


Abstract
Objectives: To assess the specificity and sensitivity of prognostic biomarkers in individuals diagnosed with acute pulmonary embolism (PE).
Methods: This study retrospectively enrolled 162 patients from the 741 patients who were hospitalized with acute PE and diagnosed using pulmonary computed tomography (CT) angiogram at 5 hospitals in Saudi Arabia between January 2015 and December 2019. Pulmonary embolism patients classified into survivor and non-survivor groups. Neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and red cell distribution width (RDW) were all recorded and were compared between the groups. The evaluation of mortality prediction, sensitivity, and specificity was carried out by employing receiver operating characteristic curves.
Results: The variables NLR and RDW exhibited a statistically significant correlation with increased mortality and disease severity. A total of 8 patients among the 162 patients died. At the cut-off value of 5.5, NLR was showed an association with all-cause mortality, demonstrating a sensitivity of 75% and a specificity of 82%. At the cut-off value of 18.15, RDW was found to be significantly associated with all-cause mortality, displaying a sensitivity of 63% and a specificity of 88%.
Conclusion: Multiple parameters have been implicated in the mortality and severity of PE. Our study revealed a statistically significant association between NLR, RDW, and PE mortality. These tests are easily accessible and may provide insights into the mortality associated with PE.
Pulmonary embolism (PE) ranks as the third most prevalent cause of cardiovascular mortality in hospitalized individuals within Western nations.1 The main mechanism underlying the development of PE is the detachment of the vein thrombus, usually from the lower limb, and its passage to the lung arteries.2 Most clinical presentations of PE are non-specific, resulting in frequent misdiagnosis.3 Pulmonary embolism is associated with significant morbidity; thus, it requires accurate evaluation and diagnosis. Pulmonary angiography is the most accurate method for diagnosing PE; however, it is not used frequently in clinical practice due to its high cost and invasive nature. Computed tomography (CT) pulmonary angiogram and ventilation-perfusion scans are frequently employed diagnostic procedures that are considered to be less invasive in nature.4 Anticoagulant therapy is the mainstay of treatment for PE; however, massive PEs may require thrombolytic therapy.5 Previous studies have demonstrated the validity and utility of the existing prognostic models for acute PE. Although all of these models predict the mortality rate and risk stratification, they also have some differences. For instance, the American Heart Association (AHA) and European Society of Cardiology (ESC) prognostic models are used to identify patients who require therapeutic thrombolysis.6,7 In contrast, the simplified pulmonary embolism severity index (sPESI) is used for the purpose of identifying individuals with a low risk of PE, therefore determining their suitability for outpatient treatment.8 Neutrophil-to-lymphocyte ratio (NLR), red cell distribution width (RDW), and platelet-to-lymphocyte ratio (PLR) are emerging prognostic laboratory biomarkers for several acute conditions, such as pneumonia and multiple chronic diseases including, cancers.9,10
The objective of this study was to assess the specificity and sensitivity of laboratory biomarkers in predicting in-hospital mortality and disease severity among patients diagnosed with acute PE. These biomarkers reflect the role of the inflammatory factors in the coagulation cascade. The pathophysiology of thrombus formation involves an interaction between the inflammatory and coagulation pathways.11
Methods
This retrospective cohort study examined a sample of 162 patients out of a total of 741 individuals who were diagnosed with PE at 5 hospitals (King Fahad General Hospital, Al-Madinah Al-Munawarah, King Fahad Medical City, Riyadh, and the National Guard Hospitals in Al-Madinah Al-Munawarah, Jeddah, and Riyadh, Saudi Arabia) from January 2015 to December 2019. Electronic registries of the King Fahad General Hospital, Al-Madinah Al-Munawarah, King Fahad Medical City, Riyadh, and the National Guard Hospitals in Al-Madinah Al-Munawarah, Jeddah, and Riyadh, Saudi Arabia, were used for this purpose.
The data were filtered based on the inclusion and exclusion criteria (Table 1). In total, 162 patients who satisfied the predefined inclusion criteria were enrolled in the present study.
- The inclusion and exclusion criteria.
Electronic hospital information systems were used to obtain the clinical, demographic data, and laboratory parameters results. Clinical vital signs (pulse rate, blood pressure [BP], and oxygen saturation) and laboratory results were used to classify the PEs as low-risk, sub-massive, or massive. Low-risk PE was defined as the absence of the criteria for massive or sub-massive PEs based on AHA risk stratification. Sub-massive PE was defined as the presence of normal blood pressure (systolic BP [SBP] of >90 mmHg) with signs of right ventricular dysfunction or increased levels of troponin. Massive PE was defined as the presence of continuous hypotension (SBP of <90 mmHg) for more than 15 minutes or the use of inotropes for maintaining the BP within normal limits. The NLR, RDW, and PLR data were obtained from the laboratory results at the time of arrival at the emergency department. Neutrophil-to-lymphocyte ratio represents the proportion of neutrophils to lymphocytes, while PLR denotes the ratio of platelets to lymphocytes.
The present study obtained approval from the Institutional Review Board of the Ministry of Health and King Abdullah International Medical Research Center, Riyadh, Saudi Arabia (IRB: 1173/22).
Statistical analysis
The Statistical Package for the Social Sciences, version 22 (IBM Corp., Armonk, NY, USA), was utilized in the analysis. Descriptive statistics were applied to calculate the frequencies (n) and percentages (%) pertaining to all categorical variables, whereas means and standard deviations (SDs) were used to describe the scale variables. The normality of the scale variables was assessed using the Shapiro-Wilk and Kolmogorov-Smirnov tests. The associations between mortality and the categorical variables were assessed using the Chi-square test, whereas the t-test was used to evaluate the associations between mortality and the continuous variables. Receiver operating characteristic (ROC) curves were obtained for NLR and RDW to illustrate their overall ability to predict mortality, sensitivity, and specificity. Youden’s J statistic was calculated to determine the best cut-off values for NLR and RDW. A p-value of <0.05 was considered significant.
Results
The analysis included 162 participants who met the inclusion and exclusion criteria. A total of 8 (5%) patients experienced mortality during the designated study period. The mean age of all participants was 60.6±18.9 years, with the ages ranging from 21-94 years.
Tables 2 & 3 present the sociodemographic and clinical characteristics of the participants. Patients with acute PE who subsequently died exhibited a statistically significant decrease in lymphocyte (1.17±0.45 vs. 2.0±0.85; p=0.007) and platelet counts (154±112 vs. 281±117; p=0.003).
- The sociodemographic and clinical characteristics of the participants (N=162).
- Distribution of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and red cell distribution width according to the severity of pulmonary embolism.
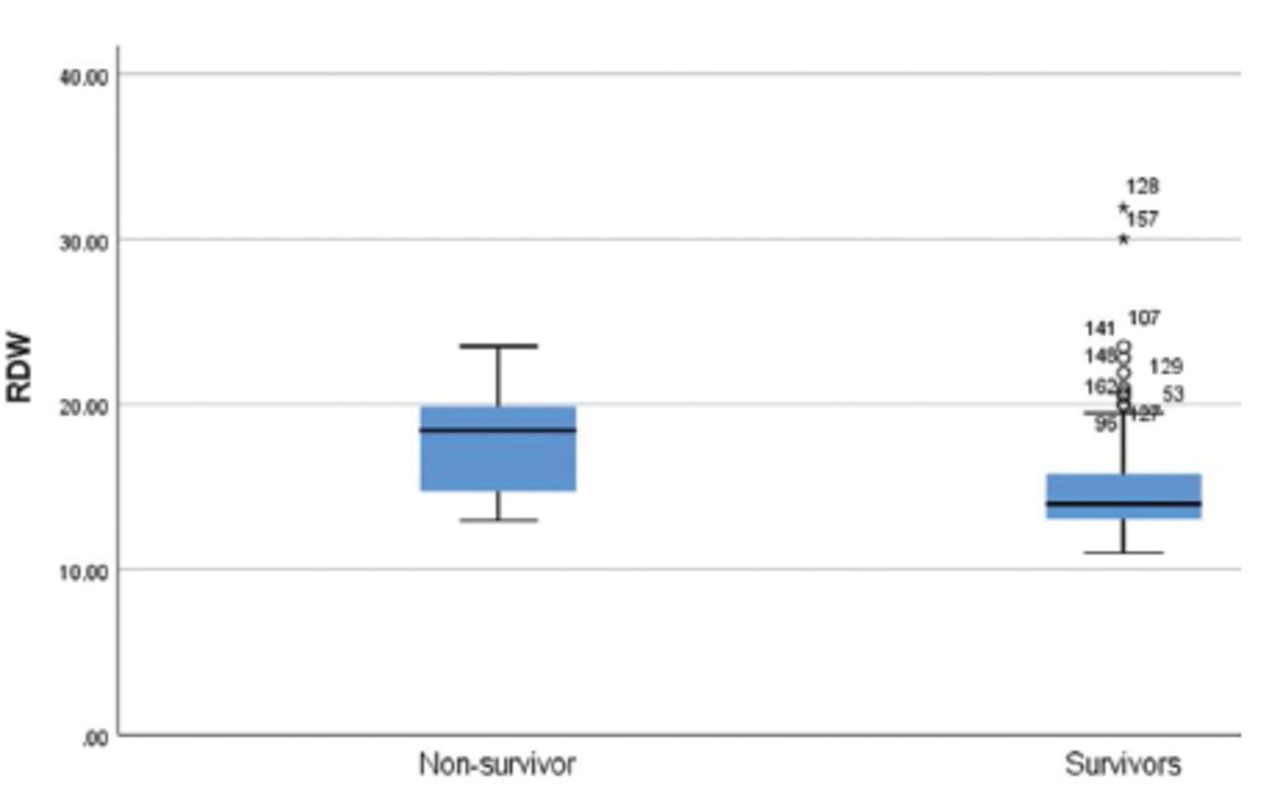
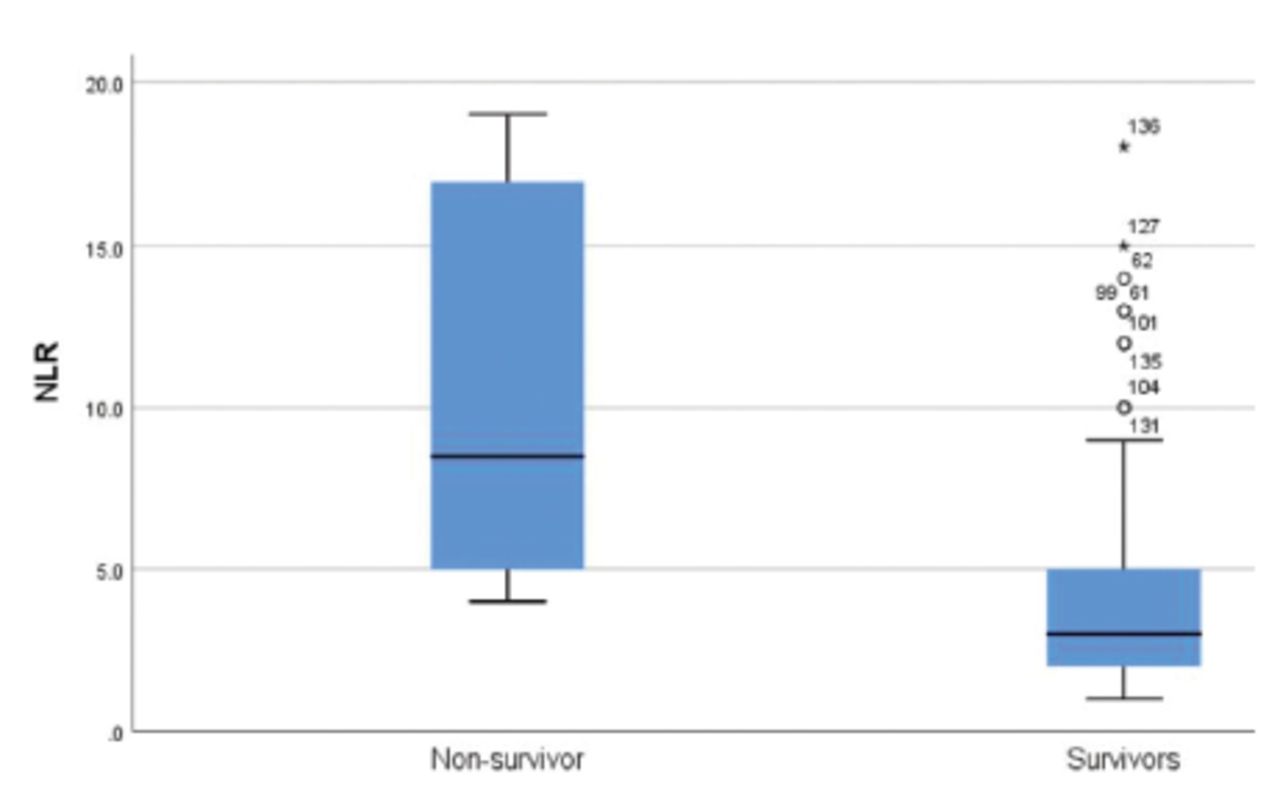
Red cell distribution width was significantly higher in the patients who died (17.82±3.54 vs. 14.97±3.02; p=0.011, Figure 1). The patients who died demonstrated a significantly higher NLR (10.5±6.2 vs. 3.9±3.0; p<0.001, Figure 2) as well. High-risk patients based on the sPESI had significantly higher mortality rate (9.9%) compared to those who low risk (0.0%; p=0.004). The mortality rate was found to be significantly associated with the location of PE, with the saddle location of the PE exhibiting the highest mortality rate (p<0.001). Patients diagnosed with massive PE shown a considerably elevated mortality rate compared to individuals diagnosed with sub-massive or low-risk PEs (p=0.001). The majority of patients (58.6%) had low-risk PE, whereas 36.4% had sub-massive PE and 5% had massive PE.

- Comparison of red cell distribution width (RDW) in patients with acute pulmonary embolism based on the survival and mortality.

- Comparison of neutrophil-to-lymphocyte ratio (NLR) in patients with acute pulmonary embolism based on the survival and mortality.
Table 3 presents the association between PE severity and NLR, PLR, and RDW. Neutrophil-to-lymphocyte ratio was significantly higher in patients with massive PEs (10.6±6.1) than that in those with sub-massive (4.7±3.8) or low-risk PE (3.4±2.3; p<0.001). Similarly, RDW was significantly higher in patients with massive PEs (17.55±3.50) than that in those with sub-massive (15±2.8) or low-risk PEs (14.97±3.18; p<0.05).
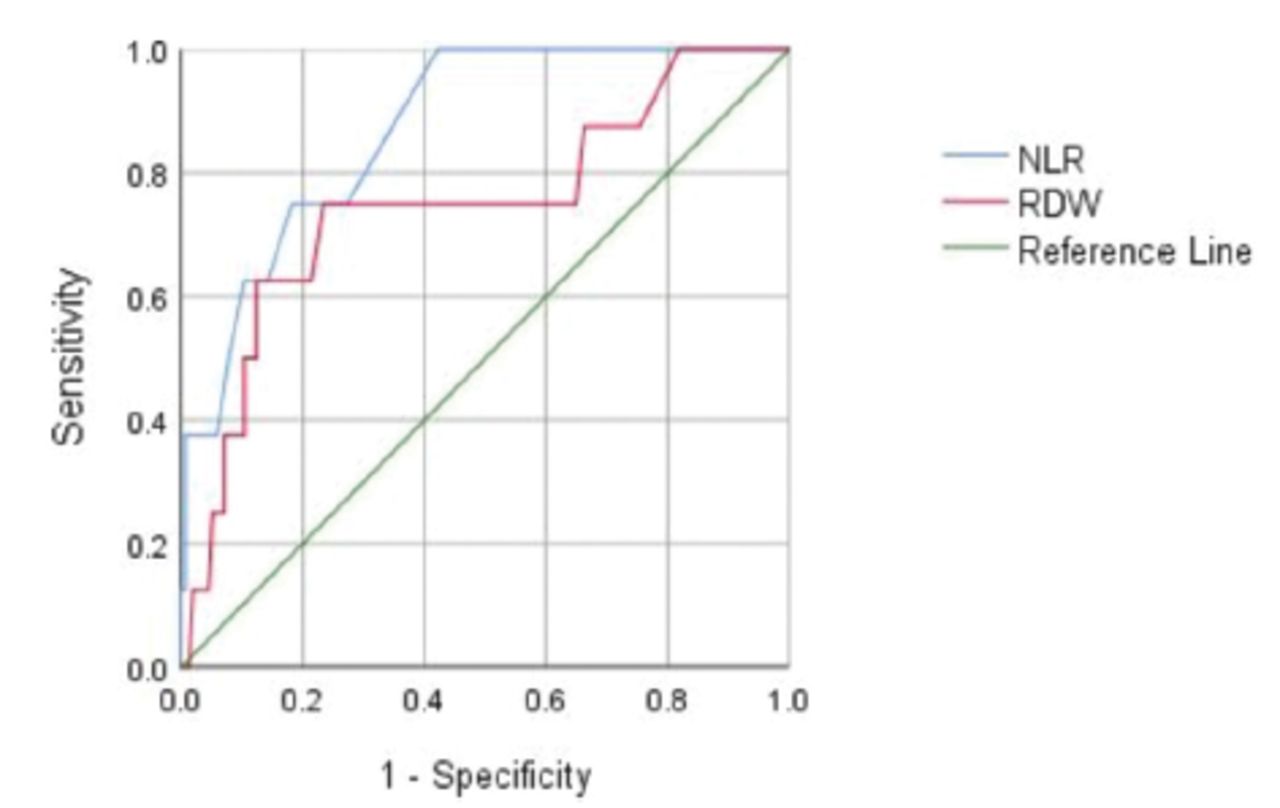
There was an absence of statistically significant variation in PLR between patients with low-risk, sub-massive, and massive PEs (p>0.05). The area under the curve (AUC) for NLR based on the ROC curve analysis was 0.87 (95% confidence interval [CI]: [0.77-0.97]; p<0.001) and for RDW it was 0.75 (95% CI: [0.55-0.94]; p<0.019). At the cut-off value of 5.5, NLR had a sensitivity of 75% and specificity of 82%. At the cut-off value of 18.15, RDW had a sensitivity of 63% and specificity of 88% (Figure 3).

- Receiver operating characteristic curve illustrating the area under the curve sensitivity and specificity of neutrophil to lymphocyte ratio (NLR) and red cell distribution width (RDW) for predicting mortality.
Discussion
In recent years, NLR, RDW, and PLR have been used to predict the prognosis of multiple disorders, such as sepsis and acute heart failure, at the emergency level of care and for the assessment of mood disorders.12-14 Moreover, these factors have wide acceptance due to their availability and low cost. The usefulness of these markers may be attributed to their ability to indicate the severity of the inflammatory process due to underlying diseases.13
Red cell distribution width is a numerical value that describes in percentage the differentiation in the red blood cell size, and its normal value ranges from 12-15%.15 Neutrophil-to-lymphocyte ratio is the ratio between the neutrophil and lymphocyte counts, and its normal value ranges from 0.78-3.53.16 Platelet-to-lymphocyte ratio is the ratio between the platelet and lymphocyte counts, and a higher value of PLR is linked to increased inflammation.17 The findings of our study indicate a statistically significant association between elevated NLR and in-hospital mortality, as observed in the analysis of the 162 patients included in the study (Figure 2). Patients diagnosed with massive PE showed a notably elevated mortality rate compared to individuals diagnosed with sub-massive or low-risk PEs (p=0.001). Furthermore, it was observed that a higher NLR was correlated with increased severity of PE according to the AHA risk stratification for acute PE (Table 3). This finding supports the findings of multiple clinical studies showing that NLR is an inexpensive, fast, sensitive, specific, valuable, routinely ordered, and simple to calculate test that can be used for risk stratification and mortality prediction in patients with acute PE.18,19 The cut-off value for NLR in our study was 5.5, with a sensitivity of 75% and specificity of 82% for predicting all-cause mortality. Other studies have reported similar cut-off ranges, sensitivities, and specificities.18,19
The existing comprehension of the correlation between of a higher NLR and mortality is based on the involvement of inflammation in the development of thrombosis.20 During acute stress, the secretion of corticosteroids and adrenaline increases, thereby decreasing the lymphocyte count and increasing the leukocyte count.21 The more acute and stressful the condition, the higher the NLR is.
The second most significant prognostic factor was RDW. In our study, a significant relationship was observed between RDW, PE severity, and mortality, similar to NRL. Evidence from our study showed that RDW was significantly higher among patients who died (17.82±3.54 vs. 14.97±3.02; p=0.011, Figure 1). The cut-off value in our study was 18.15, with a sensitivity of 63% and specificity of 88%. A study carried out revealed a significant correlation between RDW and mortality occurring during a patient’s hospital stay with a cut-off value of ≥15 and sensitivity of 66% and specificity of 59% for all-cause deaths.22
A previous study reported that patients with massive PEs had significantly higher RDW than those with non-massive PEs, the optimal cut-off value for RDW that had the highest combined sensitivity and specificity was >14 (sensitivity of 72% and specificity of 46%).23 In our study, RDW was higher in patients with massive PE (17.55±3.50) than that in those with sub-massive (15.00±2.80), or low-risk PEs (14.97±3.18, p=0.042).
Severe hypoxia in acute events, such as pneumonia, will induce the bone marrow to produce new large red blood cells under the effect of erythropoietin secretion secondary to hypoxia and stress.24 Platelet-to-lymphocyte ratio can be a useful biomarker for predicting acute PE as it is a part of the systemic inflammatory response (SIR).25 However, the findings of our study showed no significant value of PLR as an indicator of PE severity or mortality (p>0.05). In contrast, another study reported that PLR had a significant prognostic value at a cut-off value of 191 and was associated with high 30-day mortality, with a sensitivity of 60.6% and specificity of 83.2% (p=0.01).19 Low platelet counts were observed in the massive PE group. These patients did not receive anticoagulants or thrombolytic therapy, and their platelet levels were measured at the emergency department level. A previous study showed that the platelet count in massive PE group is lower than submassive and low-risk PE groups.26 In addition, a meta-analysis of platelet indices for the risk stratification of acute PE reported that patients with acute PE had higher mean platelet volume and lower platelet counts.27
To clarify this point, the baseline of the patients must be recorded before the development of PE in further prospective studies. Lastly, based on our cut-off value for predicting all-cause mortality for both NLR (5.5) and RDW (18.15), we suggest using NLR and RDW in establishing a management plan for submassive PE in future prospective studies. This incorporation may help in making decisions regarding thrombolysis therapy for this group. As well as incorporation with other PE risk stratification models may facilitate the choice of treatment disposition.
Study limitations
This study had a small sample size. Moreover, the retrospective design of the study was a limitation. Another limitation of our study was that NLR and PLT had no universal reference for the normal range based on age, gender, and ethnicity. Further studies are required to identify the normal ranges of NRL and PLR in different populations.
In conclusion, NLR and RDW are simple and inexpensive tests that can be carried out at the emergency department level and may indicate prognostic value. Their role as prognostic factors can be explained by their relationship with the severity of inflammation. These factors are independent predictors of mortality and disease severity in patients with acute PE.
Acknowledgment
The authors gratefully acknowledge Editage for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 12, 2023.
- Accepted August 14, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.