


Abstract
Objectives: To assess argyrophilic nucleolar organizer regions (AgNORs) in 60 patients with primary breast carcinoma and evaluated their association with clinical prognostic parameters of breast cancer.
Methods: Argyrophilic nucleolar organizer regions were stained in paraffin sections of the tissues using Ploton’s silver method. For each sample, the number of AgNORs within the nuclei of 100 tumor cells was counted. The average number of AgNORs per nucleus was calculated, and the results were expressed as mean.
Results: The number of AgNORs was significantly higher in breast invasive ductal carcinoma (6.6) compared to benign breast tumors (fewer than 2.0). However, differences in AgNOR counts across different age groups were not statistically significant.
Conclusion: This study suggests that AgNOR counts could be used as a potential procedure for estimating proliferation characteristics in histopathological sections of benign and malignant breast lesions. Argyrophilic nucleolar organizer region counts may also be valuable for identifying high-risk patients and indicating tumor aggressiveness. A larger study with an increased sample size that incorporates both AgNOR numbers and Ki67 scores for assessing cell kinetics is needed to confirm our findings.
Breast cancer is the most common cause of cancer-related death among women worldwide.1 It is frequently diagnosed among the Saudi population, with the incidence of breast cancer in Saudi Arabia increasing in recent years.2 Breast cancer is a multifactorial condition with several risk factors, including previous benign breast disease.3 The most common benign breast lesions include fibrocystic changes, adenosis, and fibroadenomas, which are among the most common benign tumors of the breast. The majority of breast cancers are carcinomas that originate in cells within the ducts or lobules, with invasive ductal carcinoma and invasive lobular carcinoma being the most prevalent types.4
The nucleolus plays a crucial role in regulating cell proliferation and protein synthesis. Rapidly dividing cells and cells with high metabolic activity have prominent nucleoli.5 Cancer cells typically exhibit large, irregular nucleoli.6 Nucleolar organizer regions (NORs) are DNA segments closely associated with nucleoli and contain genes coding for ribosomal RNA, contributing to cellular protein synthesis.7 Nucleolar organizer regions are associated with argyrophilic proteins, and the silver staining technique enables the visualization of NORs in conventional histologic sections by quantifying argyrophilic nucleolar organizer regions (AgNORs) in tumor cells.8 Argyrophilic nucleolar organizer regions serve as indicators of malignancy in certain tumor types.9
Given the significant contribution of nucleolar activity to cell proliferation, this study investigates the potential of AgNORs to provide dynamic information in conventional histologic sections of benign and malignant breast lesions. Numerous studies have suggested that breast cancer dynamics, nucleolar activity, and molecular information based on gene expression patterns offer valuable prognostic information.10-12
Microscopic differentiation of malignant aberrations from benign ones can be challenging, and routine histopathological techniques may not reveal all diagnostically and prognostically significant features. Therefore, it is crucial to propose a simple adjunctive procedure, such as the silver staining method, to study breast cancer dynamics and provide valuable prognostic information. This approach may aid in the accurate and early diagnosis of malignancy.
The aim of the present study is to demonstrate and quantify the mean number of NORs in breast lesions and cancer cells using silver staining methods. Additionally, the study investigated the association between age groups of patients with different breast lesions and the number of NORs.
Methods
This cross-sectional case-control study was carried out at the Clinical Laboratory Department, College of Applied Medical Sciences, Taif University and King Faisal Specialized Hospital, Taif, Saudi Arabia, from January to April 2023. The study involved 60 women with breast cancer and 50 control women with benign breast lesions. Clinicopathological information was collected from patient archives.
We obtained paraffin sections from patients previously diagnosed with breast tumors at the Pathology Department of King Faisal Specialized Hospital, Taif, Saudi Arabia.
The scientific research ethics committee at King Faisal Medical Complex in Taif, Saudi Arabia, approved this study (IRB number: HAP-02-T-123; approval number: 2023-B-14). All personal data in this study were anonymized, and medical data were used solely for this research.
We carried out the silver colloid technique for staining nucleolar organizer region-associated proteins (AgNORs) as described by Ploton with slight modifications.8 Briefly, we cut paraffin sections at 5 microns thickness from formalin-fixed paraffin wax (embedded blocks). We incubated them in an oven at 65°C for one hour, then dewaxed them in xylene, rehydrated them through decreasing grades of ethanol, and thoroughly washed them in distilled water for 5 minutes.
We prepared the AgNOR staining solution by dissolving gelatin at a concentration of 2% w/v in distilled water on a hotplate at 70°C. Then, we added pure formic acid to a final concentration of 1%. We mixed this solution with 2 volumes of freshly prepared 50% aqueous silver nitrate solution. We incubated the sections in the dark with the AgNOR working solution for 60 minutes. The silver colloid was washed off 3 times in distilled water for 5 minutes. The sections were then dehydrated through an ascending series of ethanol concentrations, cleared in xylene, and mounted in DPX.
The morphology, intensity, and spatial relationships of AgNORs on chromosomes vary during the cell cycle. Therefore, in all specimens, we examined 100 cells using a 100X oil-immersion lens and counted the number of AgNOR “dots. Single AgNORs and individual AgNORs within clumps were counted. With magnifications less than 1000x, we were not able to count individual AgNORs within clusters. We expressed results as mean cell counts per case. To eliminate bias, we carried out all counting without the examiner’s knowledge of the diagnosis.
Statistical analysis
Recorded data were analyzed using the Statistical Package for Social Sciences, version 20.0 (SPSS, Chicago, IL, USA). Quantitative data were expressed as mean ± standard deviation (SD). Qualitative data were expressed as frequency and percentage.
Results
This study included 110 females with breast tumors, ranging in age from 18-82 years, with a mean age of 42±14.84 years. Half of the participants (50%) were between 36-51 years old, and approximately 9% were under 20 years old. Among the breast lesion cases, 60 (56.4%) were diagnosed with invasive ductal carcinoma, 33 (29.1%) with fibroadenoma, and 17 (14.5%) with fibrocystic breast changes.
The study investigated the association between age groups and tumor types. Among patients in the middle age group (36-51 years), 58.3% (n=35) were diagnosed with invasive ductal carcinoma, 39.4% (n=13) with fibroadenomas, and 41.3% (n=7) with fibrocystic breast changes. However, statistical analysis using Pearson’s Chi-square test revealed no significant difference between age groups and tumor types (p>0.005, Table 1).
- Age groups and tumors types.
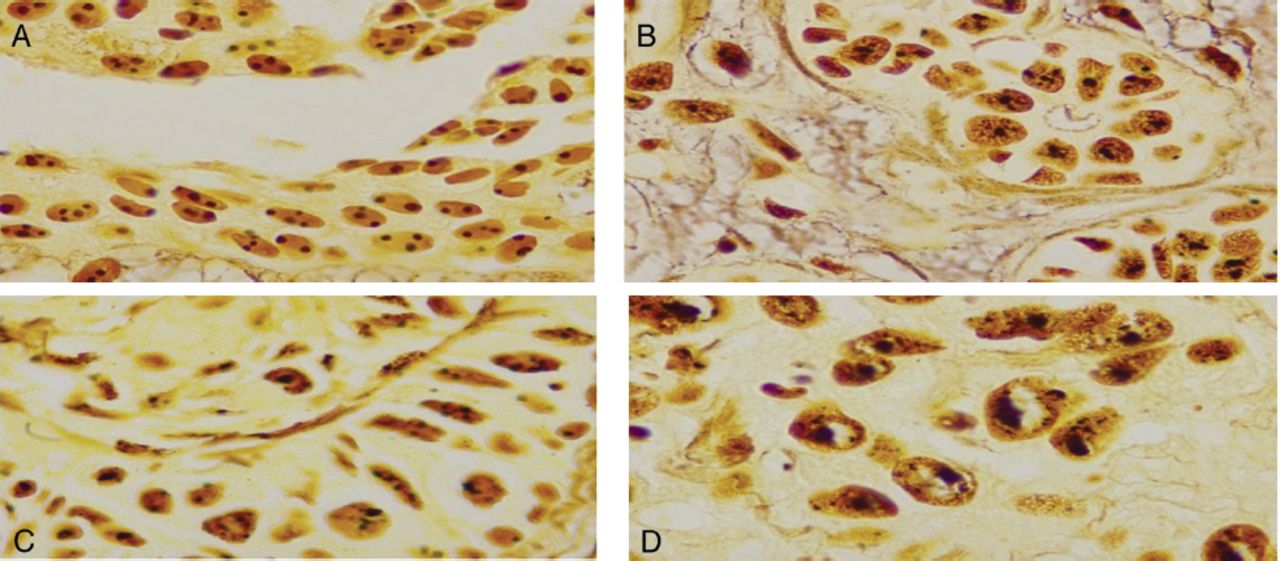
All benign and malignant cells contained black dot-like AgNORs. Cells from fibroadenoma and fibrocystic breast disease exhibited limited small, round, uniform AgNORs within each cell. In contrast, cells exhibiting invasive ductal carcinoma contained numerous AgNORs, often of varying sizes and shapes (Figure 1).

- Argyrophilic nucleolar organizer regions microscopic findings. A) Benign breast fibroadenoma, round regular argyrophilic nucleolar organizer regions (AgNORs) in each nuclues (X1000). B) Fibrocystic disease (benign glands). Small regular AgNORs in each nuclues (X1000). C&D) Breast invasive ductal carcinoma. Argyrophilic nucleolar organizer regions are heterogenous in size, shape, and number. Many nulcei contain large numbers of AgNORs (X1000).
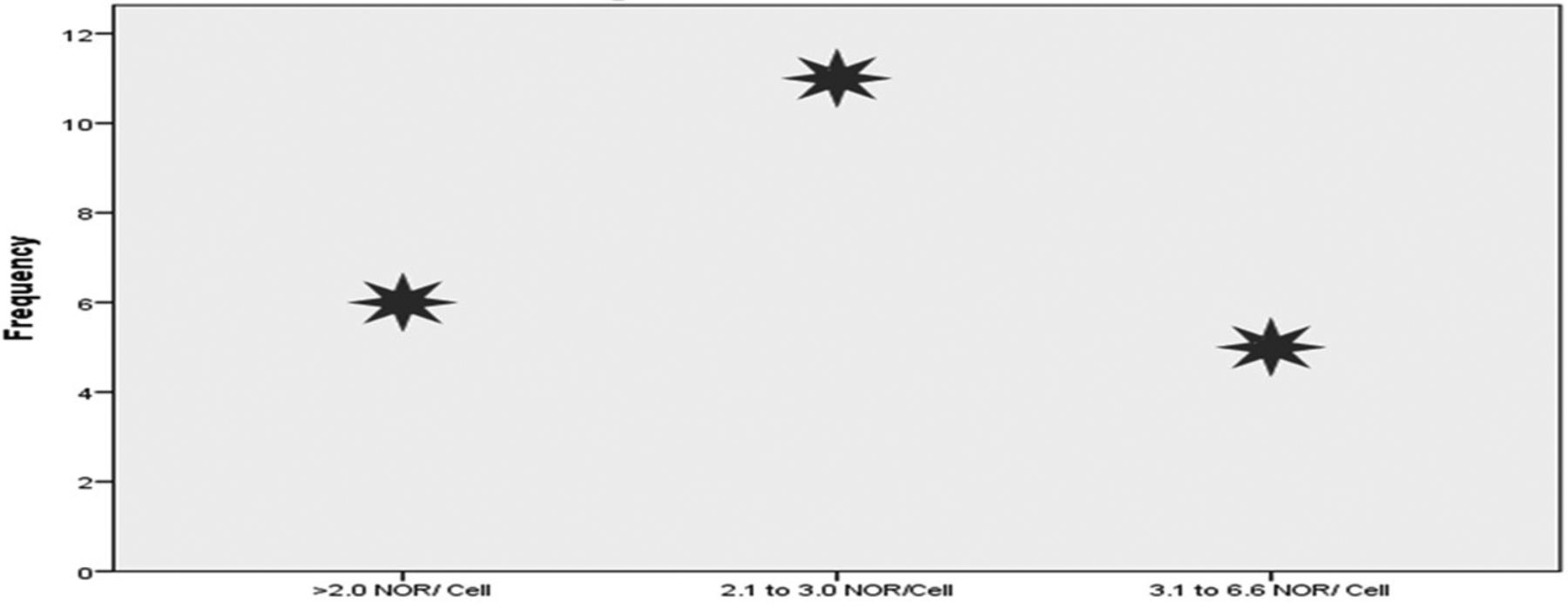
The minimum mean number of NOR per cell was 1.2, observed in fibroadenoma cases, while the maximum mean of 6.6 was reported in invasive ductal carcinoma cases. The overall mean of the means was 2.5 NOR per cell. The distribution of the average mean number of NOR indicated that 50% of NOR counts ranged between 2.1-3.0 NOR per cell (Figure 2).

- Avarage number of nucleolar organizer region/cell. NOR: nucleolar organizer region
The average mean number of NOR ≤2.0 per cell was observed in 40.0% (n=12) of fibroadenoma cases, 36.7% (n=11) of fibrocystic breast changes, and 23.3% (n=7) of invasive ductal carcinoma cases. In contrast, tissue sections with an average NOR count ranging from 3.1-6.6 per cell were predominantly noted in invasive ductal carcinoma cases. Statistical analysis revealed a significant association between the type of breast lesion and the number of NOR per cell, as indicated by Pearson’s Chi-square test (p<0.005, Table 2).
- The average mean number of nucleolar organizer region/cell among different types of breast lesions.
Regarding the average mean number of NOR per cell among benign and cancerous cases, 76.7% (n=23) of benign cases exhibited an average NOR count of ≤2.0 per cell, compared to 23.3% (n=7) of cancerous cases. Conversely, a majority of breast cancer cases (92%, n=23) demonstrated an average NOR count between 3.1-6.6 per cell (Table 3). Pearson’s Chi-square test (p<0.005) indicated a significant difference in NOR counts per cell between breast cancer and benign breast lesions.
- The average mean number of nucleolar organizer region/cell among breast cancer and benign lesion.
Concerning the mean number of NORs per cell among different age groups, 54.5% (n=30) of individuals aged 36-51 exhibited an average NOR count between 2.1-3.0 per cell. In comparison, 9.1% (n=5) of individuals aged under 20 years also fell within this range. We observed no significant differences in the mean number of NORs per cell among the different age groups (Table 4).
- The average number of nucleolar organizer region/cell among different age groups.
Discussion
Nucleolar organizer regions are clusters of nucleolar proteins linked to ribosomal genes that can be verified in histologic tissue with a silver colloid technique, hence the term “silver-staining nucleolar organizer region” (AgNOR). In some tissue sections, the amount of AgNORs per nucleus is linked with cellular proliferation and, originally, with malignant conversion. We examined AgNORs in 110 paraffin-embedded breast tumors consisting of invasive ductal carcinoma, fibroadenoma, and fibrocystic breast changes. Invasive ductal carcinoma had a significantly higher mean AgNOR count than benign breast lesions (p<0.0001). The results of this study are consistent with the findings reported by Borgiani et al13 and Krüger et al14 in breast lesions. Although this study found a wide scatter of AgNOR amounts in carcinomas, there was a clear difference between the mean amounts in benign and malignant breast lesions.
Breast cancer carries out differently in diverse people, and the behavioral differences in the tumor impact the final result of the disease. Indicators of tumor behavior comprise proliferative measures and DNA ploidy. Numerous methods for evaluating these markers have been demarcated.15-17 The amount of AgNORs per nucleus has lately been presented as a good indicator of the proliferative activity of several tumors.18,19 The AgNOR amount showed a stable increase from benign to malignant conversion in tumors. In benign lesions (fibroadenoma and fibrocystic breast changes), the AgNOR count is typically 1.0-2.0 per nucleus, and any count greater than 2.0 is indicative of increased DNA aneuploidy.20
This study establishes that an AgNOR count greater than 3.0 is strongly indicative of malignancy. This information may be applied to identifying individuals at high risk and to determining which lesions are suspicious. Consequently, patients with AgNOR counts greater than 3.0, even if they have histologically benign tumors, require earlier investigation.
Researchers have defined AgNOR count as a predictive parameter in hematological malignancies and many solid neoplasia, as well as breast cancer.21-23 The results reported in the literature are inconsistent concerning the stage and type of the tumor and the amount of AgNOR. Since a higher AgNOR amount reflects greater cellular proliferation, we expect that it could serve as a prognostic marker for aggressive neoplasia.
Breast cancer patients diagnosed among young age group women experience a more aggressive disease course and have poorer survival outcomes compared to those diagnosed among the old age group.24,25 In this study, the majority of the study group comprised individuals aged between 36-51 years, with over half diagnosed with invasive ductal carcinoma. Our study investigated the validity of AgNOR counts in a young, population-related breast cancer group. However, the age-related biological differences underlying this disparity are not well described. The current study did not find any association between AgNOR counts and the age of the study group, corroborating the findings of Raymond et al26 that AgNOR counts do not correlate with age groups. The differences among several studies could be attributed to variances in sample sizes and study groups.
Study limitations
This study primarily focused on the quantification of AgNORs without incorporating additional molecular markers such as Ki67 or other well-established proliferation indices. The absence of these molecular markers limits the ability to comprehensively assess cellular proliferation. Future research should aim to integrate AgNOR quantification with molecular markers to provide a more thorough evaluation of proliferative activity.
In conclusion, although the precise nature and function of AgNORs continue to be undetermined, the present study indicates that breast tumors with a higher AgNOR count, even in cases of fibroadenoma and fibrocystic changes and more than 3 AgNORs per nucleus, necessitate careful investigation. This study also proposes that AgNOR counts could be a valuable tool for assessing proliferation features in histopathological sections of benign and malignant breast tumors. Argyrophilic nucleolar organizer region counts may be useful for categorizing high-risk patients and indicating tumor aggressiveness. A larger study with an increased sample size, incorporating both AgNOR counts and Ki67 scores for the assessment of cell kinetics, is necessary to confirm our findings.
Acknowledgment
The authors gratefully acknowledge the Deanship of Graduate Studies and Scientific Research, Taif University, Taif, Kingdom of Saudi Arabia, for funding this study. The authors also would like to thank American Manuscript Editors for thier English language editing.
Footnotes
Disclosure. This study was funded by the Deanship of Graduate Studies and Scientific Research, Taif University, Taif, Kingdom of Saudi Arabia.
- Received June 4, 2024.
- Accepted August 15, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.