


Abstract
Objectives: To evaluate the safety and feasibility of the cable-transmitted, magnetically controlled capsule endoscopy (CT-MCCE) system for examining the esophagus and stomach.
Methods: A pilot study was carried out at the endoscopy facility of Peking University First Hospital; 30 volunteers were enrolled between September and November 2022. All participants were instructed to swallow the CT-MCCE capsule. An external magnetic robot arm was utilized to manipulate the capsule endoscope with string-facilitated control of the endoscope. This study assessed gastric preparation, safety, maneuverability, and mucosal visualization.
Results: The participants exhibited favorable reactions to the gastric preparation and examination, with no reported adverse effects, and the average duration of the gastric examination was 29.5±6.63 minutes. The gastric cavity cleanliness assessment revealed a good rating in 25 participants (83.3%) and a moderate rating in 5 participants (11.8%). TheCT-MCCE demonstrated good maneuverability in all 30 subjects (100%).The analysis of visualization indicated that more than 75% of the gastric mucosa was discerned in 79.4% of the participants (27 individuals), whereas 50% to 75% was visualized in 20.6% of the participants (7 individuals).
Conclusion: This study substantiates the feasibility and safety of employing magnetically controlled capsule endoscopy with cable transmission for the evaluation of human stomach and esophagus.
Upper gastrointestinal diseases pose significant medical and economic challenges globally, particularly in East Asian nations like Japan, Korea, and China.1-3 Esophagogastroduodenoscopy (EGD) is essential for diagnosing and treating upper gastrointestinal conditions. However, conventional EGD consistently causes discomfort for patients and thus decreases compliance. Despite the application of anesthesia enhances patient adherence to medical procedures, it is imperative to consider the possible adverse effects associated with pharmacological agents as well as the financial implications of escalating healthcare expenditures.
Capsule endoscopy (CE) is a pragmatic substitute for individuals devoid of considerable distress and has been utilized in recent decades for clinical assessment of small intestine-associated ailments and has been demonstrated to be secure and efficacious.4,5 Magnetically controlled capsule endoscopy (MCCE) is an innovative technique utilized for stomach examinations. The diagnostic accuracy and safety of MCCE have been proven by several related studies and validated by the expert consensus on MCCE.6-10 Nevertheless, the MCCE systems that are currently in clinical use still have some limitations. The capsule often traverses the esophagus quickly, hindering comprehensive examination of the esophageal mucosa and dentate line. Second, the magnetic force is not stable enough to avoid accidental capsule evacuation to the duodenum, which is driven by gastric peristalsis. Finally, although rare, there is still a risk of capsule retention.
Recently, a new cable transmission MCCE (CT-MCCE) system has been developed. Compared with conventional MCCE systems, CT-MCCE, with the help of a linked electric wire, can provide a detailed examination of the esophageal mucosa and dentate line. The attached wire aids in moving the capsule within the gastric cavity. After the procedure, the cable transmission capsule can be pulled out of the digestive tract to avoid retention risk. This preliminary pilot study assessed the feasibility and safety of the innovative CT-MCCE system in subjects who are considered healthy volunteers.
Methods
This study represents as a preliminary investigation within a multi-center prospective framework. The Institutional Review Board of Peking University First Hospital endorsed the study protocol, and informed consent was acquired from all participants.
A pilot study with 30 volunteers was carried out at the in an endoscopy center at Peking University First Hospital, Beijing, China from September to November 2022. The inclusion criteria required healthy volunteers aged 18 to 75 years without significant abdominal symptoms, no medication history, or history of abdominal surgery. Volunteers with implanted metal foreign bodies or medical devices susceptible to magnetic fields were excluded. Following an 8-hour fasting period, participants consume a solution comprising 600 mg of simethicone, 20,000 units of Dexamethasone granules, and 2 g of sodium bicarbonate, all solubilized in 50 ml of water. In the 10 minutes (min) preceding the evaluation, the participant ingests between 500 and 1,000 ml of water until they reach a state of satiety. Five minutes prior to the evaluation, participants receive a pharyngeal anesthetic via lidocaine spray (Guangzhou Xiangxue Pharmaceutical Co., Ltd., China). The subjects were directed to ingest a single sterile capsule accompanied by a minimal volume of water. The investigators enhanced the visualization of the esophagus and dentate line through the manipulation of the interconnected wires to modulate the velocity of the capsule’s movement subsequent to its entry into the esophagus.
According to our protocol, the capsule was first guided into the duodenal bulb to inspect the duodenal mucosa. The electric wire subsequently retracted the capsule into the stomach. The whole gastric cavity was observed in the following order: pylorus, antrum, angulus, body, fundus, and cardiac. If distension was inadequate, additional water was ingested again. Images were taken from various angles after typical landmarks were identified. After the gastric preparation was completed, the CT-MCCE maneuverability and mucosal visualization were graded by the investigators according to the ease or difficulty of each process. Participants completed a questionnaire evaluating discomfort and acceptance of the CT-MCCE procedure.
The gastric preparations were classified into 3 grades based on tissue cleanliness: good (transparent fluid, <5% mucosa coverage by contents), moderate (slightly opaque fluid, 5%-10% mucosa coverage), and poor (opaque fluid, >10% mucosa coverage).
The investigator assessed the maneuverability of the CT-MCCE as good, moderate, or poor. The CT-MCCE was classified as ‘good’ if it precisely followed control to the anatomical landmark, ‘moderate’ if it moved toward the landmark but not precisely, and ‘poor’ if it did not follow control. Observation of the dentate line and duodenal bulb, which is not a routine step for conventional MCCE, was also evaluated as an indicator of maneuverability.
Mucosal visualization was evaluated via a subjective scoring system with 3 grades (1, 2, and 3) for each anatomical landmark, including the upper, middle, and lower esophagus, body, fundus, antrum, angulus, cardia, pylorus of the stomach, and duodenal bulb. A visualization score of one indicated that less than 70% of the mucosa could be clearly observed, a visualization score of 2 indicated that 70–90% of the mucosa could be clearly observed, and a visualization score of 3 indicated that more than 90% of the mucosa could be clearly observed. Mucosal visualization is deemed good with a score exceeding 27, moderate with a score ranging from 20 to 27, and poor with a score below 20. The evaluation of mucosa visualization was completed by 2 investigators according to the images and videos of the CT-MCCE process.
Safety was evaluated according to the occurrence of adverse events and tolerability to the subjects through the questionnaire.
The CT-MCCE system
The cable transmission MCCE system, innovatively engineered by Shan Xing Medical Technology Co., Ltd., includes a capsule endoscope, an electrical interconnecting cable, a mechanical handle with guiding magnets, a data acquisition device, and a computer workstation equipped with real-time observation software (Figure 1). The operational principle of the guiding apparatus facilitates the movement of capsules towards one another through the utilization of a permanent magnetic handle that engages with a magnet embedded within the capsule. Moreover, the flexibility of the electric wire enables capsule mobility in both directions. The device uses multi-joint support arm technology to facilitate the movement of the magnet handle on the surface of the abdomen. With the assistance of the magnet handle, the capsule can achieve arbitrary spatial and angular movement in 4π space and move freely in the upper digestive tract.

- The Cable Transmission Magnetically Controlled Capsule Endoscope system. A) Disposable sterile capsule endoscope. B) The Image Processor. C) The front view of the magnetic-controlled capsule system.
Statistical analysis
Data analysis utilized IBM SPSS Statistics for Mac, version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means ± SDs or absolute numbers and proportions. Categorical variables were analyzed using the chi-square test or Fisher’s exact test. Statistical significance was determined as 2-tailed with P-values under 0.05. Data analysis utilized IBM SPSS Statistics for Mac version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean±standard deviation or absolute numbers and proportions. Categorical variables were analyzed by Chi-square test or Fisher’s exact test. Statistics were performed using the two-tailed method, with P-values of less than 0.05 showing significant differences.
Results
A successful stomach preparation and capsule swallowing was performed in all subjects between October 2022 and March 2023, the study involved 30 volunteers (9 women, 21 men) with the mean age is 43.0±12.7 years, accompanied by a mean body mass index of 24.0±3.1 kg/m.² They all tolerated the preoperative preparation well and successfully swallowed the capsule endoscope, with one subject requiring assistance from the magnetic handle. Two subjects experienced nausea during the first attempt at swallowing the capsule endoscope but were able to successfully swallow it after the lidocaine aerosol was sprayed on the posterior pharyngeal wall.
Examination process
Cable transmission magnetically controlled capsule endoscopes (CT-MCCEs) successfully enter the esophagus, and with the help of a traction wire, they provide a comprehensive view of the esophagus before it gradually advances into the cardia. The superior curvature of the proximal gastric corpus, representing the most inferior aspect of the stomach in a recumbent orientation, was first documented. In 83.3% of the subjects, the gastric mucosa, which was initially covered with minimal mucus and foam, was clearly observable by adjusting the angle of the capsule endoscope. The capsule endoscopy revealed a completely unobstructed field of vision in 16.7% of the participants. The subjects were positioned in the supine posture, while the magnet handle facilitated the navigation of the capsule towards the pylorus and into the duodenal bulb. Upon the retraction of the tow rope, the capsule endoscope was withdrawn into the stomach, allowing for the observation of the pylorus, cardia, gastric fundus, gastric sinus, gastric body, and the sinus section. When the surface of the capsule endoscope is covered with mucus, it can be removed by friction with the gastric mucosa using a magnetic handle or by pulling the capsule into the esophagus and using peristalsis of the cardia to remove the mucus.
The average examination time of the capsule endoscope was 29.5±6.63 min (18.9~43.9 min). To account for the impact of gastric emptying on gastric filling, all examinations were conducted within 45 min, with an average of 24.5±7.0 min in the stomach (range:14.6--40.6 min). The cleanliness within the gastric cavity was assessed as good in 25 (83.3%) individuals and categorized as moderate in 5 (11.8%) individuals. Excessive mucus was the main cause of opaque visualization.
Feasibility
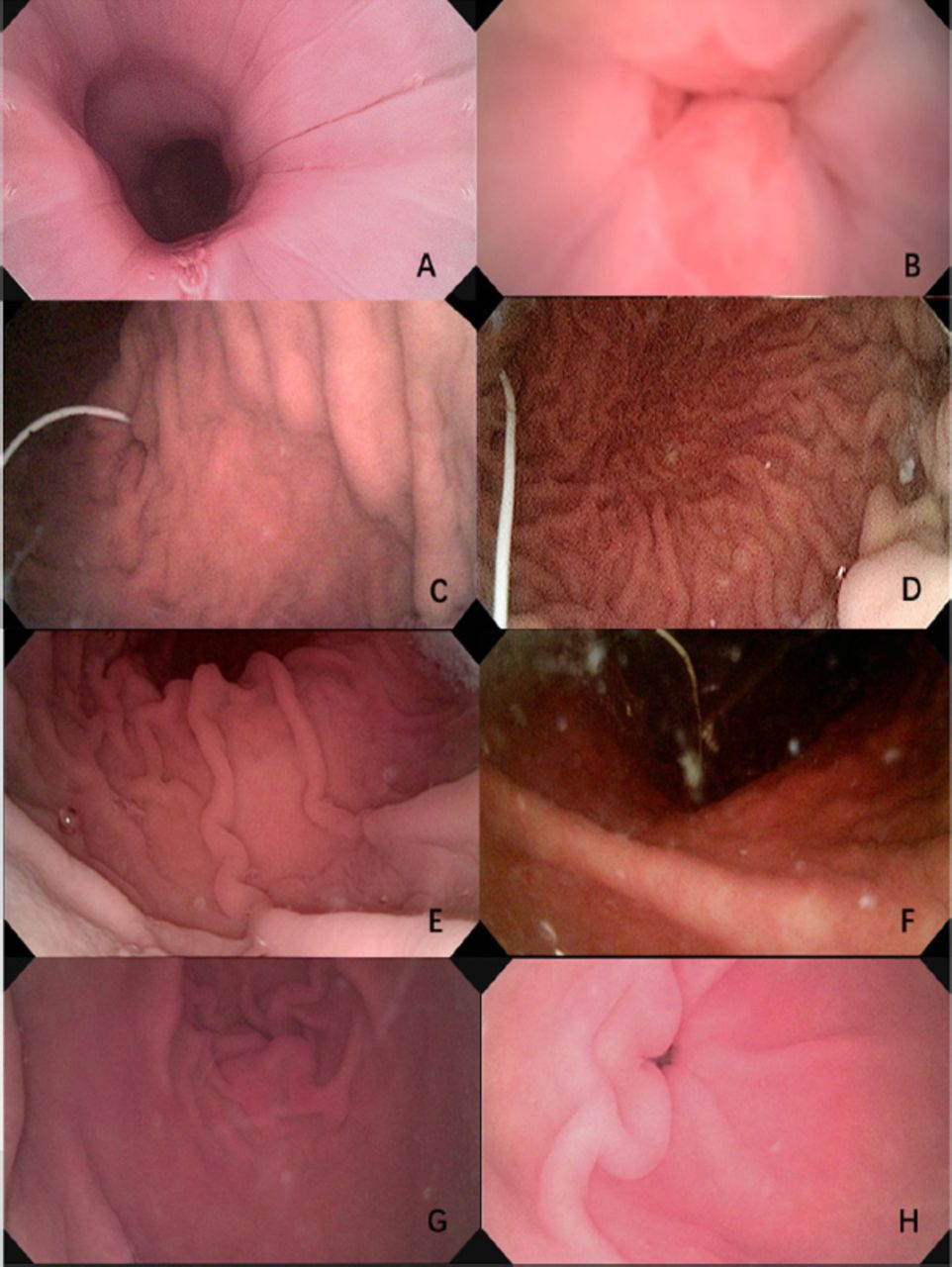
In all 30 subjects, the CT-MCCE capsule followed the guiding magnetic robot and reached the primary landmarks, including the esophagus, cardia, fundus region, dentate line, body of the stomach, antrum, gastric angle and pylorus; thus, maneuverability was categorized as good (Figure 2). The CT-MCCE capsule entered the duodenal bulb through the pylorus successfully in all 30 subjects, with an average time from swallowing to entering the duodenal bulb of 10.1±5.0 min (1.93~20.2 min). In 6 subjects, the capsule took longer than 15 min to pass through the pylorus because of relaxation of the pyloric sphincter and the anatomical position of the gastric cavity.

- The images of primary landmarks in esophagus and stomach. A) esophagus, B) dentate line, C) cardia, D) fundus, E) body of stomach, F) angulus, G) antrum, H) pylorus
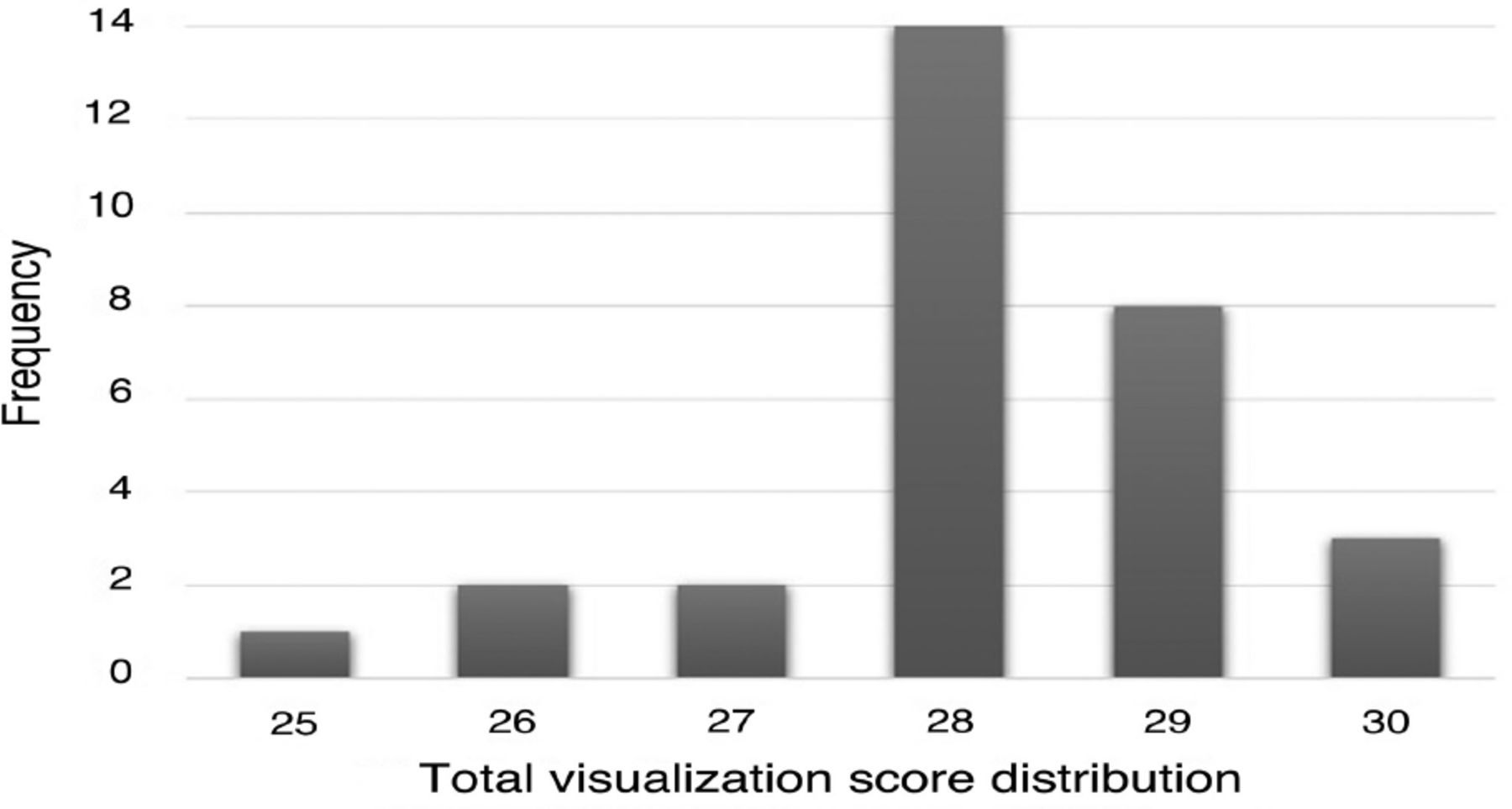
Table 1 shows the visualization score of each anatomical landmark. Mucosal visualization was rated as good (total score ≥27) in 90% of the subjects (27 individuals) and moderate (20≤ total score <27) in 10% of the subjects (3 individuals). Two subjects (subjects 1 and 18) were Helicobacter pylori positive with significant opaque fluid, and one subject (n=25) experienced significant bile reflux after 35 min of examination (Figure 3). The structural landmarks of the esophagus, stomach, and duodenal bulb were clearly delineated in the majority of patients.
- Visualization score for each anatomical landmarks in 30 volunteers.

- The total visualization score distribution of 30 volunteers.
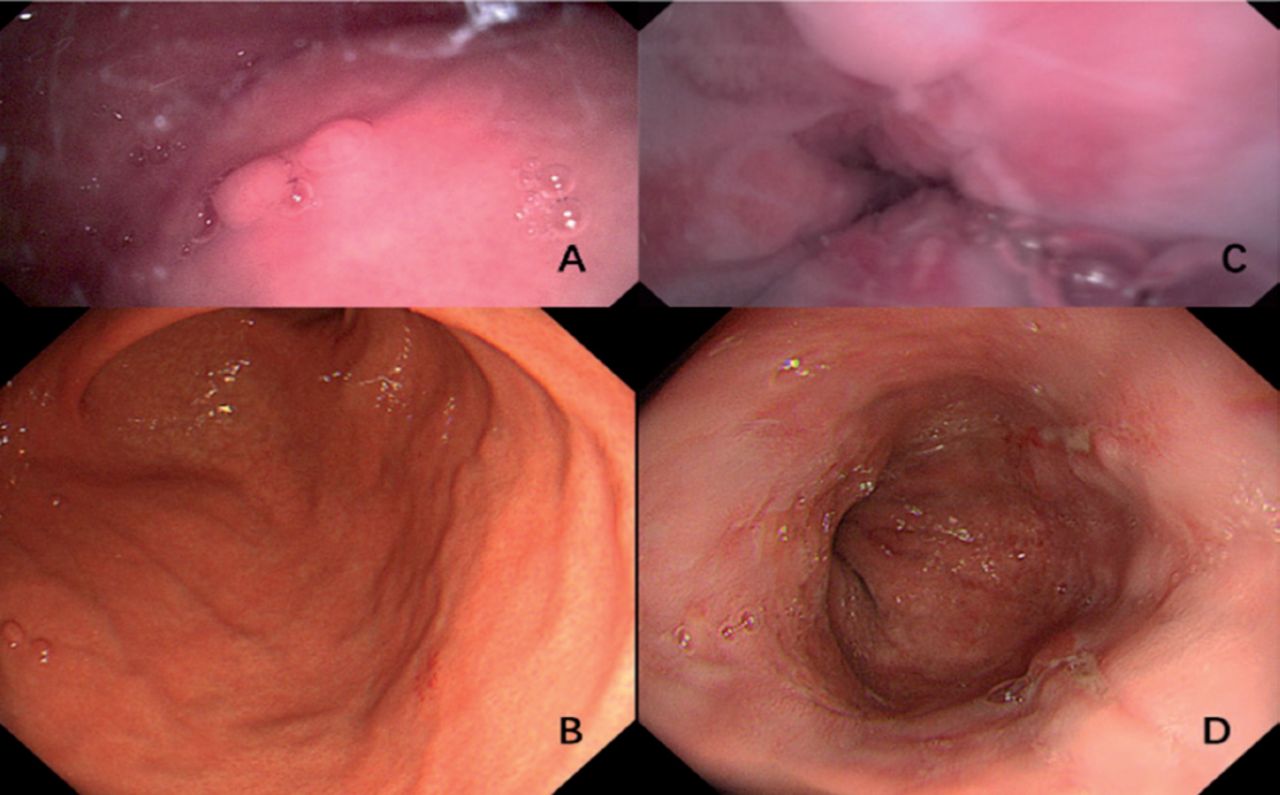
Pathologic results revealed polyps in 4 subjects (13.3%), erosive lesions in 4 (13.3%) subjects, and reflux esophagitis in 3 (10%) subjects. After 3 hours, the lesions were evaluated and confirmed by gastroscopy (Figure 4).

- Gastric polyps and reflux esophagitis were found during Cable transmission Magnetically Controlled Capsule Endoscope examination. A) The image of gastric polypsby capsule endoscope. B) gastric polyps confirmed by the following gastroscopy. C) The image ofreflux esophagitisby capsule endoscope. D) reflux esophagitis confirmed by the following gastroscopy.
Safety
The gastric preparation protocols and the CT-MCCE assessments were both proficiently endured and considered satisfactory. All 30 (100%) subjects rated the gastric preparation as good and the gastric CT-MCCE as very good. None of the 30 subjects experienced discomfort during the CT-MCCE examination or follow-up, whereas 10 (33.3%) subjects reported nausea, vomiting, or abdominal distention during the traditional endoscopic examination. All capsules were successfully retrieved from the stomach to the mouth without discomfort in all the subjects.
Discussion
Capsule endoscopy is widely recognized as a revolutionary innovation with notable advantages, such as its noninvasive nature and convenience. With the development of magnetically controlled capsule technology, traditional passive capsules can now be actively controlled by endoscopists. Research has shown that an external magnetic field can manipulate the capsule for relevant examinations within the stomach.9,11-12 Magnetically controlled capsule endoscopy has several advantages, such as high acceptance and tolerance, satisfactory image quality, similar diagnostic yields, convenience and no need for sedation.13,14 However, the esophagus has remained a challenging area to observe adequately with magnetic capsule endoscopy. In addition, the retention risk of traditional capsule endoscopy cannot be ignored.
This pilot study preliminarily evaluated the innovative cable transmission magnetically controlled capsule endoscope system in healthy volunteers.15 CT-MCCE represents as a potential advancement over other clinically available magnetic-controlled capsule endoscopes in the field of capsule endoscopy. This capability is attributed to the use of a flexible wire traction system, which enables clear visualization of the esophagus. Researchers can manipulate the position of the capsule endoscope and thereby observe various regions of the esophagus. In our study involving 30 volunteers, all the dentate lines were successfully visualized using CT-MCCE. This finding highlights the effectiveness of the device in providing comprehensive views of the esophageal structure. Notably, in one patient, the dentate lines initially obscured by mucus became visible after the patient’s body position changed. Additionally, the flexible wire enhances the mobility of the capsule within the gastric cavity. When the control of the capsule by the external magnetic handle is not satisfactory, the pushing and pulling of the flexible wire can provide an effective supplement.
In our study, the CT-MCCE system showed excellent maneuverability with good mucosal visualization. The capsule followed the guidance of the magnetic handle to any part of the stomach. Anatomical landmarks, including the dentate line and duodenal bulb, were reached in all 30 subjects, which is not a routine step in conventional magnetic capsule endoscopy. The average examination time of the capsule endoscope was 29.5±6.63 min, and all examinations were completed within 45 min. Mucosa visualization was rated as good in 90% of the subjects and moderate in 10%.
The cable transmission design of our system eliminates the need for a built-in power supply, which makes the capsule smaller and potentially easier to swallow. Table 2 shows the primary parameters of the CT-MCCE system and other MCCE systems that are clinically used. The CT-MCCE system is smaller and lighter in weight and offers high resolution. The study’s examination process proceeded smoothly without any adverse events. All capsules were successfully swallowed and subsequently removed during the examination process.
- Primary parameters of different MCCEs.
The gastric preparation and CT-MCCE examinations were both adequately tolerated and considered satisfactory. All 30 subjects rated the gastric preparation as good and the CT-MCCE capsule acceptance in the stomach as very good. None of the 30 subjects experienced discomfort during the CT-MCCE examination or follow-up, whereas 10 subjects (33.3%) reported nausea, vomiting, or abdominal distention during the traditional endoscopic examination. All capsules were successfully pulled from the stomach to the mouth without discomfort in all the subjects. The presence of the string did not increase the discomfort of swallowing, and the patient experienced no discomfort in the pharynx when the cable capsule moved into the stomach.
Study limitations
First, we enrolled a relatively small sample size in our study, which means that feasibility, safety, and diagnostic power need to be further validated. Furthermore, in spite of the previously mentioned benefits, the CT-MCCE system does not facilitate biopsy procedures or other therapeutic interventions.
In conclusion, the CT-MCCE system is feasible, safe, and well-tolerated for a comprehensive examination of the esophagus, duodenal bulb and stomach. Further research with larger samples in high-risk groups is necessary to assess the diagnostic accuracy of CT-MCCE.
Acknowledgment
We acknowledge American Journal Experts (www.aje.com) for their assistance with the English language editing.
Footnotes
Disclosure. This study was funded by the Ministry of Science and Technology Xiong’an New Area Science and Technology Innovation Special Project (No. 2022XAGG0146) and the Youth Clinical Research Project of Peking University First Hospital (No.2021CR06).Scientific Research Seed Fund of Peking University First Hospital (No. 2020SF28 and No. 2021SF41).
- Received August 24, 2024.
- Accepted November 1, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.