


Article Figures & Data
Figures
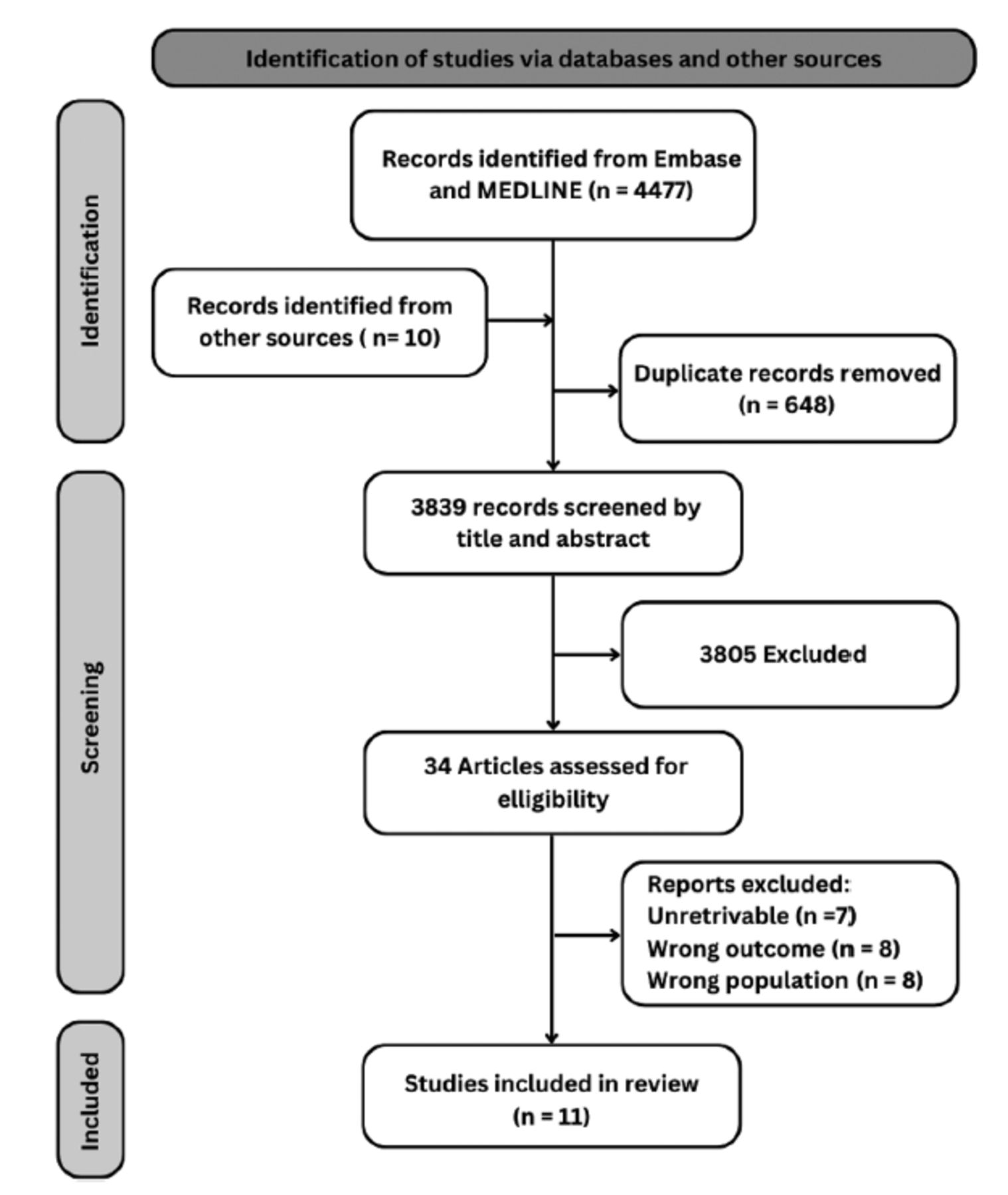
- Figure 1
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart for study selection.
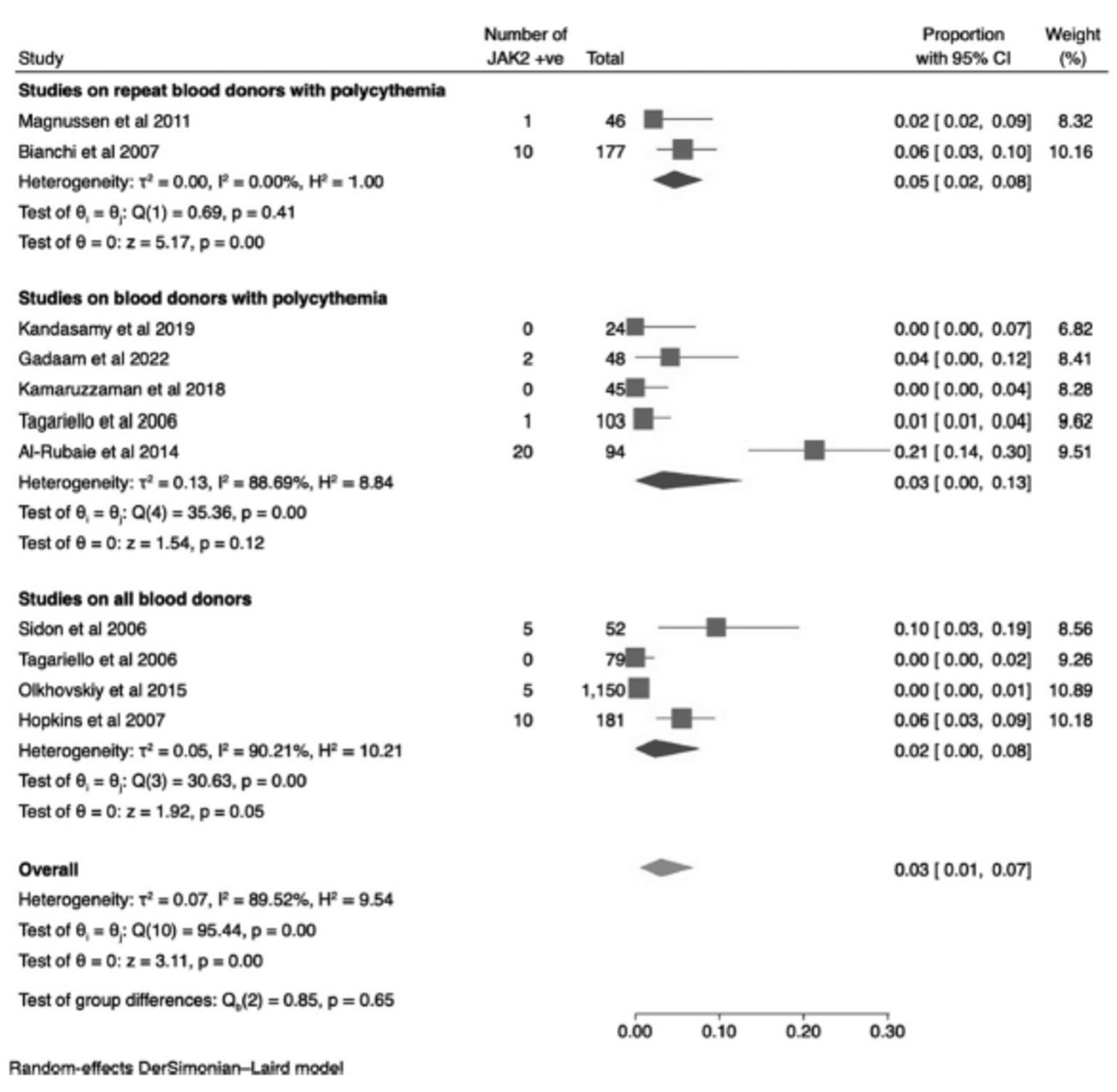
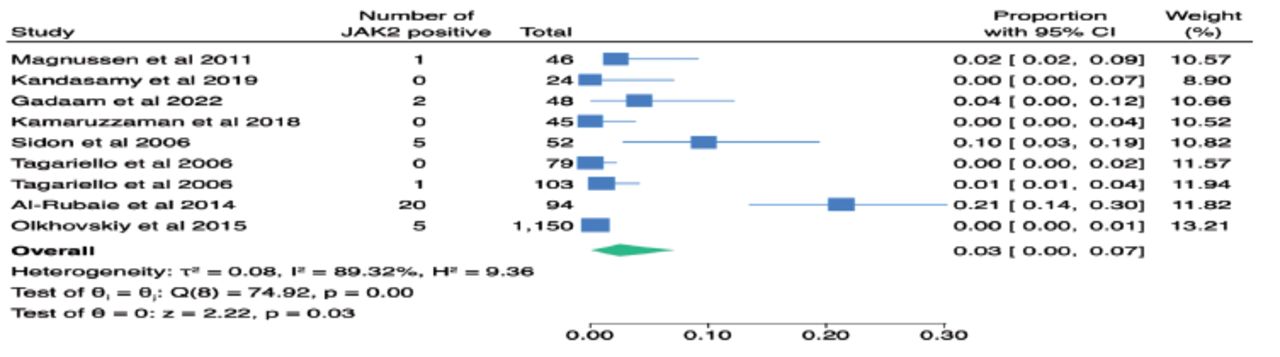
- Figure 2
- Forest plot of the prevalence of JAK2V617F mutation among blood donors (overall, and subgroups).
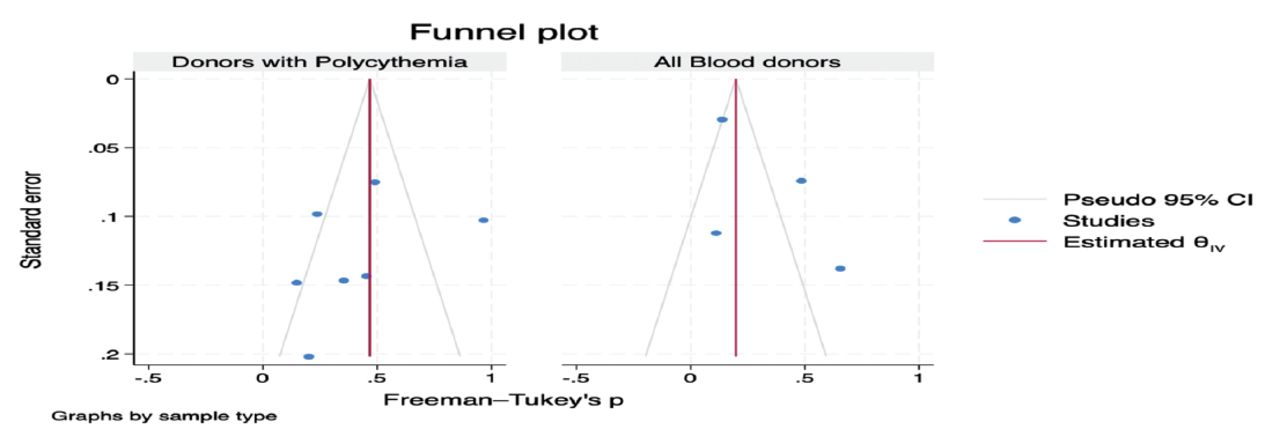
- Appendix 5
- Egger’s funnel plot of JAK2V617F mutation among blood donors
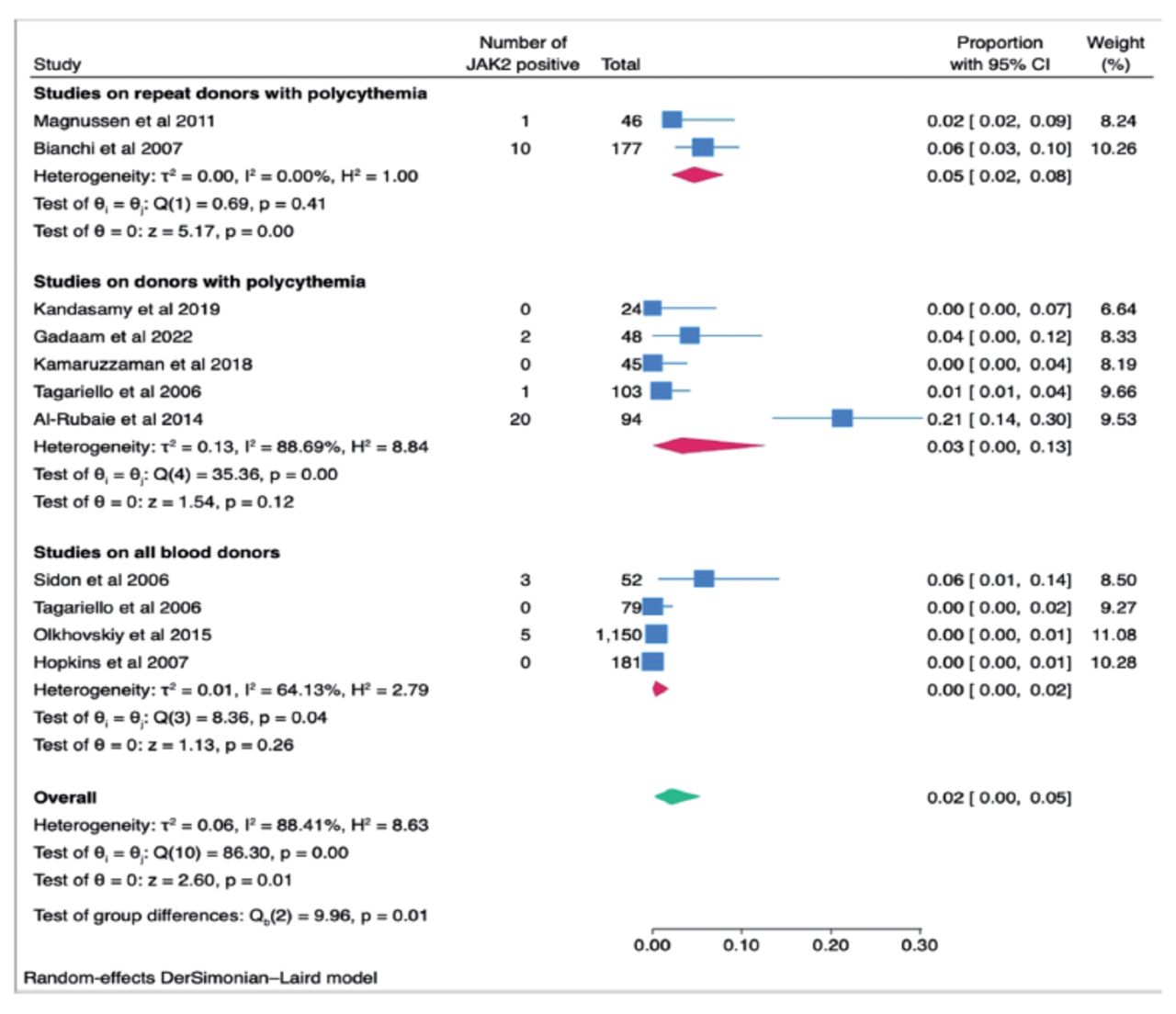
- Appendix 6
- Results of post-hoc analysis after removing studies that reported very low JAK2V617F mutation allele levels <1% among blood donors (overall, and subgroups).
- Appendix 7
- Results of post-hoc analysis after removing abstracts.
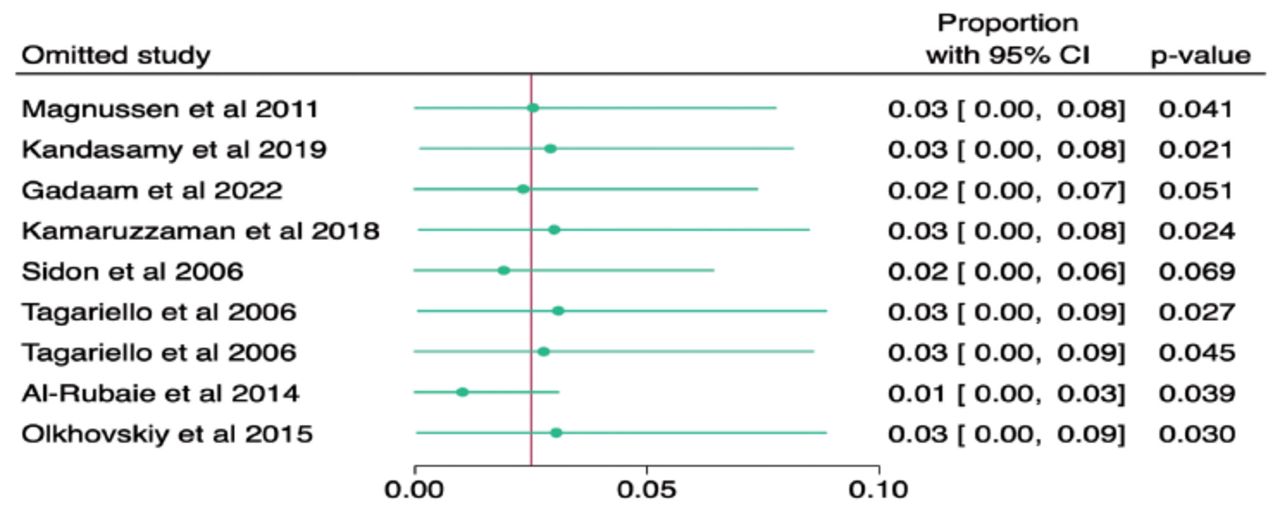
- Appendix 8
- Results of the leave one out meta-analysis.






Tables
- Table 1
- Characteristics of studies included in the meta-analysis to assess prevalence of JAK2 mutation among blood donors.
No. References/Author Study design Number of centers Country Study duration 1 Zanella et al 198613 Case-control Single Italy Unspecified 2 Tagariello et al 200610 Prospective cohort Single Italy 1 year 3 Sidon et al 200617* Cross-sectional Unspecified Belgium Unspecified 4 Bianchi et al 200718* Prospective cohort Single Italy Unspecified 5 Magnussen et al 201319 Prospective cohort Single Denmark 2 years 6 Al-Rubaie et al 201420 Prospective cohort Single Iraq 7 months 7 Olkhovskiy et al 20159 Prospective cohort Single Russia 1 month 8 Kamaruzzaman et al 201811 Prospective cohort Two Malaysia 9 months 9 Kandasamy et al 201921 Prospective cohort Single India 4 months 10 Gadaam et al 202222 Prospective cohort Single India 18 months 11 Hopkins et al 200712* Prospective cohort Single USA Unspecified No. References/Author Sample source and cutoffs used Total sample size Individuals with JAK2 mutation +ve/total number tested (%) Individuals diagnosed with PV JAK2 analysis assay type 1 Zanella et al 198613 Consecutive repeat blood donors 81 No testing for JAK2 3 NA 2 Tagariello et al 200610 Out of 5,636 repeat donors, 103 (1.8%) had high HCT (>50% for M and >46% for F), and 79 regular donors as control. 103 High HCT / Normal HCT 79 1/182 (0.55%) 0 ARMS amplification refractory mutations system PCR 3 Sidon et al 200617* Healthy blood donors 52 (57 recruited but 5 samples rejected) 5/52 (9.60%) NA Quantitative PCR 4 Bianchi et al 200718* Consecutive repeat blood donors with (HCT > 0.47 for M and > 0.42 for F or platelet count >300x109/L) on at least 2 occasions within 1 year. 177 10/177 (5.65%) NA Allele-specific (PCR) 5 Magnussen et al 201319 Repeat Blood donors with Hb >16.5 g/dl for F and > 18.5 g/dl for M. 46 1/46 (2.20%) 2 Unspecified 6 Al-Rubaie et al 201420 Male blood donors with HCT ≥ 48% 94 20/94 (21.30%) NA Allele-specific Oligonucleotide Real-time quantitative PCR 7 Olkhovskiy et al 20159 Healthy blood donors 1150 5/1150 (0.65%) NA Allele-specific real time (PCR-RV) 8 Kamaruzzaman et al 201811 Out of 2238 blood donors, 175 (7.8%) blood donors had high Hb > 16.5g/dl for M,> 13.8g/dl for f). 45 of these donors (highest counts) were then tested for JAK2 mutation. 175 0/45 (0%) NA Allele-specific Oligonucleotide PCR 9 Kandasamy et al 201921 Out of 7,076 donors, 112 males with Hb ≥ 18 g/dL were deferred and considered for the study.108 donors with persistent Hb ≥ 18 g/dL at least after 1 month, with no secondary causes of polycythemia were included. 108 (but only 24 were tested) 0/24(0%) NA Real-time PCR 10 Gadaam et al 202222 Out of 13,798 donors, 185 were deferred for Hb > 18 g/dl, those with persistent Hb >18 g/dl after 3 months were tested for JAK2 48 2/48 (4.10%) NA Real-time PCR 11 Hopkins et al 200712* Healthy Blood donors 181 0/181 (0%) NA Real-time quantitative PCR M: males, F: females, HCT: hematocrit, Hb: hemoglobin, PCR: polymerase chain reaction, PV: polycythemia vera, USA: United States of America, JAK2: JAK2V617F
↵* Abstract studies.
- Appendix 1
- Ovid MEDLINE(R) and Epub ahead of print, in-process, in-data-review and other non-indexed citations, Daily and Versions 1946 to August 18, 2023
# Searches Results 1 (JAK Kinases or janus kinases or JAK Kinase or janus kinase or JAK2 Protein Tyrosine Kinase or JAK 2 Protein Tyrosine Kinase or JAK-2 Protein Tyrosine Kinase or v617fjak2 or v617f or Janus Kinase 2).mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms, population supplementary concept word, anatomy supplementary concept word] 21855 2 (erythrocytoses or erythrocytosis or polycythemia or polycythemias).mp. or Hematocrit/ or exp Blood Cell Count/ or exp Erythrocyte Indices/ 196065 3 1 or 2 215766 4 exp Blood Donation/ or (blood donor or blood donors or donor, blood or donors, blood).mp. or Blood Donation/ or exp Blood Donors/ 36878 5 3 and 4 1482 # Searches Results 1 (JAK Kinases or janus kinases or JAK Kinase or janus kinase or JAK2 Protein Tyrosine Kinase or JAK 2 Protein Tyrosine Kinase or JAK-2 Protein Tyrosine Kinase or v617fjak2 or v617f or Janus Kinase 2).mp. [mp=title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword heading word, floating subheading word, candidate term word] 54278 2 exp Blood Donation/ or (blood donor or blood donors or donor, blood or donors, blood).mp. or Blood Donation/ or exp Blood Donors/ 55355 3 (erythrocytoses or erythrocytosis or polycythemia or polycythemias).mp. or Hematocrit/ or exp Blood Cell Count/ or exp Erythrocyte Indices/ 485352 4 1 or 3 531816 5 2 and 4 2996 References/Author Mean age (range) Proportion of males JAK2 allelle load Hb range (mean+SD) HCT range (mean+SD) WBC range (mean+SD) RBC range (mean+SD) PLT range (mean+SD) 1 % smokers 1 Zanella et al 1986 Median 39 (18-64) 81/81 NA Not reported 0.49-0.54 Not reported Not reported Not reported 62% 2 Tagariello et al 2006 44.5±11.3 (M high HCT) 59/79 control Not reported Not reported 49.7±1.3 (M high HCT) 6.5±1.3 (M high HCT) Not reported 226-277 Not reported 44.5±11.3 (M control) 84/103 high HCT 43.8±1.87 (M control) 5.6±1.2 (M control) 3 Sidon et al 2006 38 (23-25) Not reported <10 copies 13.9-16.9 Not reported Not reported Not reported Not reported Not reported 4 Bianchi et al 2007 45 median (19-66) 92/177 Not reported 16.6-20.3 42-47% (44.5%) 4.8-9.2 Not reported 300-454 (median 338) Not reported 5 Magnussen et al 2011 47 (27-66) 13/46 37% 13.5-16.1 42-57 (49.5%) 4.2-16.3 Not reported 147-449 84% 6 Al-Rubaie et al 2014 NA (21-62) 94/94 Not reported NA (52.5±3.9) 9.7±2.7 5.9±0.4 (331±124.6) 84%, smoking index more than 10 in 28% 7 Olkhovskiy et al 2015 39 (31—53) 752/1150 0.07 to 2.58%. 111- 178 g /L Not reported 3.2 – 12.9 Not reported 97 - 527 Not reported 8 Kamaruzzaman et al 2018 22.66 (17-55) 92/175 Not reported 19.1 ± 1 37.2-55.4 % (47.64±4.20) 3.2-20.1 (8.20 ± 2.36) 4.3-7.5 (5.48±0.56) 159 - 468 28% 9 Kandasamy et al 2019 31.4 (18-56) 108/108 Not reported 16-23.23 (mean 18.23±1.19) 49.2-73.6 (56.2 ± 4.03) 4.4 - 11.4 4.9-7.5 94- 328 24% 10 Gadaam et al 2022 31.2 (20–50) 48/48 Not reported 13.9-19.1g/dl (15.9±1.52) 51.9–83.3% (58±5.02), 3.99–10.8 (7.8±1.5) 4.35–8.43 (6.2±0.6) 120–450 (227±57.2) Not reported 11 Hopkins et al 2007 44 (17-77) 104/181 <1% NA Not reported Not reported Not reported Not reported Not reported SD: standard deviation, NA: not available, HCT: hematocrit, JAK2: JAK2V617F, Hb: hemoglobin, WBC: white blood cells, RBC: red blood cells, PLT: platelet
No. Study Selection Comparability Outcome Total score Abstract or full article 1 Zanella et al 1986 ** * ** 5 full article 2 Tagariello et al 2006 **** * *** 8 full article 3 Magnussen et al 2011 **** * *** 8 Full article 4 Al-Rubaie et al 2014 *** * *** 7 full article 5 Olkhovskiy et al 2015 **** ** *** 9 Full article 6 Kamaruzzaman et al 2018 *** * *** 7 full article 7 Kandasamy et al 2019 ** * *** 6 full article 8 Gadaam et al 2022 **** * *** 7 full article 9 Sidon et al 2006 *** ** *** 8 Abstract/letter 10 Bianchi et al 2007 *** * *** 7 Abstract 11 Hopkin et al 2007 **** ** *** 9 Abstract Title Diagnostic criteria PVSG 1975 Major criteria A1 Raised RCM, male >/= 36 ml/kg, female >/= 32 ml/kg A2 Normal arterial oxygen saturation >/= 92% A3 Splenomegaly on palpation Minor criteria B1 Platelets < 400 x109/l B2 WBC >12 x109/l B3 Elevated leuocyte alkaline phosphatase score Diagnosis A1 + A2 + A3 establishes PV A1 + A2 + two of category B establishes PV World Health Organization Classification 2001 Major criteria A1 Increased red cell mass >25% above mean normal value or Hb >18.5 g/dL in men, Hb >16.5 g/dL in women A2 Absence of secondary erythrocytosis A3 Splenomegaly on palpation A4 Clonal evidence other than Ph-positive or BCR/ABL A5 Spontaneous EEC Minor criteria B1 Platelets > 400 x109/l B2 Leukocytes > 12 x109/l B3 Bone marrow biopsy with typical PV features Increased cellularity with trilineage myeloproliferation and clustering of small to giant (pleiomorphic) megakaryocytes B4 Low serum erythropoietin level Diagnosis A1+A2+any other from A A1+A2+two from B British Society of Hematology Guidelines for the diagnosis, investigation and management of polycythaemia/erythrocytosis 2005 Major criteria A1: Raised red cell mass (>25% above mean normal predicted value) or Hct>/= 0.60 males;>/= 0.56 females A2: Absence of cause for secondary erythrocytosis (consider possibility of dual pathology) A3: Palpable splenomegaly A4: Clonality marker, i.e. acquired abnormal marrow karyotype Minor criteria B1: Thrombocytosis (platelet count >400x109/l) B2: Neutrophil leucocytosis (neutrophil count >10x109/l in non-smokers; >12.5x109/l in smokers) B3: Splenomegaly (demonstrated on isotope/ultrasound scanning) B4: Characteristic BFU-E growth or reduced serum erythropoietin Diagnosis A1 + A2 + A3 or A4 establishes PV A1 + A2 + any 2B criteria establishes PV Modified diagnostic criteria for polycythemia vera from the British Committee for Standards in Hematology criteria 2007 JAK2-positive polycythaemia vera A1 High haematocrit (>0.52 in men, >0.48 in women) OR raised red cell mass (>25% above predicted) A2 Mutation in JAK2 Diagnosis requires both criteria to be present JAK2-negative polycythaemia vera Major criteria A1 Raised red cell mass (>25% above predicted) OR hematocrit >/= 0.60 in men,>/= 0.56 in women A2 Absence of mutation inJAK2 A3 No cause of secondary erythrocytosis A4 Palpable splenomegaly A5 Presence of an acquired genetic abnormality (excluding BCR-ABL) in the hematopoietic cells Minor criteria B1 Thrombocytosis (platelet count >450x109/l) B2 Neutrophil leucocytosis (neutrophil count > 10x109/l in non-smokers; >12.5x109/l in smokers) B3 Radiological evidence of splenomegaly B4 Endogenous erythroid colonies or low serum erythropoietin Diagnosis requires A1 + A2 + A3 + either another A or two B criteria 2008 World Health Organization diagnostic criteria Major criteria 1 Hemoglobin > 18.5 g/dl (men), > 16.5 g/dl (women) or Hemoglobin or Hematocrit >99th percentile of reference range for age, sex or altitude of residence or Hemoglobin >17 g/dl (men), >15 g/dl (women) if associated with a sustained increase of >/=2 g/dl from baseline that cannot be attributed to correction of iron deficiency or Elevated red cell mass >25% above mean normal predicted value 2 Presence of JAK2V617F or similar mutation Minor criteria 1 BM trilineage myeloproliferation 2 Subnormal serum Epo level 3 EEC growth Diagnosis requires meeting either both major criteria and one minor criterion or the first major criterion and 2 minor criteria The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia Major criteria 1. Hemoglobin >16.5 g/dL in men Hemoglobin >16.0 g/dL in women Or, Hematocrit >49% in men Hematocrit >48% in women Or, Increased red cell mass (RCM) 2. BM biopsy showing hypercellularity for age with trilineage growth (panmyelosis) including prominent erythroid, granulocytic, and megakaryocytic proliferation with pleomorphic, mature megakaryocytes (differences in size) 3. Presence of JAK2V617F or JAK2 exon 12 mutation Minor criterion Subnormal serum erythropoietin level Diagnosis of PV requires meeting either all 3 major criteria, or the first 2 major criteria and the minor criterion. Criterion number 2 (BM biopsy) may not be required in cases with sustained absolute erythrocytosis: hemoglobin levels >18.5 g/dL in men (hematocrit, 55.5%) or >16.5 g/dL in women (hematocrit, 49.5%) if major criterion 3 and the minor criterion are present. The 5th edition of the World Health Organization Classification of Hematolymphoid Tumours 2022 Major criteria 1. Hemoglobin >16.5 g/dL in men Hemoglobin >16.0 g/dL in women Or, Hematocrit >49% in men Hematocrit >48% in women 2. BM biopsy showing hypercellularity for age with trilineage growth (panmyelosis) including prominent erythroid, granulocytic, and megakaryocytic proliferation with pleomorphic, mature megakaryocytes (differences in size) 3. Presence of JAK2V617F or JAK2 exon 12 Mutation Minor criterion Subnormal serum erythropoietin level Diagnosis of PV requires meeting either all 3 major criteria, or the first 2 major criteria and the minor criterion. Criterion number 2 (BM biopsy) may not be required in cases with sustained absolute erythrocytosis: hemoglobin levels >18.5 g/dL in men (hematocrit, 55.5%) or >16.5 g/dL in women (hematocrit, 49.5%) if major criterion 3 and the minor criterion are present.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.