


Abstract
Objectives: To evaluate LDL-C control in patients within 6 months after hospitalization for ACS in Saudi Arabia.
Methods: This multicenter, prospective, observational registry evaluates LDL-C control in patients within 6 months after hospitalization for ACS in Saudi Arabia between December 2017 and October 2019. The study aimed at recruiting 170 patients and data were collected retrospectively at baseline and prospectively at 2 subsequent visits.
Results: 201 patients were included at baseline, 193 completed the 3-month visit and 186 completed the 6-month visit. Post-ACS, virtually all patients were prescribed high-intensity statins and LDL-C levels decreased consistently. However, at LDL-C target assessment, 57.1% of patients still had LDL-C levels >55 mg/dL, while 62.6% of patients had achieved LDL-C level decrease ≥50%. The composite milestone of LDL-C decrease ≥50% and LDL-C levels <55 mg/dL was met by 20.6% of study patients. Importantly, 37% of patients did not have LDL-C reading post-ACS and the primary outcome was only valuable for 126 out of 201 patients (63%).
Conclusion: Levels and decrease of LDL-C from baseline achieved in this study are suboptimal, according to updated 2019 ESC/EAS guidelines. While statins were prescribed to all patients post-ACS, the recommended add-on treatments were largely overlooked. Gaps in dyslipidemia management linger, despite clear updated guidelines.
Elevated cholesterol levels are causal to the development of atherosclerosis, a long-established risk factor for cardiovascular disease (CVD).1-6 For decades, the long-term, multigenerational, ongoing Framingham Heart study associated the low-density-lipoprotein-cholesterol (LDL-C) with increased risk for CVD.1,7 The importance of lowering LDL-C levels is reflected in the updated European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS) prevention guidelines, where target LDL-C was 1.8 mmol/L (70 mg/dL) in 2016, whilst in the 2019 ESC/EAS guidelines, targets were brought down to a maximum of 1.4 mmol/L (55 mg/dL).8,9 The solid evidence implicating LDL-C levels with CV health motivates lipid-lowering therapy (LLT), ideally with lifestyle changes, for primary or secondary CVD prevention. Lipid-lowering therapys encompass several therapeutic classes: statins, fibrates, cholesterol absorption inhibitors (notably ezetemibe), proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors and others.10 The ESC/EAS and the American College of Cardiology (ACC)/American Heart Association (AHA) recommend statins, ezetemibe and PCSK9 inhibitors as major LLTs.10-13 Statins are the mainstay of pharmacological LLT, and should be offered to all patients with elevated LDL-C levels at high CV risk and who tolerate them.10,13 Statins work majorly by inhibiting the 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase, thus suppressing cholesterol biosynthesis. They also modulate small G protein activity, suppress pro-inflammatory mediators, and induce endothelial nitric oxide synthase, which is of particular interest in atherosclerotic CVD.14
Despite the efficacy of available LLT, achieving LDL-C targets remains a challenge.7,10 Among acute coronary syndrome (ACS) patients participating in the EUROASPIRE V survey across 27 European countries and receiving high-intensity LLT, only 32.3% of male patients and 23.1% of female patients achieved LDL-C targets of 1.8 mmol/L (70 mg/dL), at least 6 months into their treatment.15 A 2021 randomized controlled found that only 49.6% of post-ACS patients had achieved the target (LDL-C <70 mg/dl or 50% reduction from baseline) at one year in the group offered treatment adherence reinforcement, compared to 44.9% in the group on pharmacological LLT only.16
In a recent real-world study of 47,884 patients, only 50% had LDL-C levels measured within 6 months after percutaneous coronary intervention (PCI) and only 57% had LDL-C levels <70 mg/dL.17 In addition, higher levels of LDL-C were associated with increasingly higher rates of CV events, after a 3-year follow-up period.17
In the Arabian Gulf, data on LDL-C target attainment are scarce, but point at a suboptimal target achievement. A search on PubMed was performed to identify papers on ACS in Saudi Arabia and the Arabian Gulf) and only relevant manuscripts were retained. In 2014, the DYSIS-Middle East study reported that around two-thirds of statin-treated patients in Saudi Arabia and other Arab countries had poorly controlled lipid levels.18 In Saudi Arabia, only 24.3% of patients with coronary heart disease (CHD) and 11.4% of patients with acute coronary syndrome (ACS) achieved LDL-C targets in 2018.19 The STARS-1 Program in 2019 revealed a suboptimal management of ACS in Saudi Arabia, in terms of revascularization, pharmacological LLT or use of emergency medical services.20 Evident shortcomings in post-ACS clinical care and limited data on LDL-C management post-ACS globally and in Saudi Arabia, motivated the Acute Coronary Syndrome Management (ACOSYM) study (Prospective Observational study of Lipid Management in Non-US, Nonwestern European Patients Who Have a Recent Acute Coronary Syndrome Event) to better depict ACS patient profile, the status of LDL-C level control and the implementation of intensive statin-based LLT for post-ACS patients in real-world clinical practice.18-20 The global study has been published and the current paper reports on the Saudi Arabian situation.21
Methods
The ACOSYM study was a prospective, observational, multicenter study that recruited patients admitted for ACS in the 12 weeks leading up to baseline visit, to report on their real-life management. Patient data were collected retrospectively at the baseline visit (Visit 1) and prospectively at Visit 2 (3 months ± 2 weeks) and Visit 3 (6 months ± 2 weeks), according to routine follow-up. Data from patient medical records were entered onto a study-specific Electronic Data Capture (EDC) form.
Patient surveys were administered at the baseline visit and during the 3-month and 6-month follow-up visits; by a person delegated by the investigator, who collected data from the patient through a face-to-face or a telephone interview. The patient survey tool was designed to capture the precise/verbatim responses of the patients using closed-ended questions. The study took place in Saudi Arabia between December 2017 and October 2019 (22 months). All patients provided informed consent, before any study-related activities. Ethics Committee’s approval was obtained from King Saud University (approval number E18/0466/IRB), Saud Al Babtain Cardiac Center – Dammam (approval number IRB-2018-12), King Khaled Medical City (approval number MED0240) and King Fahed Medical City (approval number 18-455), prior to any study-related activities, which were carried out according to the Declaration of Helsinki.
Patients admitted to the hospital for ACS were evaluated for eligibility to participate in the ACOSYM study (Table 1). Consecutive patients fulfilling eligibility criteria were included in the study by participating cardiologists. The study aimed at recruiting a total of 170 patients.
- Eligibility criteria for enrolment in the Acute Coronary Syndrome Management study.
Operational definitions of major variables
Cholesterol control was described in terms of LDL-C levels and target level achievement. The primary objective of the study was to describe the proportion of post-ACS patients reaching the following four LDL-C targets over 6 months: <130 mg/dL, <100 mg/dL, <70 mg/dL and <50 mg/dL. It was reported for all eligible patients with at least one LDL-C test result during the follow-up period. The last available LDL-C value within the 2 years leading up to study entry was used as a baseline value and the last available LDL-C value in the follow-up period was used at the 3-month and the 6-month data points.
Secondary objectives described the LLTs prescribed to patients with ACS, the proportion of statin-intolerant patients and potential barriers to achieving LDL-C targets.
In line with the 2019 ESC/EAS recommendations of achieving at least 50% decrease in LDL-C levels and meeting the target LDL-C below 55 mg/dL, data from this study were further analyzed to reflect on the subset of patients achieving the recommended LDL-C target post-ACS.
Statistical analysis
Categorical variables were summarized as the counts and percentage of patients in each category. The count of missing observations was provided. In addition, a 2-sided 95% confidence interval (CI) was presented for percentages, when relevant. Continuous variables were summarized using the mean, standard deviation (SD), median, first and third quartiles (Q1, Q3), minimum, maximum, and the number of non-missing and missing observations. Statistical analysis was conducted using SAS® Software, Version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
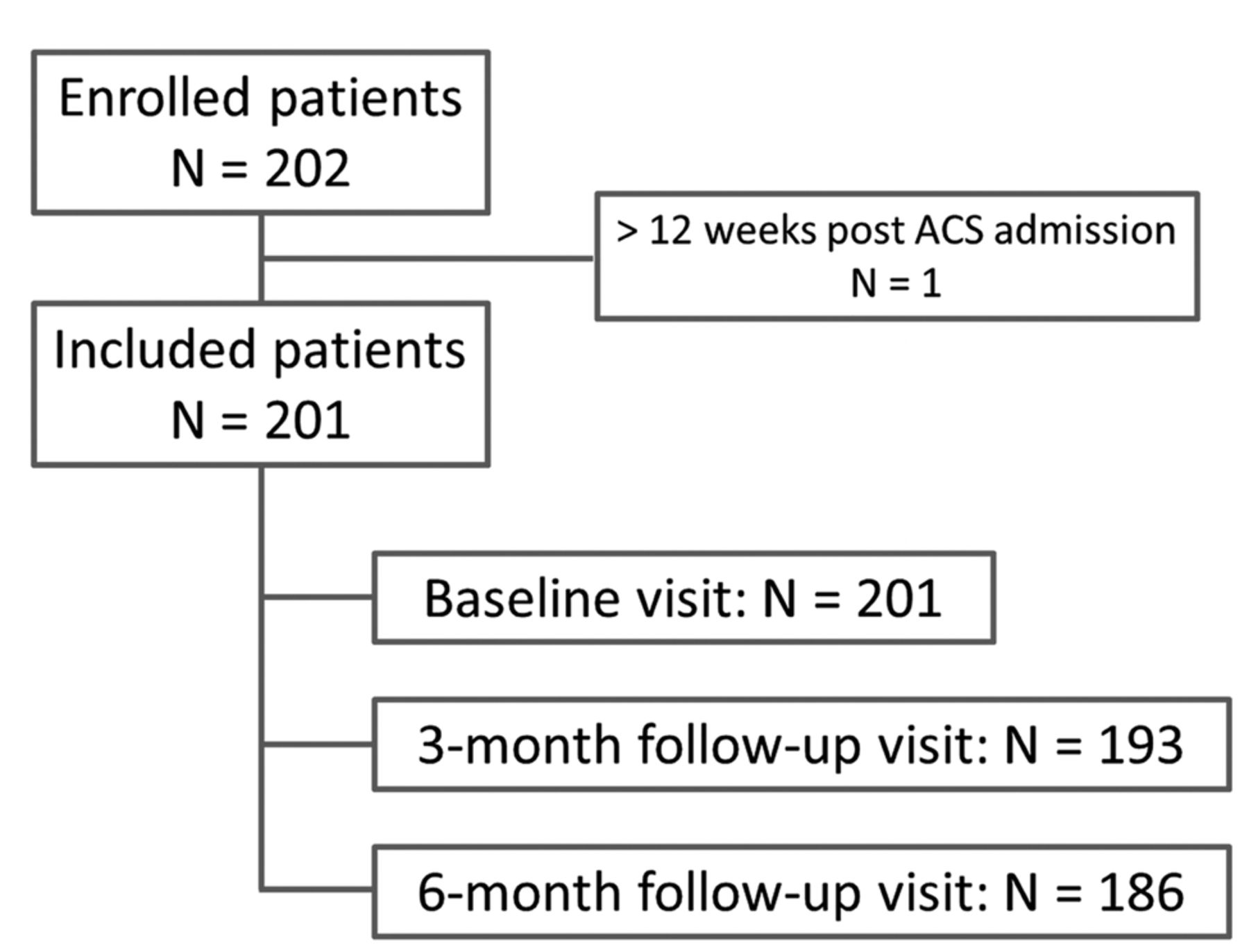
On average, the 201 patients were enrolled in the study 0.9±2.2 weeks after their admission for ACS and the large majority (93.5%) was discharged on the day of the baseline visit. Symptoms of ACS included ST-segment elevation myocardial infarction (STEMI) in 104 (51.7%) patients, non ST segment elevation myocardial infarction (NSTEMI) in 74 (36.8%) patients and unstable angina in 23 (11.4%) patients. Emergent PCI was performed in 76% of cases, mostly involving drug-eluting stents. Out of the 201 patients included, 186 completed the study. Patients were recruited by 4 investigators across 4 study sites, of which one Ministry of Health center (88 patients), one university hospital (70 patients) and 2 government institutions (17 and 27 patients). There were 15 discontinuations due to death (5 cases due to cardiac arrest [n=2], cardiac failure [n=1], pulmonary edema [n=1], and indeterminate cause [n=1]), loss to follow-up (9 cases) and patient’s wish for discontinuation (1 case). Figure 1 summarizes patient disposition in this study.

- A total of 201 patients were included for analysis. One patient did not meet the inclusion criterion of enrolment within 12 weeks of admission for ACS and 15 patients discontinued the study since their baseline visit. ACS: acute coronary syndrome
Baseline characteristics
The enrolled population was between 26 and 84 years of age (with an average of 54.4±11.1 years and a median of 55). Over 3 quarters of the patients were below 65 years of age (82.6%). The vast majority were male patients, with only 19 (9.5%) female patients; of whom 15 were not of childbearing potential due to menopause (86.7%). Medical history, anthropometry (weight and height), vital signs and blood sugar and lipid profile were reported for study participants (Table 2). Among the 107 patients with type-2 diabetes (average glcated hemoglobin 8.7%±3.9), 48.6% were on insulin.
- Baseline characteristics of the patients (N=201).
Analysis of the primary objective
A total of 126 (62.7%) patients were evaluable for the primary objective, as they had one or more LDL-C measures available during the follow-up period. The percentage of patients reaching the different LDL-C targets is given in Table 3. Time from ACS admission to LDL-C target achievement assessment ranged between 3 and 42 weeks, with an average of 21.7±7.9 weeks. All measurements happened after discharge. Low-density-lipoprotein-cholesterol levels went down from 115.8±46.5 mg/dL at baseline to 69.0 ± 33.4 mg/dL at target achievement assessment (p<0.001). Importantly, levels were also down by 39.2% ± 29.5% at the 3-month visit (Visit 1, p<0.001) and by 31.9%±37.5% at the 6-month visit (Visit 2, p<0.001). Counts and frequencies of patients achieving LDL-C levels between 55 and 70 mg/dL on the one hand and below 55 mg/dL on the other hand were calculated as part of a post hoc analysis. Importantly, 26 out of 126 patients (20.6%) achieved the composite target of a LDL-C decrease ≥50% and LDL-C levels <55 mg/dL.
- Low-density-lipoprotein-cholesterol (LDL-C) levels throughout the study (N=126).
Analysis of secondary objectives. Patient medical status in the follow-up period
A total of 9 patients (4.5%) experienced at least one ACS recurrence after the initial ACS admission, 5 of which due to NSTEMI, 1 due to STEMI and 3 to unstable angina. Importantly, 7 out of the 9 recurrent ACS occurred within the initial 3-month period after initial hospitalization for ACS.
At the 6-month visit, the proportion of patients who had consulted with a heart specialist or cardiologist since the previous visit was 48.5%. At the time of LDL-C target achievement, 71.4% of patients had used healthcare resources related to ACS, 84.4% of which at the outpatient department.
Use of statins in the Saudi patient population
Statin use was reported for patients participating in the study. Table 4 displays the proportion of patients on statin-based LLT before their ACS, at their discharge from the hospital (baseline) and in the follow-up period. Before their ACS, only 58 out of 201 (28.9%) patients had been on statins. Before their discharge from the hospital upon ACS admission, almost all patients (200/201 [99.5%]) were prescribed statins, of whom 194 (97%) were prescribed high-intensity statins. From the population who was evaluable for the primary objective (N=126) of achieving LDL-C targets within 6 months, 124 (98.4%) patients were on statins. Noteworthy, only 17 (8.5%) patients were prescribed other LLT at discharge (selective cholesterol-absorption inhibitors [15 patients], nicotinic acid [1 patient] and fibrates [2 patients]); and at LDL-C target assessment, only 12 patients were on a LLT besides statins.
Description of lipid profile throughout the study
Figure 2A shows lipid profile (HDL-cholesterol, LDL-C, total cholesterol and triglycerides) in the 2 years leading up to the ACS event, at the study baseline (post-ACS) and in the period leading up to LDL-C target achievement. At LDL-C target achievement, HDL-cholesterol levels were 39.3±9.86 mg/dL and triglyceride levels increased by 7.6 mg/dL. At the time of target assessment, most patients had LDL-C levels below 100 mg/dL, and 42.9% had LDL-C levels below 55 mg/dL; but some still maintained higher levels (Figure 2B). Almost all patients were prescribed the most common CV medications after their ACS, compared to modest medication use for CV prevention (pre-ACS), as shown in Figure 2C.

- LDL-C levels at target assessment. A total of 126 patients had at least one LDL-C value at the time of target achievement assessment. A. Change in lipid profile parameters over time (Pre-ACS n=33, Baseline n=115, At target assessment n =126). B. Distribution of the 126 patients across LDL-C categories at the time of target achievement assessment. C. Number of patients on the major medications reported pre-ACS, at baseline and at the time of target achievement assessment. ACEI: angiotensin-converting enzyme inhibitors, ACS: acute coronary syndrome, ARB: angiotensin II receptor blockers, HDL-C: high-density lipoprotein cholesterol, LDL-C: low-density lipoprotein cholesterol, NSAIDs: non-steroidal anti-inflammatory drugs
Treatment landscape among patients achieving the composite milestone LDL-C target below 55 mg/dL and 50% LDL-C decrease from baseline
At baseline, 9 (7.8%) patients had LDL-C levels <55 mg/dL, increasing to 41 (44.1%) patients at month 3 and then down to 32 (42.1%) patients at month 6. Overall, 54 (42.9%) patients achieved LDL-C levels below 55 mg/dL throughout the study. However, the 2019 ESC/EAS composite milestone of LDL-C levels below 55 mg/dL AND a 50% LDL-C decrease from baseline was achieved by 26 out of 126 (20.6%) patients.
All study patients were prescribed statins at baseline. In addition, patients achieving the composite milestone were also prescribed salicylate NSAIDs n=26 (100%), antiplatelet medications n=26 (100%), beta-blockers n=22 (84.6%), angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers n=20 (76.9%) and cholesterol-lowering medicines besides statins n=3 (11.5%). Frequencies of patients prescribed the aforementioned treatment cocktail came as follows: 13 (50%) at baseline, 19 (73.1%) at the 3-month visit and 16 (61.5%) at the 6-month visit.
Profile of patients not evaluable for the primary objective
A total of 75 patients (37.3% of the study population) did not have follow-up LDL-C values and were therefore not evaluable for the primary objective of the study. Demographic, education, and family status data, as well as LDL-values recorded at baseline were not significantly different between the 2 populations (the 126 patients evaluable and the 75 patients not evaluable for the primary objective). On the other hand, a difference was identified between these 2 populations when it came to ACS admission and management. A significantly higher percentage of patients in the non-evaluable population received emergent thrombolysis at ACS admission (25.3%), compared to the primary objective population (13 [10.3%]), p=0.005. Additionally, 81 out of 126 patients and 50 out of 75 patients underwent PCI for stent placement during hospitalization and the type of stent was significantly different between the two populations (p<0.001): 77 patients (95.1%) evaluable for the primary objective had a drug eluting stent, compared to 28 out of 75 patients (56.0%) constituting the non-evaluable population. The stent type for the latter group was reported as “unknown” for 22 patients (44.0%).
Patient perception about ACS and statin intake
Similar proportions of patients pre-ACS and post-ACS believed their cholesterol levels were high (26.5% and 25.9%), but almost twice as many patients got tested post-ACS (35.1%) than pre-ACS (18.4%). A large proportion of patients (83 [43.7%]) reported never worrying about the risk of ACS recurrence, with 27.6% saying that preventing another ACS event was out of their control. Although 26.4% believed they were at high risk for CV events, 68.6% do not associate high cholesterol levels with increased risk of ACS. Among statin users, 14.6% reported experiencing symptoms of statin intolerance at baseline and 8.7% at the 6-month visit. However, 119 patients (64.0%) seem to believe that statins would alleviate the risk of ACS, and 106 patients (57.0%) thought that statins were safe.
Patients reportedly obtain information on cardiac medication mostly from their treating physician (165 [83.8%]). However, large proportions of patients answered with “I do not know”, reflecting gaps in awareness and knowledge about their condition.
Discussion
The Saudi Arabia chapter from the global ACOSYM study evaluated LDL-C level evolution, statin use and patients’ general perception of their CV condition. In accordance with other studies, the male gender prevailed among ACS patients; similar to the 2009 SPACE registry reporting that 77% of ACS patients were men in Saudi Arabia.25 In 2011, high prevalence rates of diabetes (40%), hypertension (49%), dyslipidemia (32%), smoking (38%), and obesity (27%) were reported among ACS patients in the Gulf region.26 In the current study, 74% of ACS patients suffered from overweight/obesity, 54% had hypertension, 53% had diabetes, and 42% were smokers, in line with recent literature. Compared to the 1500 patients included in the global ACOSYM study, smaller proportions of Saudi patients had hypertension, family history of stroke or myocardial infarction, coronary artery disease and heart failure; but a much greater proportion of them had diabetes.21 These conditions, together with dyslipidemia, are proven traditional CV risk factors, known to manifest before the occurrence of the CV event and to benefit from timely management.27-29 In particular, average total cholesterol and LDL-levels were highest within the 2 years leading up to the ACS, and lowest at the 6-month target achievement data point. At baseline, all patients were prescribed high-intensity statins (97%), but alarmingly, over 60% of patients were not on statins pre-ACS. The prevalence of these CV risk factors is comparable to data reported in a 2009 study that underscored a time lag between availability of clinical evidence and its translation into ACS care in Saudi Arabia.25 Unfortunately, the ACOSYM study confirms this gap in CV management and ACS prevention, since large proportions of patients experiencing ACS presented with CV risk factors that frequently occur in clusters.30
This study also looked at the patients’ health perception. Over 40% of ACS patients in this study did not identify themselves at risk for ACS recurrence although over 70% of them required ACS-related care in the study follow-up period. In fact, a recent study reported that up to 63% of 18,924 ACS cases had a recurring event, due to prior atherosclerotic CV events and multiple high-risk conditions, including residual dyslipidemia despite maximum tolerated statin.31 In that study, patients largely benefited from the addition of a PCSK9 inhibitor to their statin prescription, further highlighting the modest treatment of dyslipidemia pre-ACS reported in this study, and sometimes despite the physician’s advice.31
Noteworthy, LDL-C levels consistently decreased after statin introduction and only a small percentage of patients sustained LDL-C levels beyond 100 mg/dL at 6 months. During the study, about 33% of post-ACS patients achieved LDL-C levels below 50 mg/dL and 61% had levels <70 mg/dL, similar to the global study population and to a 2020 study that reported that 57% of patients had LDL-C <70 mg/dL.17 At LDL-C target achievement, 63% of patients had at least a 50% reduction from baseline LDL-C.21 Of particular importance, the 2019 ESC/EAS guidelines aim for the composite milestone achievement of LDL-C level decrease ≥50% AND LDL-C levels below 55 mg/dL.9 In the current study, around 21% of patients met this updated composite milestone, despite being all prescribed statins post-ACS. Moreover, the 2019 ESC/EAS guidelines call for LDL-C goals <40 mg/dL for patients with recurrent ACS within 2 years of highest tolerated dose of statin therapy.9 The ACOSYM study started recording ACS recurrence (among 4.5% of patients) within 3 months of initiating statins and around 40% of patients had no LDL-C reading in the follow-up period, pointing at major shortcomings in ACS management in Saudi Arabia. In the STARS-1 Program in 2019, recurrent myocardial infarction was reported in 79 (3.54%) of the 2233 patients, before hospital discharge; of whom 31 with ST-segment elevation myocardial infarction (STEMI) and 48 non-STEMI (NSTEMI). Additionally, after one-year follow-up, patients with NSTEMI had higher mortality rates than patients with STEMI (7% and 3.8%, respectively, p<0.05).20 Updated ESC/EAS guidelines now recommend a PCSK9 inhibitor as a statin add-on treatment in post-ACS patients not achieving LDL-C goals after 4-6 months on maximal tolerated statin therapy and ezetemibe.9 Alarmingly, a very small proportion of Saudi Arabian patients in the ACOSYM study were prescribed another LLT, yet another gap in dyslipidemia management. This trend has been reported in the literature, despite the availability of treatments.32
Collectively, data from this study, supported by the available literature on CV health in Saudi Arabia, point at suboptimal management of dyslipidemia in the country, from modest use of statins, to misconceptions about ACS risk and recurrence, and unassertive measures taken to control risk factor clusters. Noteworthy, clinical inertia and the reluctance to observe updated practice guidelines in the management of dyslipidemia and ACS have prompted several groups to publish position and practical guidance papers to strengthen the management of dyslipidemia and other risk factors, for the prevention of CV events in patients with prior CV events and patients at high and very high risk.10,33,34 Widespread clinical inertia indeed calls for more aggressive treatment of high LDL-C, strict control of CV risk factors, the early prescription of multiple LLT in dyslipidemia treatment, and the straightening out of misconceptions related to chronic statin use.33-37
The relatively small sample size might not fully reflect the extent of unmet needs in terms of post-ACS management in Saudi Arabia, but results confirm previous studies reporting on healthcare gaps in mitigating the CV risk in general, and dyslipidemia in particular in Saudi Arabia. Indeed, the under-diagnosis and under-treatment of dyslipidemia in Saudi Arabia have already been reported, and more efforts need to be dedicated at primary and secondary care levels to mitigate the long-term impact of dyslipidemia on health.38,39 Primary care services should be leveraged to identify patients at risk for ACS, treat CV risk factors, and offer patient and family education to prevent ACS and decrease mortality rates. In addition, awareness must be raised among patients with prior ACS, in terms of health hygiene, blood lipid control by medications, regular screening, and the risk of ACS recurrence due to dyslipidemia.
Study limitations
This study include a small sample size, which was further reduced for primary endpoint analysis; thus not reflecting the population of ACS patients in Saudi Arabia. Additionally, the 4 study centers are not representative of the large Saudi Arabia territories. Moreover, no data were collected on dietary measures, physical exercise and other health hygiene practices prescribed/implemented after ACS occurrence to try and mitigate subsequent CV risks.
In conclusion, The management of dyslipidemia (notably high LDL-C) post-ACS remains suboptimal in Saudi Arabia, despite widespread statin prescription, which increases the risk of ACS recurrence. This study attempted to fill a literature gap on the management of ACS patients in Saudi Arabia; and has identified a lag in achieving LDL-C targets, a virtually complete absence of statin treatment until after the ACS has occurred, as well as a need for raising awareness on the benefits and safety of statins (and potentially other LLTs) among ACS patients. We reiterate the importance of involving primary care in the prevention, diagnosis and management of dyslipidemia, streamlining treatment and follow-up of patients with ACS and ACS risk factors and launching awareness and educational initiatives for the general population, healthcare providers and medical students.
Inspired by invaluable real-world data provided by the START registry highlighting the suboptimal management of dyslipidemia in clinical practice and given the gaps identified in the current study, we propose the development of a nationwide continuous dyslipidemia registry in Saudi Arabia.40 This registry will include clinical, pharmacological, and health hygiene data, on patients at high risk for ACS and on patients with ACS, and will allow for risk factor surveillance, follow-up of trends, as well as research and clinical practice.
Acknowledgment
The authors would like to acknowledge Dr. Jessica Saliba, a Senior Medical Writer with KBP-Biomak, a Contract Research Organization, for writing and editorial support; funded by Sanofi® (KSA affiliate), Riyadh, Saudi Arabia. The authors would also like to thank Mrs. Zeina Chalhoub for English language editing.
Footnotes
Disclosure. Michael U. Youssef is a Sanofi employee. Other authors have no conflict of interest and this study was funded by the Sanofi group headquartered in Paris, France.
- Received February 6, 2023.
- Accepted May 17, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.