


Abstract
Objectives: To identify barriers and facilitators to physiotherapy adherence in adult patients who attended an orthopaedic clinic and underwent physical therapy at King Khalid University Hospital (KKUH), Riyadh, Saudi Arabia.
Methods: This cross-sectional study was performed at KKUH between September 2022 and January 2023. After conducting a literature review, a survey questionnaire was created, and a pilot study was conducted to evaluate its validity and clarity. Patients were approached in the waiting areas of the outpatient clinics and provided with a consent form to participate in the study.
Results: Ongoing pain, travel distance, and lack of transportation were common barriers while being given a choice in rehabilitation activities, regular assessments of progress and function, and regular goal setting with the physician were common facilitators. Living in rural areas and the belief that rehabilitation is important were associated with both higher barrier and facilitator scores.
Conclusion: A patient-centred approach to physical therapy, effective pain management, and regular evaluation of functional progress can increase adherence to physiotherapy. These findings have implications for physiotherapy providers, policymakers, and patients in promoting adherence to treatment for improved functional outcomes, reduced pain, and increased patient satisfaction.
It is well documented that a fundamental underlying adherence must exist to achieve optimal outcomes throughout the full spectrum of management options.1 This is especially evident in disciplines such as physical therapy, where adherence has long been recognized as a major obstacle. Non-compliance has been shown to be highly prevalent, with some studies showing up to 65% of attendees to be non- or partially adherent.2-4 When such neglect has been measurably shown to have adversely affected outcomes throughout the multitudes of physical therapy sessions, a search for the underlying factors is warranted.5-7
This research attempts to survey the underlying motivators towards and against compliance with a physiotherapy program through enquiry and subsequent analysis of multiple facilitators and barriers. Such studies highlighted a lack of sufficient data to infer appropriate results and the need for further research to improve knowledge on this subject.7,8 The insufficiency of data regarding the obstacles and enablers in the field of physiotherapy in Saudi Arabia is particularly noticeable. This scarcity of information is exacerbated by the cultural dissimilarities between the Arabic culture and the Western culture that has been the subject of numerous prior research. This inevitably results in distinct differences that may have a quantifiable impact on specific outcomes. As a result, this constrains efforts to improve the efficacy of physiotherapy within an Arabic society, particularly within the context of Saudi Arabia. This study utilized a cross-sectional approach where a questionnaire was distributed amongst patients attending an orthopaedic clinic, primarily to seek out clinically significant barriers and facilitators and secondarily to extrapolate potential approaches to better compliance and adherence rates and, therefore, better outcomes.
Methods
This study, which followed a cross-sectional design, took place at King Khalid University Hospital, which is a tertiary academic centre located in Riyadh, Saudi Arabia. It primarily serves the local population in Riyadh and its surrounding regions. The hospital serves a diverse population, including Saudi citizens and residents. The study was performed between September 2022 and January 2023. We targeted adult patients who had attended an orthopaedic clinic and had previously received physical therapy. We excluded patients who were <18 years old, did not attend any physical therapy sessions, were last offered physiotherapy more than 10 years ago, and those with cognitive deficits or who could not read or write. The aforementioned individuals were excluded from the study due to their failure to satisfy the research objectives.
The study adhered to the principles of the Helsinki Declaration and received its ethical approval from The Institutional Review Board at the College of Medicine, King Saud University, Riyadh, Saudi Arabia (approval no E-22-7019). After being told of the study’s goals and given the option to resign at any time without incurring any obligations to the study team, each subject completed a signed consent form indicating their agreement to participate.
To ensure an adequate sample size, at least 420 individuals were approached for enrolment in the study. The calculation of the sample size took into account the current population size of Riyadh, aiming for a 95% confidence level and a margin of error of 5%. A 10% was added to account for refusals; 18 (2.1%) refused to partake in the study. Out of 402 participants enrolled in the study, 62 (15.4%) participants were also eliminated for meeting an exclusion criterion or for incomplete responses. This yielded a response rate of 340 (84.6%) responses analyzed in this study.
The questionnaire employed in this investigation was based on a thorough review of the literature and was subjected to a team discussion involving 2 clinical physiotherapists.9 To minimize potential self-reported data biases, the study participants were assured that their responses would be kept anonymous and confidential. The questionnaire’s validity was evaluated by survey research experts, and it was designed to minimize fatigue. The questionnaire was divided into 4 sections. The first section assessed sociodemographic characteristics; the second section had questions regarding the participants’ physiotherapy referrals and clinical conditions. The third section assessed barriers and the fourth section accessed facilitators of physiotherapy.
The questionnaire was originally created in English and subsequently translated into Arabic by a translator not specialised in the medical field and was subsequently reviewed by a specialist in the medical field. A pilot study was then carried out with participants to ensure the clarity of expression of the survey items.20 The data obtained from the pilot sample were not utilized for subsequent analysis. The final version of the questionnaire was distributed in both Arabic and English, and participants were expected to spend approximately 5-10 minutes to complete it.
Patients were approached in the waiting areas of the orthopaedic outpatient clinic and provided with a consent paper explaining the study’s goal. They were then administered a questionnaire in their preferred language. Duplication was minimized by asking the patient if they participated in the study before.
Data cleaning involved the removal of any responses with more than 10% missing data. Any missing response of less than 10% was assigned an average score for missing variables. Finally, participation with responses that were deemed invalid, such as contradictory responses, was also eliminated.
The barriers and facilitators of physiotherapy were assessed using 9- and 8-item sections, respectively. Each question contains 3-point Likert scale categories, such as “not at all” coded with 0, “sometimes” coded with 1, and “a lot” coded with 2. The total scores for both barriers and facilitators were calculated by adding all the items present in the section. The higher the score, the higher the barriers or facilitators to physiotherapy. We used 50% and 75% as cut-off points to determine the levels of barriers or facilitators faced by the participant during their physiotherapy journey. Patients were categorized as having low adherence barriers or facilitators if the score was below 50%, as average if the score was 50%-75%, and high if the score was above 75%.
Confirmatory factor analysis was done to determine if all 17 questions (9 questions for barriers and 8 for facilitators) represent the same construct. For questions regarding the barriers (Q1-Q9), confirmatory factor analysis was done to determine if all the items represented the same construct. The rotation used was direct oblimin. The determinant was =0.168, suggesting that the items were related. No items had a correlation value ranging from 0.095 to 0.477, and no value was ≥0.8, suggesting no multicollinearity (item cut-off for multicollinearity of 0.8). To maintain the integrity of the matrix, no items were eliminated. The Kaiser-Meyer-Olkin measure of sampling adequacy yielded a value of 0.745, indicating satisfactory sampling adequacy, and Bartlett’s Test of Sphericity was statistically significant (p<0.001), indicating that the data were suitable for factor analysis. The reliability analysis demonstrated Hotelling’s T-squared test value of 32.819 (p<0.001), indicating significant reliability and a good level of internal consistency was observed with a Cronbach’s alpha coefficient of 0.750.
For questions about the facilitators (Q1-Q8), confirmatory factor analysis was also done to determine if all the items represented the same construct. The rotation used was direct oblimin. The determinant was =0.150, suggesting that the items were related. No items had a correlation value ranging from 0.094 to 0.546, and no value was ≥0.8, suggesting no multicollinearity (item cut-off for multicollinearity of 0.8), so no item would be eliminated from the matrix. The Kaiser-Meyer-Olkin measure of sampling adequacy yielded a value of 0.740, with a significant Bartlett’s Test of Sphericity (p<0.001). Reliability analysis showed Hotelling’s T-squared test of 40.463 (p<0.001) and good internal consistency (Cronbach’s alpha of 0.758).
Statistical analysis
Qualitative variables are presented using numbers and percentages in the form of descriptive statistics, while mean, and standard deviation are utilized for quantitative variables. To examine the association between the total barriers and facilitator scores with sociodemographic characteristics, the Mann-Whitney Z-test and Kruskal-Wallis H-test were employed. Data analysis was conducted using Statistical Packages for Social Sciences Statistics for Windows, version 26 (IBM Corp., Armonk, N.Y., USA). Statistical significance was determined at a threshold of p<0.05.
Results
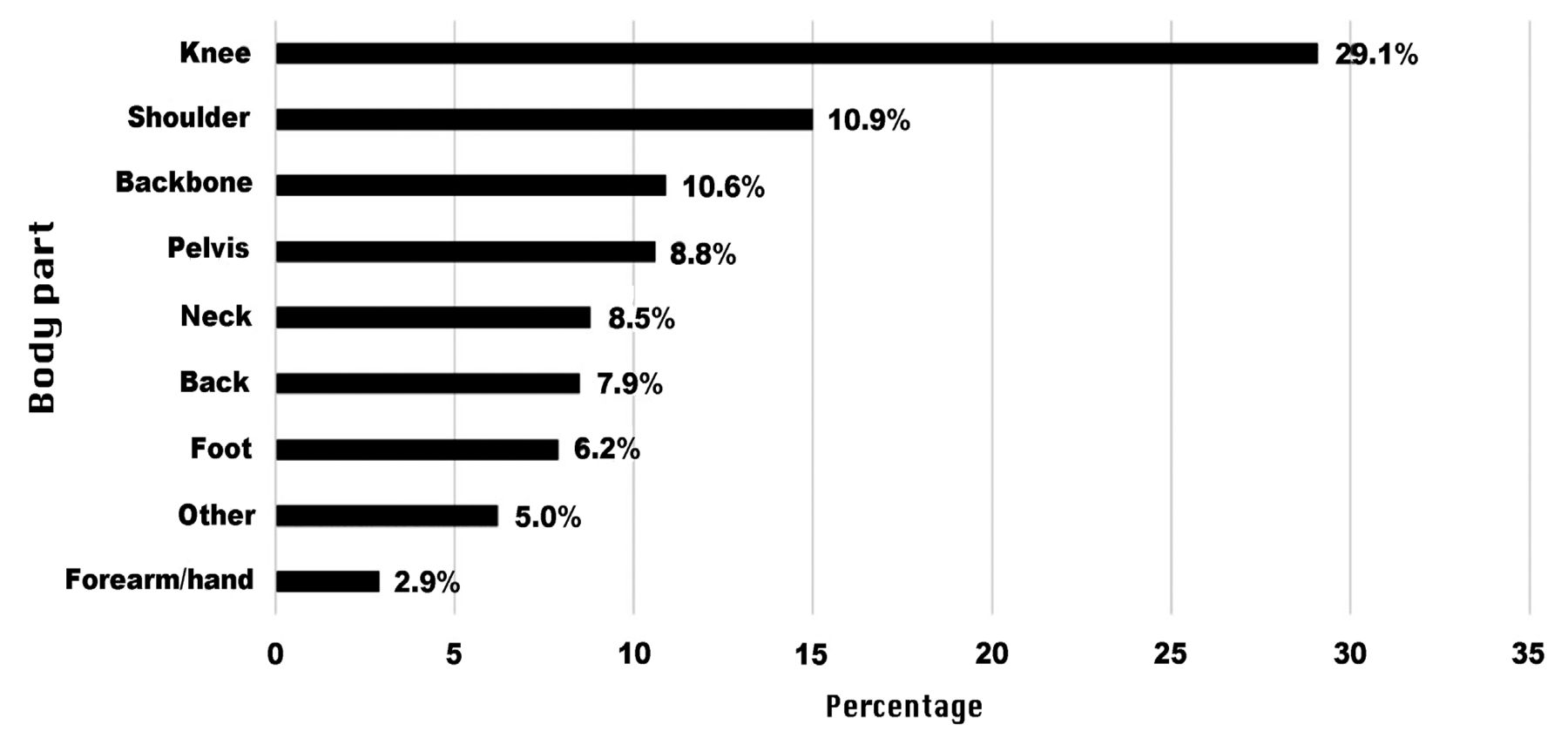
A total of 402 individuals were initially enrolled in the study. However, 62 patients were excluded either because they met one or more exclusion criteria or during the data-cleaning process. As a result, the final sample size consisted of 340 patients included in the study. As seen in Table 1, the most common age group was 31 to 40 years (41.5%), with more than half being male (57.9%). Most lived in urban areas (82.4%), with 64.1% of respondents being employed. A total of 53.2% of the patients had a bachelor’s degree. The most common reason for referral to physiotherapy was conservative treatment (55.3%), and more than half (52.9%) of the participants believed that rehabilitation is very important. Nearly half (49.4%) indicated a 16 to 30 minutes (mins) travel time from home to the physiotherapy location. Approximately 56.2% of the patients had regular sessions with a physiotherapist as part of their rehabilitation, mostly at a public hospital clinic (80.3%). As shown in Figure 1, the most common location of the body for rehabilitation referral was the knee (29.1%), followed by the shoulder (15%) and back (10.9%).
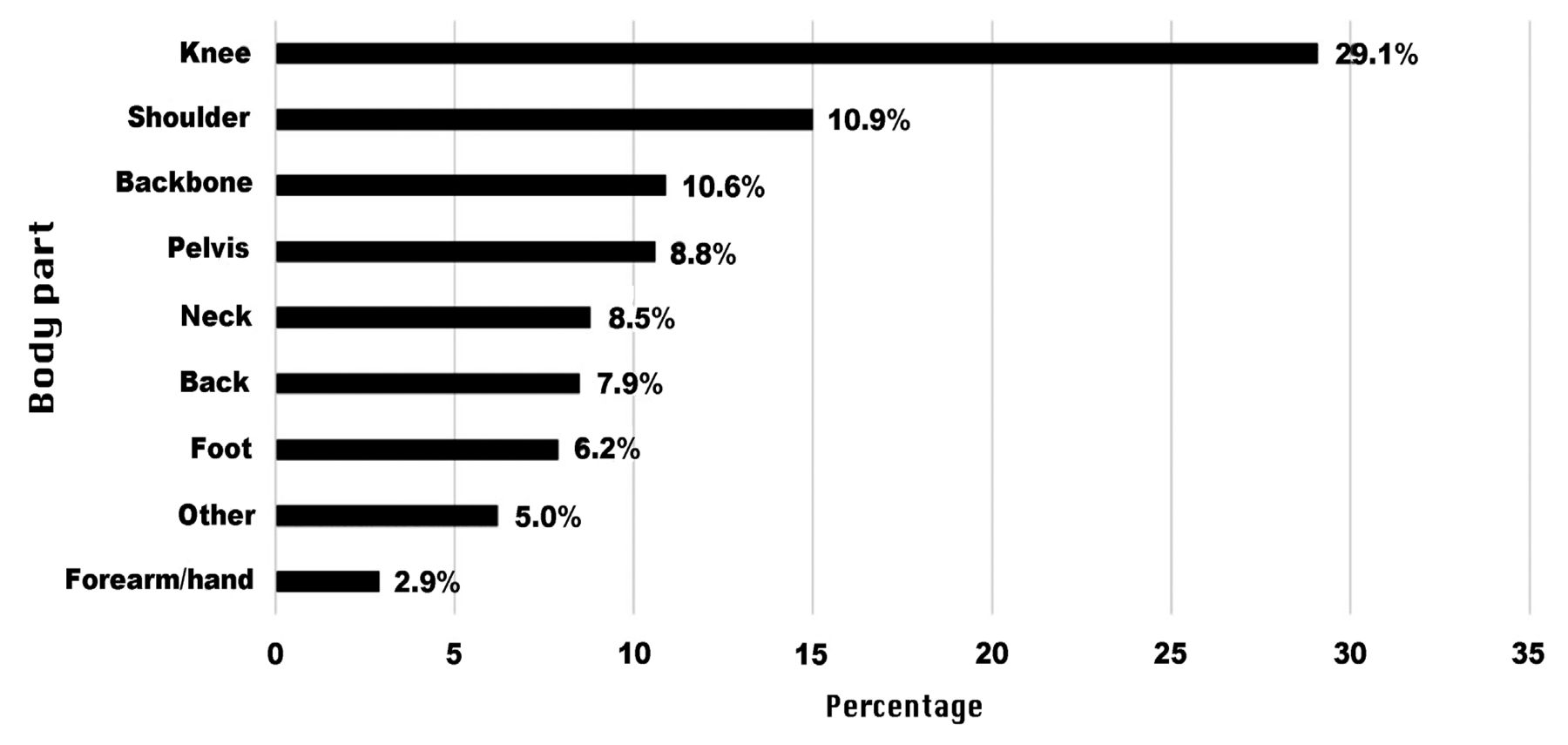
- Physiotherapy referral locations illustrating the highest referral location was the knee joint followed by shoulder.
- Sociodemographic characteristics of adult orthopaedic patients (N=340).
The assessment of the barriers and facilitators of physiotherapy is shown in Table 2. According to the patients’ ratings, the most common barrier to physiotherapy was ongoing pain (mean score:1.36), followed by distance to the physiotherapy centre (mean score:1.35) and no means of transportation (mean score:1.33). The overall mean score for barriers to physiotherapy was 11.6 (SD=3.52), with low (18.8%), average (53.8%), and high (27.4%) levels of barriers to adherence. Regarding facilitators of physiotherapy, based on patients’ ratings, the most common factors of facilitators were “Being given a choice in what you do for rehabilitation” (mean score:1.41), “Regular assessments of your progress and function” (mean score:1.41), and “Regular goal setting with your rehabilitation provider” (mean score:1.41). The overall mean score of facilitators to physiotherapy was 10.7 (SD 3.16), with low (12.1%), average (62.6%), and high (25.3%) levels of facilitators to adherence detected.
- Assessment of barriers and facilitators to physiotherapy among adult orthopaedic patients (N=340).
In assessing the relationship between sociodemographic characteristics and barrier scores, it was observed that higher barrier scores were significantly associated with living in rural areas (Z=4.478; p<0.001) and having a strong belief in the importance of rehabilitation (H=20.186; p<0.001). However, no significant differences in barrier scores were found based on other sociodemographic variables, including age, gender, employment status, educational level, reason for physiotherapy referral, distance from home to physiotherapy location, seeing a physiotherapist at rehabilitation, and type of clinic for rehabilitation (p>0.05).
We also tested the association between the sociodemographic variables in terms of the facilitator’s score. Based on the results, it was perceived that a higher facilitator score was more associated with living in the rural areas (Z=5.338; p<0.001), being unemployed (Z=1.994; p=0.046), being less educated (Z=2.032; p=0.042), having a travel time from home to physiotherapy location of 16 to 30 min (H=11.999; p=0.002), those who believed that rehabilitation is very important (H=71.768; p<0.001), and those who undergo their rehabilitation at the public hospital clinic (Z=3.125; p=0.002). Other sociodemographic characteristics did not show significant differences with facilitator score, including age, gender, the reason for physiotherapy referral, and seeing a physiotherapist as part of rehabilitation (p>0.05).
Discussion
Barriers to physiotherapy are an ongoing challenge for healthcare providers and patients. Physiotherapy is an indispensable component of healthcare and provides critical intervention for various musculoskeletal conditions. Unfortunately, its full potential is often hindered by several factors that impede compliance. Fear of re-injury, ongoing pain, geographical and time limitations, rehabilitation program length, cost, convenience, and perceived value can reduce or deny the benefits of physiotherapy services to patients.10-14
Understanding the barriers to accessing physiotherapy care is crucial for comprehending why people may or may not follow the recommended treatment plan.8 A study by Walker et al9 investigated the influence of living areas on the frequency and duration of supervised rehabilitation and found that those who lived in urban areas showed a significantly higher frequency and duration of physiotherapy. Similarly, we found that higher barrier scores were significantly associated with living in rural areas. This is particularly problematic in remote areas with few public transport options and no rehabilitation centres nearby.
The study revealed that a lack of motivation and confidence were significant barriers to successful rehabilitation in the Saudi population. This finding is consistent with previous literature, which determined that lack of motivation was a primary factor preventing people from actively engaging in treatment.9,15,16 However, for physiological adaptations to occur, the patient must actively engage in treatment and have it adapted and advanced as needed.17,18 Thus, individuals must be willing and motivated, especially if they participate in long-term rehabilitation programmes. Furthermore, psychological support may be necessary to help develop self-confidence and optimism towards engaging in rehabilitative processes.
Physical treatment compliance is hindered by ongoing pain during exercise, proving the importance of initial pain management techniques.10,19 To provide the best clinical care, clinicians need to gain an understanding of their patients’ experiences and beliefs concerning pain, as many individuals think that any activity that causes pain must have a negative impact.8,20 This explains why the results show the highest mean score was in the ongoing pain barrier domain, suggesting that clinicians should reiterate messages that alleviate the fear of pain, such as the fact that most patients can safely engage in therapeutic exercise despite experiencing pain, and that it may even result in a decrease in symptoms, improved function, and ultimately return to work.21-23
- Differences in the score of barriers in relation to the sociodemographic characteristics of adult orthopaedic patients (N=340).
- Differences in the score of facilitators in relation to the sociodemographic characteristics of adult orthopaedic patients (N=340).
One of the primary barriers to the younger population completing their suggested therapy, mainly after sport-related injuries, is the fear of re-injury, as it is a vital predictor of successful sports return.24,25 The fear of re-injury was among the lowest attributed barriers. However, most studies that linked fear of re-injury targeted the younger population. After age adjustment to the mean scores, the young age group (18-30 years old) was consistent with the previously mentioned studies. Therefore, rehabilitation service providers should prioritise developing appropriate rehabilitation programs that provide gradual exposure to exercises to lessen the fear of re-injur, which also improves psychological readiness for sports return.26,27
Another major obstacle was the time and commitment to the rehabilitation program.9 This emphasises the importance of setting reasonable expectations early to prepare patients for a fully drawn-out rehabilitation process.28,29 The length of the rehabilitation plan, lack of time, and need for commitment were perceived as significant barriers to adherence to physical therapy. A study that evaluated the duration of treatment and commitment showed that a longer duration of treatment - 5-7 weeks had deficient compliance compared with a 2-3-week plan.30 Physiotherapists must be aware of the challenges that patients anticipate when following a recommended treatment plan and working with their patients to create treatment plans tailored to their living circumstances, including coping strategies to achieve treatment goals.14,31,32
An important objective of this study was to identify the factors that facilitate patients’ compliance with their physiotherapy. By focusing on and enhancing these factors, we can improve patients’ compliance with their rehabilitation, thus enhancing the treatment process. Unfortunately, few studies have explored the facilitators of physiotherapy in patients. However, the results showed that factors such as patient engagement in their rehabilitation program, a positive relationship with their physiotherapist, regular evaluations and goal setting for their rehabilitation, and the selection of exercises that are both enjoyable and applicable to daily activities all help patients adhere to their rehabilitation.
This study revealed that one of the most crucial facilitators of physiotherapy was granting patients the freedom to choose what they wanted to do for their treatment. Patients have previously emphasized the importance of actively participating in rehabilitation and being involved in the design and execution of their physiotherapy program. It is crucial that physiotherapy providers provide patients with the agency over their rehabilitation, encourage their decision-making, and actively involve them in their treatment.33
In accordance with previous studies, the current study revealed that a positive patient-provider relationship improves patient compliance with rehabilitation.9,33 This might compel physiotherapists to pursue training on how to communicate with patients more effectively and foster a safe, secure, and interactive atmosphere that can be tailored to each patient’s personality.
The study found that frequent assessments and goal setting with the patient’s physiotherapist improved compliance and helped develop a more interactive and engaging rehabilitation program. Patients who undergo regular assessments may be able to identify areas that require improvement and receive encouraging feedback when their goals are accomplished.
According to patient reports, the study showed that a more engaging and pertinent exercise program improves patients’ overall compliance with rehabilitation. This aligns with the results of the previous studies.9 Physiotherapy providers must tailor each patient’s rehabilitation program based on their lifestyle, interests, and goals.
The results of this research can be used to guide the establishment of interventions that will increase adult orthopaedic patients’ commitment to physiotherapy, especially in the Arab world. By addressing the identified barriers and enhancing the facilitators, patients can be supported to adhere to their physiotherapy programs, resulting in better outcomes and avoidance of unnecessary treatment plan escalations.
Study limitations
The study had several restrictions that must be taken into account. First off, the study’s emphasis on adult orthopaedic patients at KKUH restricted how broadly the results can be applied to other demographics or healthcare environments. Furthermore, as surveys and questionnaires were the only methods used for data collection, it’s possible that the study didn’t fully account for the intricacy of the barriers and facilitators. A more in-depth understanding of the experiences and viewpoints of patients might be possible by combining several techniques, such as interviews or direct observation.
In conclusion, the study found that physiotherapy providers could benefit from implementing a patient-centred approach to therapy, focusing on effective pain management and regular evaluation of functional progress. Policymakers could use these findings to develop guidelines and policies that promote adherence to physiotherapy, and patients could use these findings to inform their decision-making and better understand the importance of adhering to their physiotherapy treatment plan and prevent unnecessary escalation of intended therapy.
Acknowledgment
The authors gratefully acknowledge Editage (www.editage.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 23, 2023.
- Accepted June 21, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.