


Abstract
Objectives: To compare the radiographic outcomes of our patients who encountered medial wall disruption, with those who did not while undergoing Dega osteotomy.
Methods: We retrospectively reviewed the records of 95 hips with developmental dysplasia of the hip who were treated with Dega pelvic osteotomy. Hips were divided into 2 groups according to medial wall disruption: group A included the hips with medial wall disruption, while group B included the hips without disruption. Preoperative, immediate postoperative, 12 weeks and last follow-up anteroposterior radiographs of the pelvis were reviewed for changes in the acetabular index (AI) between groups.
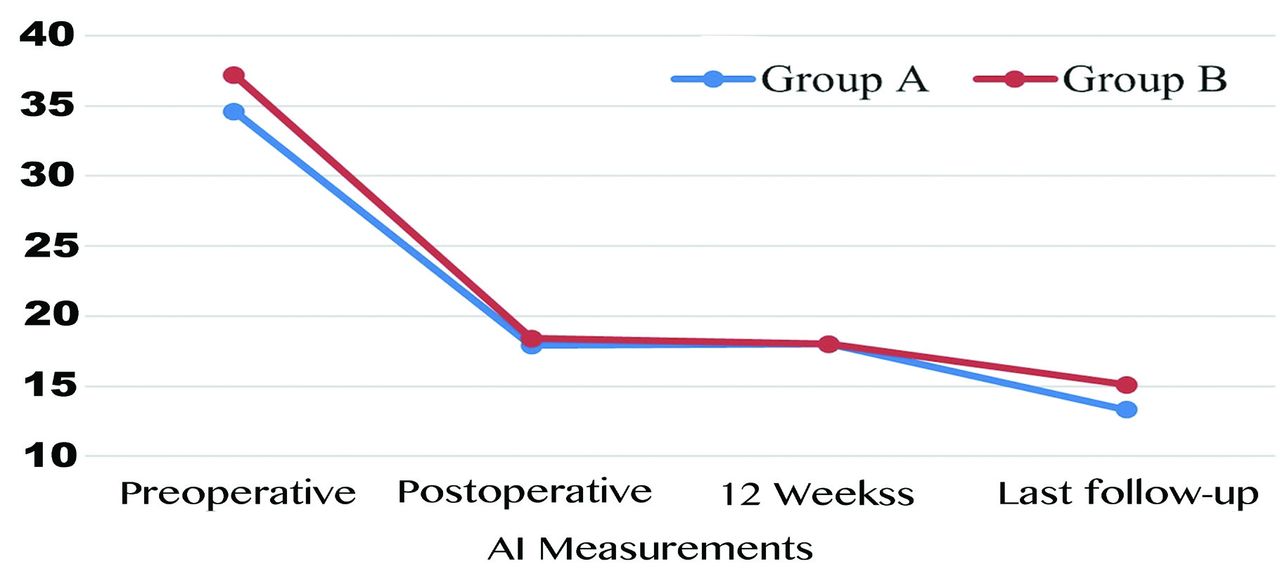
Results: There were 22 hips in group A and 73 hips in the group B. Preoperative (34.6 versus [vs] 37.2, p=0.231), postoperative (17.9 vs 18.4, p=0.682), 12th week (18 vs 18, p=0.504) and last follow-up (13.3 vs 15.1, p=0.097). The acetabular index measurements were comparable between the groups. Corrections achieved during surgery, and during the follow-up period were also comparable between the two groups, indicating no loss of radiographic correction caused by medial wall disruption. Ninety one percent of the patients in group A and 90% of group B achieved good or excellent results according to the Severin classification (p=0.944).
Conclusion: Our study shows that disruption of the medial wall did not have a significant detrimental effect on radiographic correction when performing Dega osteotomy.
Developmental dysplasia of the hip (DDH) is a spectrum of disorders that range from acetabular dysplasia without subluxation to irreducible hip dislocation. If left untreated, DDH can result in hip pain and osteoarthritis by early adulthood. The treatment aims to obtain a stable, congruent, and concentric hip joint as early as possible to allow remodeling of the acetabulum and proximal femur with minimal complications.1,2
Treatment of DDH usually becomes more challenging as age increases. After the child reaches walking age, most surgeons agree that the treatment must include a pelvic osteotomy to ensure adequate femoral head coverage.3,4 Among the different types of pelvic osteotomies, Salter, triple pelvic osteotomy (TPO), Pemberton, and Dega are the most commonly used. Salter5 and TPO6 are redirectional osteotomies aimed to reorient the acetabulum, whereas Pemberton7 and Dega8 are reshaping osteotomies that change the shape, and hence the dimensions, of the acetabulum.
Wiktor Dega first published his pelvic osteotomy technique in the Polish language in 1969;but this technique gained popularity only after being published in the English language in 2001.9,10 This technique is a supraacetabular semicircular incomplete osteotomy that allows correction of anterior, lateral, and posterior deficiencies by hinging into the triradiate cartilage.11 When the acetabular dysplasia is severe, Dega osteotomy is the selected procedure as it provides remarkable correction of the acetabular index (AI).4,12,13
During the procedure, the inner cortex of the ilium may be accidentally penetrated by the osteotome, which can be seen as a technical error. In our cases with this error, we observed a disruption of the medial wall on the intraoperative fluoroscopic views and further radiographs. Thus, an incomplete osteotomy has become a complete osteotomy and may result in instability, graft displacement, or failure of correction of acetabular dysplasia. Our study aims to compare the radiographic outcomes of our patients who encountered penetration of the inner ilium cortex, with those who did not while undergoing Dega osteotomy.
Methods
This study is carried out at the Department of Orthopedics and Traumatology, Hacettepe University Hospital, Ankara, Turkey. We retrospectively reviewed patients with DDH who underwent Dega osteotomy at our institution, between January 2015 and January 2021. The main indication for Dega osteotomy was acetabular dysplasia according to the radiographic parameters, including AI, subluxation of the hip, or a shallowed acetabulum. Patients who were diagnosed with a disorder other than DDH (such as, teratological hip dislocation), who underwent previous acetabular surgery, or had a follow-up period of less than 1 year were excluded from the study. As a retrospective study, all procedures performed on the patients were part of the routine care, and no patients were recalled specifically for this study.
All patients were operated on by the same surgeon. Open reduction, femoral shortening, or derotation osteotomy were also performed if considered necessary by the surgeon, and the decision was made intraoperatively. If a femoral osteotomy was performed, then the femoral graft was used at the pelvic osteotomy site. In all other cases, the autograft was harvested from the iliac bone in triangular pieces. The graft was seated into the osteotomy site by using an impactor with gentle mallet blows until the graft is flush with the outer cortex of the ilium. The stability of the osteotomy site was clinically confirmed by stressing the proximal portion of the osteotomy, and if found to be stable, no additional fixation was performed. At the end of the procedure, radiographs were taken before and after the application of the spica cast to prevent the occurrence of loss of correction. Patients were immobilized in a hip spica cast for 6 weeks postoperatively.
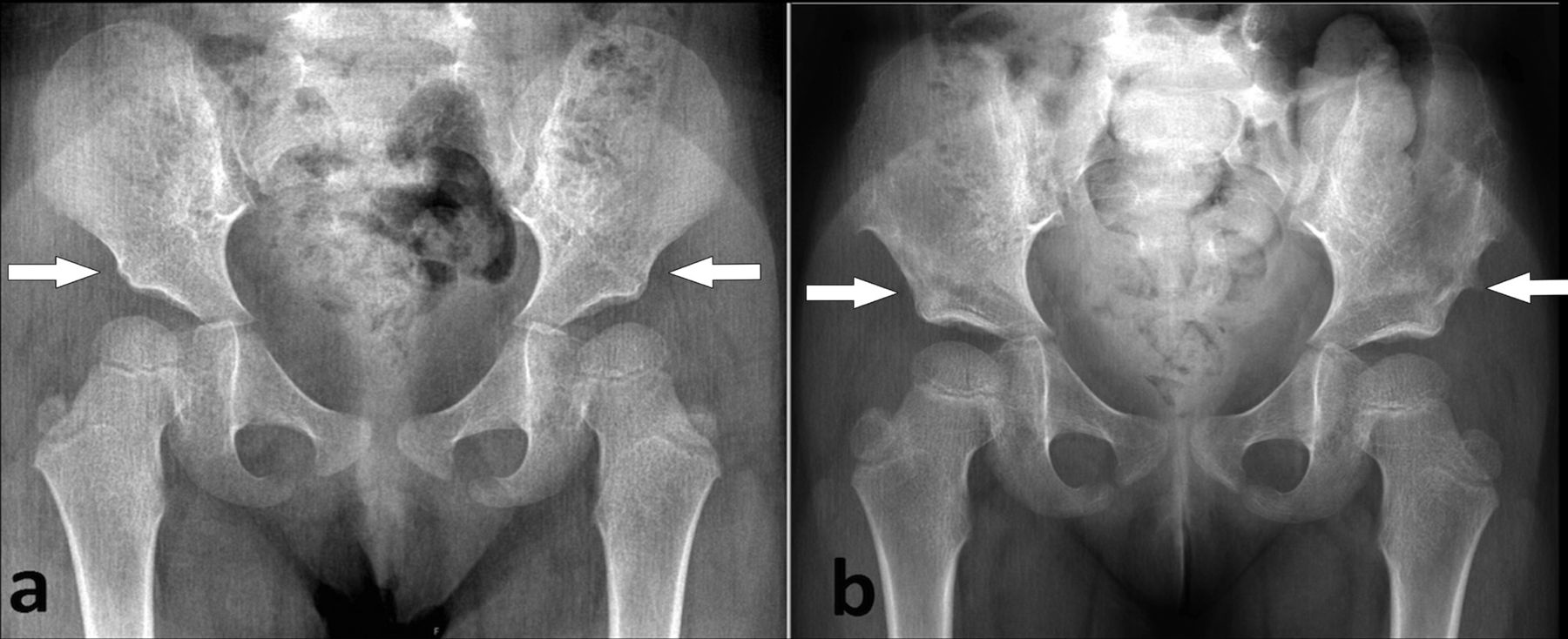
Ninety-five Dega osteotomies were performed on 75 patients, and 20 of them were bilateral. Twenty-two hips of 21 patients with medial wall disruption were identified in the immediate postoperative radiographs (Figure 1). Accordingly, we classified the hips into 2 groups to explore potential differences: group A includes hips with medial wall disruption, whereas group B includes hips without disruption. Compared with the patients without disruption, the cast duration was not modified for these patients, and no brace was advised after the removal of the cast. Thus, the postoperative course was identical. Previous surgical treatments and adjunct procedures at the time of Dega pelvic osteotomy were recorded. Preoperative, immediate postoperative, 12 weeks, and last follow-up anteroposterior radiographs of the pelvis were reviewed by xone surgeon on the hospital PACS system (Centricity PACS, GE Healthcare). Radiographs at postoperative 12 weeks and the last follow-up were selected to evaluate the short-term and final results. The acetabular index was used as the primary outcome measure to compare between groups.14 Additionally, the values of the acetabular depth ratio (ADR)15 were recorded preoperatively and at the last follow-up. The Severin classification system was also used as a secondary outcome measure.16 Classes 1, 2 and 3 were established as excellent, good and fair while classes 4, 5 and 6 are all considered poor. For comparison between groups, the Severin classification was further grouped into 2 categories as <3 and ≥3. Possible triradiate cartilage injury was noted. Ethical approval was obtained from the local ethics committee (protocol number: 16969557-1558). Patients’ legal guardians gave written informed consent for participation in the study.

- Examples of postoperative radiographs after Dega pelvic osteotomy: a) Intact medial walls after bilateral osteotomy, b) Left hip demonstrates medial wall disruption after osteotomy.
Statistical analyses
Statistical analyses were performed using the software package SPSS (IBM Corp. Released 2015. IBM SPSS Statistics for Mac OS, Version 23.0. Armonk, NY). Descriptive statistics are presented as means, standard deviations, and ranges. When comparing means between study groups, the Mann–Whitney U test and student’s t-test were used for non-parametric and parametric data groups.. Wilcoxon’s signed rank test and paired samples t-test were to compare dependent variables. Chi-square and Fisher’s exact tests were used for cross-tabulation statistics. The threshold for statistical significance was designated as p<0.05.
Results
Table 1 summarizes the demographic and radiographic characteristics of the groups. The average length of follow-up was 2.6 years (ranging 1–6.1 years). Group A had 22 hips (21 patients) and group B had 73 hips (54 patients).. The average age at the time of the procedure and average follow-up length were comparable between groups ((p=0.113 for age and p=0.778 for follow-up). Preoperative AI values were comparable between groups (p=0.231).
- Radiographic and demographic characteristics of the study groups.
Table 1 presents the mean AI values during the study period. Corrections in AI achieved at surgery, which is measured by calculating the difference between preoperative and postoperative AI measurements for each patient, are significant for both groups (p<0.001 for both groups). Corrections achieved during the follow-up period, both at 12 weeks and until final follow-up, were also comparable between the 2 groups, indicating no loss of radiographic correction caused by medial wall disruption. When the last follow-up AI measurements were compared with the immediate postoperative values, significant reductions were seen in each group (p<0.001 for both groups). Figure 2 demonstrates the measured AI values and comparisons between groups.

- Acetabuler index values and comparisons between groups.
Preoperative (p=0.363) and final (p=0.181) ADR values were comparable between groups and both groups showed significant improvements in ADR values during the study period (p<0.001 for each). According to the Severin classification, 20 of 22 hips (91%) were excellent and good in group A, compared with 66 of 73 hips (90%) in group B with the same result (Table 1). No significant difference was observed between groups (p=0.944). Four of 73 (6%) hips in group B were classified as a poor result according to the Severin classification, 2 of which were redislocation, and the other 2 were resubluxation. All the patients refused revision surgery, except for one. No radiographic sign of triradiate cartilage injury was observed in the entire study population up to the last follow-up radiographs.
Table 2 summarizes the additional surgical procedures performed in the study groups. The groups are comparable in terms of previous reduction and revision rates. The simultaneous surgery rate was significantly higher in group B (p=0.021). In group A, 3 (14%) of the previous reductions were closed, and 5 (23%) were open. In group B, 12 (17%) of the previous reductions were closed, and 9 (12%) were open. In group A, 3 (14%) of the simultaneous surgeries were open reductions, and 3 (9%) were open reduction and femoral shortening osteotomies. In group B, 21 (29% of the simultaneous surgeries were open reductions, and 16 (22%) were open reduction and femoral shortening osteotomies.
- Additional surgical procedures in the study groups.
Discussion
Although the treatment of DDH starts at an early period by early diagnosis using clinical and ultrasound screening programs, residual acetabular dysplasia continues to be a significant problem in the spectrum of DDH. Therefore, the need for pelvic osteotomies will remain. Although different types of pelvic osteotomies have been described, their main purpose is to delay the development of early osteoarthritis. Each technique has unique advantages, and none of them is unequivocally superior to another.
Dega osteotomy is a versatile procedure that provides coverage to all kinds of acetabular deficiencies. Although the original surgical technique is still debated, the classical Dega osteotomy is performed by cutting through the lateral wall of the ilium directed toward but not through its inner cortex.17 The hinge point is mainly at the triradiate cartilage, and anterior, lateral, or posterior deficiencies can be treated by relocating the graft.10,13 Dega osteotomy is also intrinsically stable, and further stabilization is not needed. Therefore additional surgery for implant removal is prevented. Moreover, it does not produce limb-length discrepancy and can be safely performed bilaterally in the same surgical session.18 The main disadvantages of this osteotomy are the need for fluoroscopic guidance and open triradiate cartilage.
Several authors reported excellent and satisfactory medium and long-term results of Dega osteotomy.10,11,19-26 A recent study that published the results of open reduction, Dega osteotomy, and proximal femoral osteotomy in delayed diagnosis of DDH showed that survival rates were 73% at 40 years in patients who were operated on before the age of 5 years.24
AI remains a reliable radiographical parameter in the evaluation of acetabular development.26 The mean AI of all hips in this study population was corrected from 36.6 degrees (°) preoperatively to 14.6° at the last follow-up. The 22° improvement in AI in our study was also comparable with the 18°–25° results shown in previous studies.10,11,19,20,23,25 Thus, our study confirms the efficacy of Dega pelvic osteotomy in reducing AI to near-normal values (Figure 3).

- Radiographs of a 3-year-old girl who underwent bilateral Dega pelvic osteotomy: a) Bilateral acetabular dysplasia and broken Shenton’s line can be seen on x-ray, b) Excellent acetabular containment achieved 16 months after surgery.
The acetabular depth ratio is a radiographic parameter that measures the width and depth of the acetabulum. Similar to AI, it reflects acetabular development. In both groups, the mean ADR values were improved to normal percentiles at the last follow-up.15 Although the effect of Dega pelvic osteotomy on the acetabular volume is controversial, the final ADR values in this study support the idea that Dega pelvic osteotomy does not reduce the acetabular volume.1,27,28
The radiological results of this study are satisfactory in both groups according to the Severin classification. We found no statistically significant difference between the groups (Table 1). However, the rate of excellent results is greater in group A (32%) compared to those in group B (27%). Similarly, no poor results were observed in group A, whereas 6% occurred in group B. We can attribute these differences to the higher rates of simultaneous surgery, such as open reduction and/or femoral shortening osteotomy in group B, and possibly to the higher Tonnis grades.
Despite satisfactory results, every surgery, including the Dega osteotomy, has its respective risks. Complications may occur during the surgery due to the incompletely ossified bony structure of young children. We have intraoperatively detected a disruption of the medial wall in rare cases, particularly after unwanted penetration of the osteotome. In such cases, we hypothesized that potential instability related to medial wall disruption may cause graft extrusion or impaction on the osteotomy level and an associated loss of correction. In our study, no graft displacement occurred in any hip with or without disruption. Furthermore, all of the hips with disruption showed similar acetabular indices compared with the group without disruption, not only in the short term but also in the final follow-up. These results indicate that in hips with medial wall disruption, the thick periosteum may still provide stability even after iatrogenic damage. It can be protective against graft displacement until graft incorporation for short-term follow-up. Additionally, considerations for acetabular remodeling due to the osteotomy and reduction of the hip may explain the similar results obtained in the long-term follow-up.29-31 Furthermore, a recent study on graft displacement showed that similar radiologic outcomes could be achieved with spontaneous remodeling after a conservative approach.32
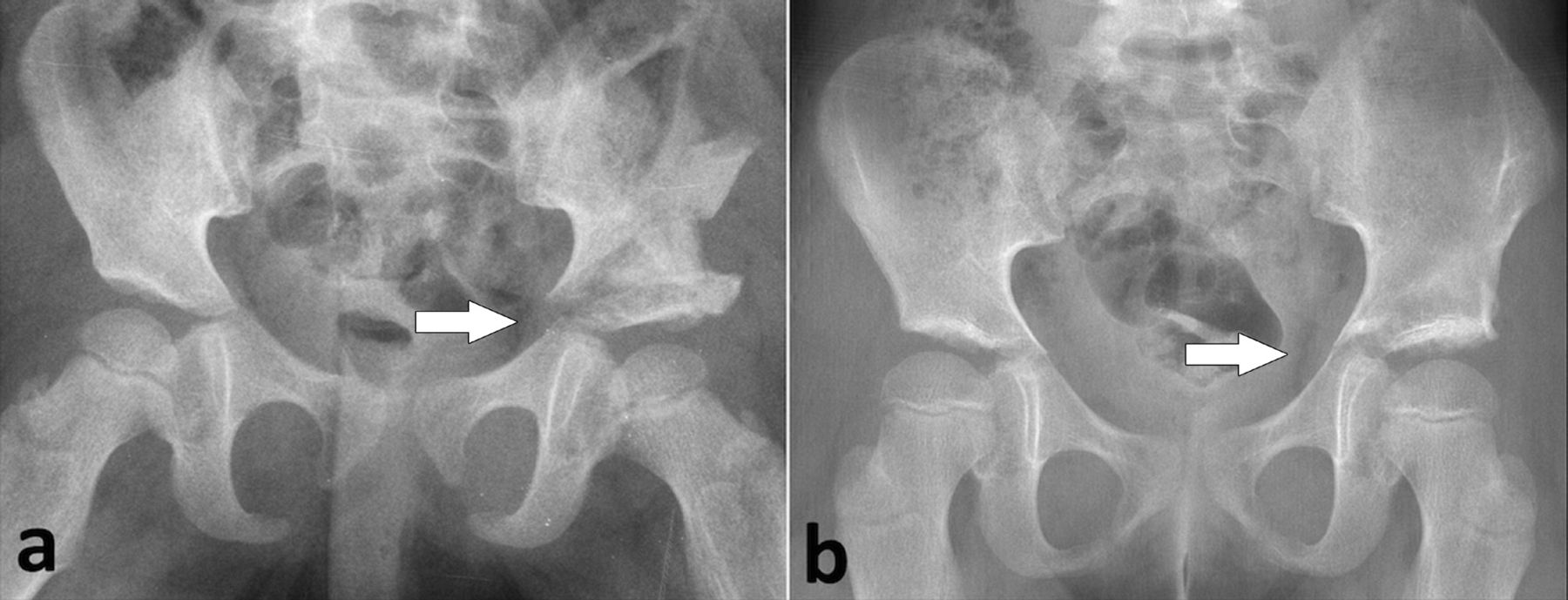
Another complication that may occur due to medial wall disruption is triradiate cartilage injury. The most common radiographic findings of triradiate cartilage injury are widening or narrowing of the triradiate cartilage gap, bone bridge formation, triradiate cartilage ossification, and premature closure.33,34 In most cases, these findings become apparent in the first year after trauma. None of the hips in the current series had radiographic signs of triradiate cartilage injury during the follow-up period (Figure 4). Nevertheless, the hips with medial wall disruption were likely extremely small to reveal differences that may have been clinically important.

- Radiographs of a 3-year-old patient who underwent left Dega pelvic osteotomy: a) Medial wall disruption can be seen on left hip x-ray, b) There was no radiographic sign of triradiate cartilage injury 36 months after surgery.
This study has several limitations. First, this study is retrospective and has a small sample size. Second, no control group with healthy hips was set to compare acetabular development. Moreover, the patients were not examined until skeletal maturity to monitor triradiate cartilage and acetabulum development. However, including 75 patients with 95 treated hips, we report one of the largest studies investigating the radiological outcome of Dega osteotomy in DDH.
In conclusion, our study shows that intraperative disruption of the medial wall did not have a significant detrimental effect on radiographic correction when performing Dega osteotomy in addition to showing the satisfactory results of Dega osteotomy in the treatment of acetabular dysplasia. This is the first study in the literature reporting on this technical error, and we believe that when this happens, the treatment course can safely remain unchanged and there will be no need for additional measures (prolonged casting period, fixation, and so on).
Acknowledgment
The authors gratefully acknowledge Scribendi (www.scribendi.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 18, 2023.
- Accepted June 21, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.