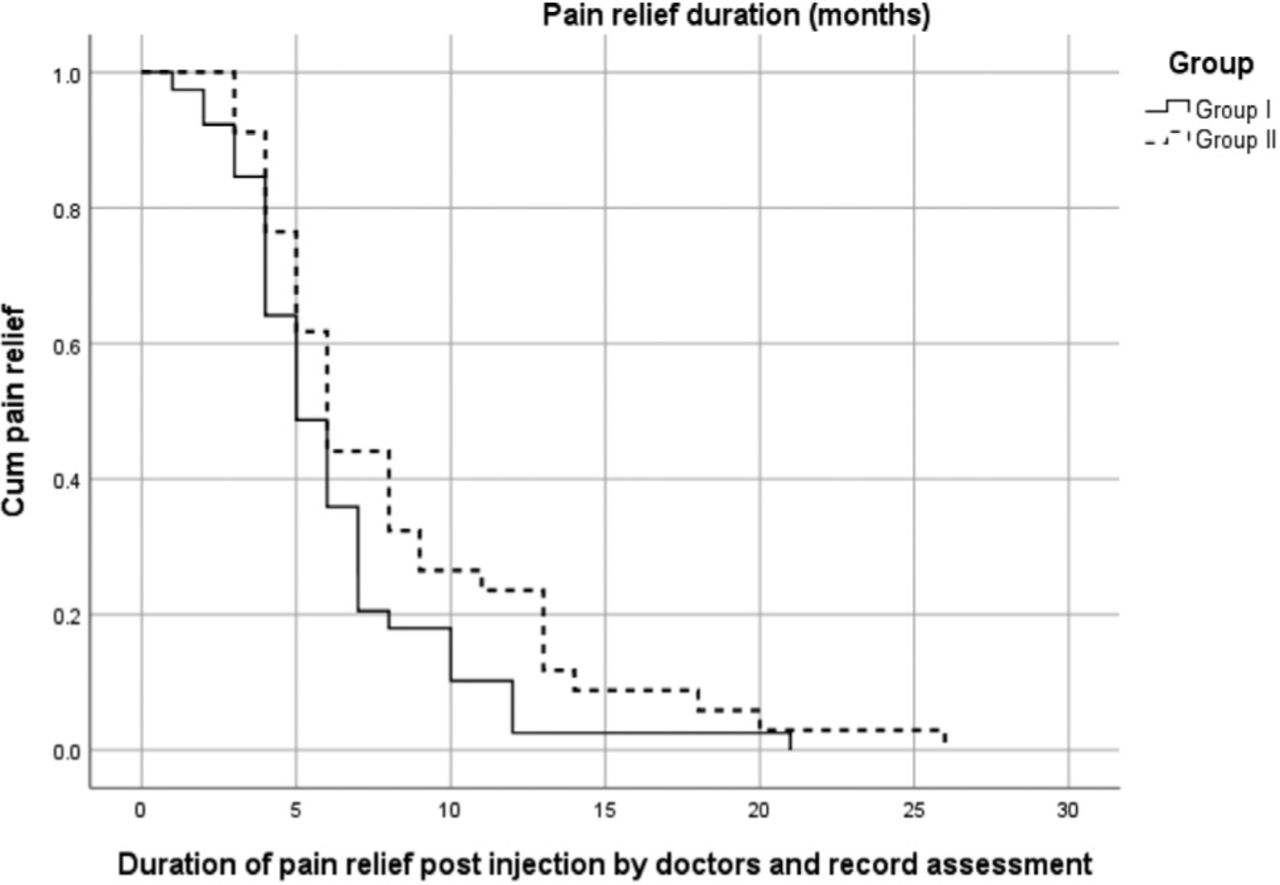
The median duration of pain relief in Group I and Group II are presented in Figure 2. We did not observe any statistically significant difference between the 2 groups, in regard to the duration of pain relief (p=0.53).

- Kaplan-Meyer analysis of the duration of pain relief.
In the present study, the pain score pertaining to the subjects prior to the commencement of treatment ranged from moderate to severe (4-9) on the NRS scale. However, all the patients displayed marked pain relief after treatment (NRS= 0-3), with the exception of one patient in Group II who displayed a score of 4 on the NRS scale. The median variation in the NRS scores in Group I was -5 (IQR= -6 to -5) and in Group II was -5.5 (IQR, -6 to -4), and difference between the 2 groups was not observed to be statistically significant (p=0.815).
The median time of onset of pain relief in Group I was zero days (immediate effect), whereas the onset of pain relief in Group II was 4.5 days (IQR=3-7). The current study observed significant difference between the 2 groups in regard to the time of onset of pain relief (p<0.001).
Upon asking the patients regarding their pain after the interventions, two-third (63.8%) of the subjects experienced good or excellent level of pain relief and mild relief was reported by slightly more than one-third (36.2%) of the patients. Among the subjects, a significantly greater percentage of females expressed good to excellent pain relief, compared to males (79.1% vs. 20%, p<0.05). Moreover, the percentage of good or excellent pain relief was higher among non-diabetic patients, compared to diabetic patients (p=0.053). Although the percentage of patients with good or excellent pain relief was higher among the subjects ≤50 years of age, patients with normal body mass index or hypertension, and those who did not receive bupivacaine, these differences were not observed to be statistically significant (p>0.05).
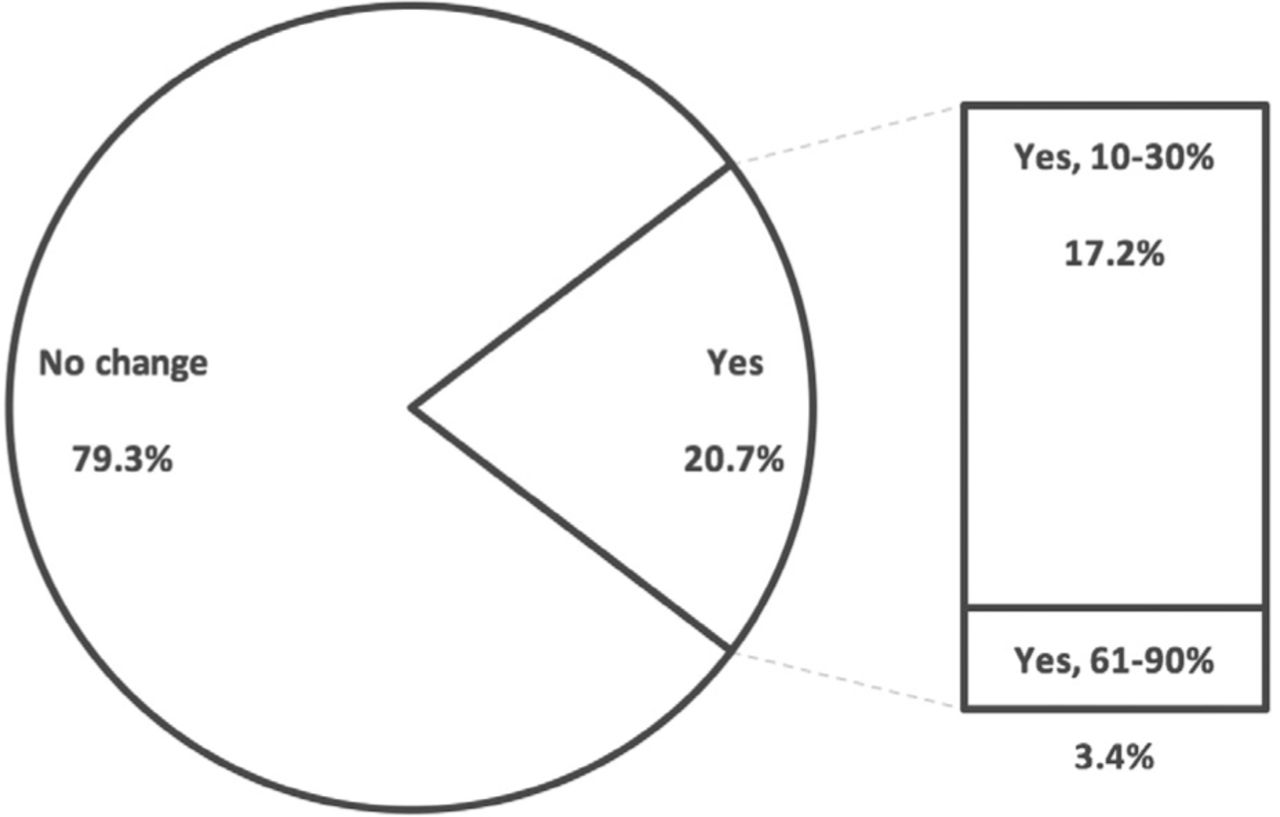
Considering the requirement of post-procedure alteration in the dosage of medications, a majority of the subjects (79.3%) were apprehensive regarding the reduction of dosage of medicines, whereas the dosage was reduced by 10-30% in 17.2% of the patients and by 61-90% in 3.4% of the patients (Figure 3). The binary logistic regression analysis to identify the predictors associated with the reduction in dosage of medications in patients with trigeminal facial pain revealed that only the application of bupivacaine had a significant effect (p<0.05) with an exponential B of 7.778, which indicated that bupivacaine injection after PRF ablation increased the chance of post-procedure reduction in the dosage of medications by approximately 8 times, compared to other factors (Table 3).
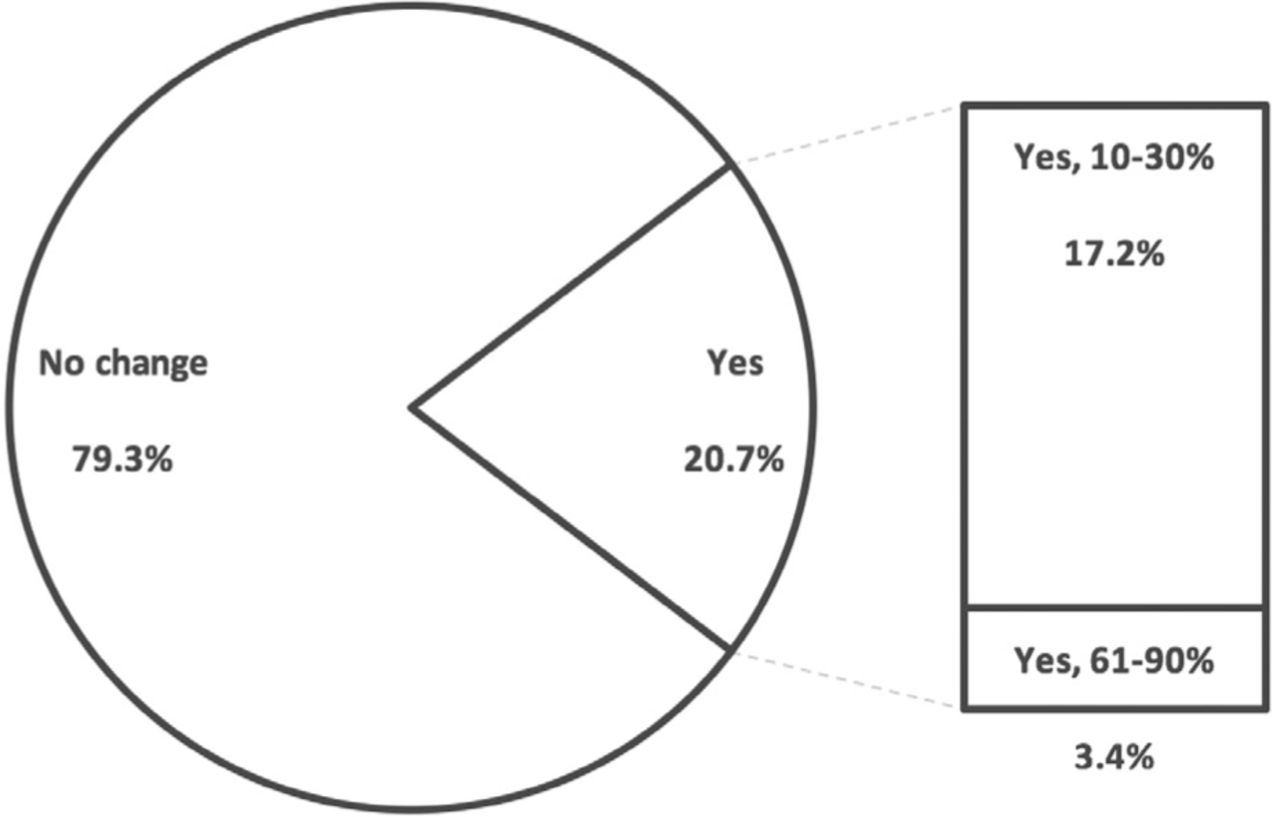
- The alteration in the dose of medications post-procedure according to the study subjects. Percentage: indicates the use of pain medications after the procedure among the study subjects
- The binary logistic regression analysis to identify the predictors associated with the reduction in dosage of medications.
In the present study, none of the subjects displayed any procedure-related complications or adverse effects related to the medications administered.
Discussion
The accelerated onset of pain relief and reduction in the dosage of prescribed medications without any effect on the duration of pain relief in patients who received bupivacaine injection after the completion of PRF therapy were the key findings of the present study.
Radiofrequency ablation is an ablative surgical technique used to treat patients with trigeminal pain. Although CRF offers better results regarding pain relief, compared to PRF, the latter is increasingly being used, owing to the less destructive nature of the technique and fewer side effects.22-25,33,34
In the present study, the use of PRF was preferred, in order to limit any procedure-related complications and to facilitate the accurate assessment of the effects of bupivacaine injection. A recent systematic review has reported that RF ablation was effective in the management of chronic facial pain.35 The aforementioned review stated that RF therapy provided pain relief, improved the quality of life, and resulted in decreased consumption of oral medications.35 Several previous studies have reported that high-voltage PRF is a more efficient method that can be employed to provide pain relief and reduce the intake of medications.23,36 The current study endeavored to use PRF, and the temperature was limited to 43°C, which might lead to higher rates of recurrence of pain. The aforesaid possibility was concurrent with the results reported by Yao et al37,38 in 2 previous studies that reported that higher postsurgical recurrence rates were observed in relation to treatment regimens that involved lower temperatures.
A systematic review by Orhurhu et al35 reported that patients with chronic facial pain who underwent CRF procedures displayed immediate pain relief, ranging from 89-99%. Furthermore, a study by Xue et al39 reported similar findings of immediate pain relief with radiofrequency thermocoagulation (visual analog scale [VAS] score of 0) in 88% of the subjects. However, a review of literature did not reveal any randomized controlled study involving the use of PRF that reported immediate relief from facial pain. The technique used in the present study is a novel method that can be used to provide immediate pain relief without subjecting the patients to the risks of any major complications.
Local anesthetic agents have been used either alone or in combination with steroids for the management of several patients with trigeminal pain in clinical situations that warranted the same.40,41 Bupivacaine is a long-acting anesthetic agent that has been used to administer nerve blocks for several decades. In addition, 2 recent studies employed bupivacaine alone to control the pain associated with TN in patients in whom invasive procedures were not indicated and reported that bupivacaine provided the patients with significant pain relief.42,43 However, in the management of TN, the duration of pain relief associated with nerve block was shorter, compared to PRF therapy.44 Hence, the situation warrants future clinical trials, in order to assess the efficacy of bupivacaine injection after CRF therapy, combined CRF and PRF therapy, or the application of PRF for a duration of 360 seconds or longer, and to estimate its effect on the onset and duration of pain relief TN cases. A previous study by Tanaka et al45 observed that increasing the duration of application of PRF from 120-360 seconds resulted in a significant antiallodynic effect without nerve injury in rats. Additionally, a retrospective study by Eissa et al46 reported that a combination of PRF at 45 °C for 12 minutes followed by CRF at 60 °C for 2 minutes, and 65 °C for 2 minutes could achieve excellent pain relief and significantly reduce the consumption of analgesics in patients with idiopathic TN.
Moreover, an additional advantage of the technique employed in the present study is the post-procedure reduction in the dosage of medications. The abovementioned advantage was reported by several previous studies that reported that the application of CRF and PRF were associated with significant reduction in the dosage of medications.23,36 However, further studies are required to identify the primary reason regarding the post-procedure reduction in the dosage of oral medications, regardless of the application of PRF or injection of local anesthetic agent.
Study limitations
Concurrent with the parameters used in previous studies, the present study assessed the degree of pain relief, incidence of complications, and other subjective indicators of pain, while the objective indicators were not considered. Electrophysiological examination may provide further information regarding the changes in neurological function of the trigeminal nerve, which might be affected by PRF, the injection of a local anesthetic agent, or both. The current scenario warrants further studies and clinical trials to ensure accurate understanding of the same.
In conclusion, bupivacaine injection following PRF ablation can be employed to provide immediate relief from trigeminal facial pain without subjecting the patients to the risks associated with major complications.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 28, 2022.
- Accepted May 11, 2022.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.