


Abstract
Objectives: To identify the clinical and histological features of MF that can assist in distinguishing MF from MF-mimicking cases. Although mycosis fungoides (MF) is the most common subtype of cutaneous T-cell lymphoma, clinicopathological correlations are required to establish an accurate diagnosis, which are currently lacking.
Methods: This retrospective observational study evaluated the clinical presentations, characteristics, and histological features of 56 patients with suspected MF who presented to our clinic between January 2018 and August 2022. Immunohistochemistry was performed, and the loss of CD5 and CD7 T-cells and T-cell receptor rearrangement was evaluated.
Results: Overall, 34 patients were diagnosed with MF, whereas 22 were not. Clinical erythroderma, poikiloderma, and nodular presentations were more commonly associated with a histological diagnosis of MF than macular presentations. Erythema and pruritus were significantly more common in MF cases than in MF-mimicking cases (p<0.05). Epidermotropism and parakeratosis were the key histological features for diagnosing MF. Additionally, Pautrier’s microabscesses correlated with the clinical presentation of plaques in MF. Loss of CD7 expression on the T-cell surface was observed even in early-stage MF cases.
Conclusion: Our proposed diagnostic features are statistically valid and, along with those previously reported, can aid in identifying and distinguishing MF cases from MF-mimicking cases.
Mycosis fungoides (MF) is an extra-nodal non-Hodgkin T-cell lymphoma originating in the skin’s epidermotropic T-cells, specifically the memory T-cells (CD45RO+), which express the T-cell receptor (TCR) CD3, cutaneous lymphocyte antigens, and CD4+ or CD8+ immunophenotypes.1 It is the most common subtype of cutaneous T-cell lymphoma, a heterogeneous group of lymphomas that, by definition, are located on the skin at diagnosis and clinically differ from systemic lymphomas.2,3
Mycosis fungoides presents at different stages with different lesions. These stages reflect disease progression, which is associated with poor outcomes and extracutaneous dissemination.4 The patch stage of MF presents with erythematous or brownish, scaly patches that may resemble eczematous lesions and predominantly appear on the unexposed areas of a patient’s body.5 As MF progresses to the plaque stage, it presents as plaques with evident infiltration, accompanied by well-defined raised edges, and may often resemble common skin disorders.6 In the tumor stage, which is the more advanced stage of MF, large-diameter erythematous nodules appear, resembling tumors seen in other cutaneous lymphomas, along with an increased lymph nodal or visceral dissemination risk.7
Occasionally, MF presents with only erythroderma, or bullous/vesicular, purpuric, poikiloderma, or hypopigmented lesions.8 Furthermore, MF’s histological features are highly variable between its different disease stages and may not be diagnostic for MF, especially in the early stages, because the infiltrates may be scant, lack definitive diagnostic markers, or mimic other inflammatory diseases.1,8-10 Therefore, additional diagnostic measures, such as immunohistochemistry (IHC) and T-cell rearrangemet (TCR) gene rearrangement, may be necessary to establish a definite diagnosis in cases where histological analysis is inconclusive.11,12 Consequently, physicians face a diagnostic challenge when dealing with MF cases; this contributes to a delay in diagnosis and appropriate disease management.13,14
Accordingly, several studies have proposed clinical and histological MF diagnostic features that could minimize the difficulties encountered in diagnosing MF.15,16 However, the diagnostic features differentiating MF lesions from their clinical mimickers are not commonly analyzed in the literature. Hence, we aimed to identify valid clinical and histological diagnostic features that could differentiate between true MF lesions and their mimickers.
Methods
This study included male and female patients with a clinical history and manifestations suggestive of MF was presented to our Dermatology clinic at King Fahd Univerisity, Al Khobar between January 2018 and August 2022. This study was approved by the Ethics Committee Imam Abdulrahman bin Faisal University. Written informed consent was obtained from all participants. Skin biopsies were performed in 56 patients. The following presentations were considered ‘suspicious clinical presentations’: i) scaly, erythematous, or hypo-/hyperpigmented macules, patches, or plaques (single or multiple) that remained fixed in the same area for >6 months and did not respond to topical steroids; ii) any lesions showing signs of poikiloderma;15 iii) erythematous nodules that presented for >6 months without obvious reasons for nodule development and with or without a previous history of MF or associated lymphadenopathy; iv) erythroderma that presented as widespread erythema involving >90% of the body surface area;16 v) follicular eruptions that presented as papular eruptions fixed for >6 months and did not respond to topical steroids in the absence of a recent drug ingestion history; and vi) any lymphadenopathy-related skin lesions. Patients with confirmed MF who were already followed-up were excluded from the analysis unless they presented with a new nodular lesion. The presence of other chronic illnesses or treatments was not considered.
After collecting the patient’s history and performing examinations, special clinical characteristics of the suspected lesions were assessed, including the presence of erythema, hypo- or hyperpigmentation, scales, association with itching, or lymphadenopathy. A provisional diagnosis was established, and a punch biopsy of the most active skin lesions (selected based on color and texture) was performed. Formalin-fixed, paraffin-embedded, archived blocks of biopsy specimens were used to prepare consecutive sections for histological, hematoxylin and eosin (H&E), and IHC staining.
Tissue analysis. Hematoxylin and eosin staining
Hematoxylin and eosin staining was performed as previously described to assess the possibility of an MF diagnosis based on the presence or absence of 10 different histological features:17 epidermotropism, which was defined as the presence of lymphocytes within the epidermis with a basilar or lentiginous pattern (this definition was used to distinguish epidermotropism from exocytosis, which commonly shows a pagetoid pattern of lymphocyte infiltration in the epidermis);18 atypical lymphocytes, which were described as slightly enlarged, hyperchromatic, and hyperconvoluted lymphocytes that are found within epidermis;19 Pautrier’s microabscesses, which were defined as ‘punch-out’ spaces in the epidermis filled with cerebriform T-lymphocytes, and these spaces were not surrounded by focal spongiosis or spongiotic vesicles;20 and cerebriform lymphocytes, defined as lymphocytes with characteristic convoluted to cerebriform nucleus with mildly condensed chromatin and inconspicuous nucleoli, spongiosis, parakeratosis, pigment incontinence, presence of dermal infiltrates, dermal fibrosis, and adnexal involvement by cellular infiltrates (Table 1).21
- Grading of histological parameters for the assessment of suspected mycosis fungoides.
Some of these features were graded from 0–3, depending on the number of these elements per high-power field or 100 cells (as in epidermotropism, cribriform lymphocytes, and atypical lymphocytes), percentage of these elements (as in parakeratosis), degree of these elements (as in spongiosis), or site of these elements (as in dermal infiltrates). Subsequently, these traits were analyzed on each slide. Slides with atypical lymphocytes, epidermotropism, Pautrier’s microabscesses, or dense dermal infiltrate with large cerebriform lymphocytes were labeled “MF”.7 Slides with histological findings of nonspecific dermatitis and perivascular dermatitis, and without the histological features of MF or other cutaneous diseases, were labeled “inconclusive MF.”
Immunohistochemistry staining
The IHC staining with anti-CD3, CD4, CD8, CD5, and CD7 antibodies was conducted on consecutive slides for confirmed MF cases using the ultraView Universal DAB Detection Kit protocol to assess the presence of CD3, CD4, and CD8 T-cells, CD4-to-CD8 ratio, and loss of CD5 and CD7.22 CD5 and CD7 are the 2 T-cell antigens usually lost in malignant T-cells in MF;18 they must be expressed by <50% of the infiltrating T-cells and <10% of infiltrating lymphocytes, respectively, to be considered lost.5,11 T-cell receptor rearrangement was evaluated using polymerase chain reaction or immunoblotting, and the patient’s skin sample was used for the TCR-γ assay. The test’s availability at diagnosis determined the number of cases examined using the test.
Statistical analysis
All contingency table analyses and ordinal logistic regressions were performed using JMP software (version 13.2; SAS Institute Inc., Cary, NC, USA). Permutation tests were performed using Genstat (version 18.2; VSN International Ltd., Hemel Hempstead, UK). Goodness-of-fit tests were conducted online using a simple Chi-square calculator. Unless otherwise noted, statistical significance was set a priori to alpha=0.05.
To examine clinical characteristics of MF lesions compared with those of their mimicker lesions, analysis of all MF count data were pooled irrespective of the clinical features, similar to that in the control group of non-MF patients. This was carried out to compare the presence/absence frequencies (proportions) of 6 lesion characteristics (see A and B) between MF and non-MF groups by applying a Fisher’s exact test to their corresponding 2x2 contingency tables. The resulting p-values were significant for erythema and itching. The resulting p-values were below 0.05 but above 0.01 for two characteristics, scales and lymphadenopathy, and the latter contained 0 counts in one cell; hence, follow-permutations tests were run (Bonferroni-correction) (n=4999) to the set of 6 tests above, to err on the side of caution, and the threshold for significance would be stricter, at 0.05/6 tests=0.0083. This made scales and lymphadenopathy not significantly different and therefore not relevant to the clinical diagnosis of MF, leaving erythema and itching as the key differing features.
Regarding histological features of MF lesions analyzed in the study, results of a detailed statistical analysis are presented in Appendix 1.
Results
Clinical presentations characterizing MF lesions
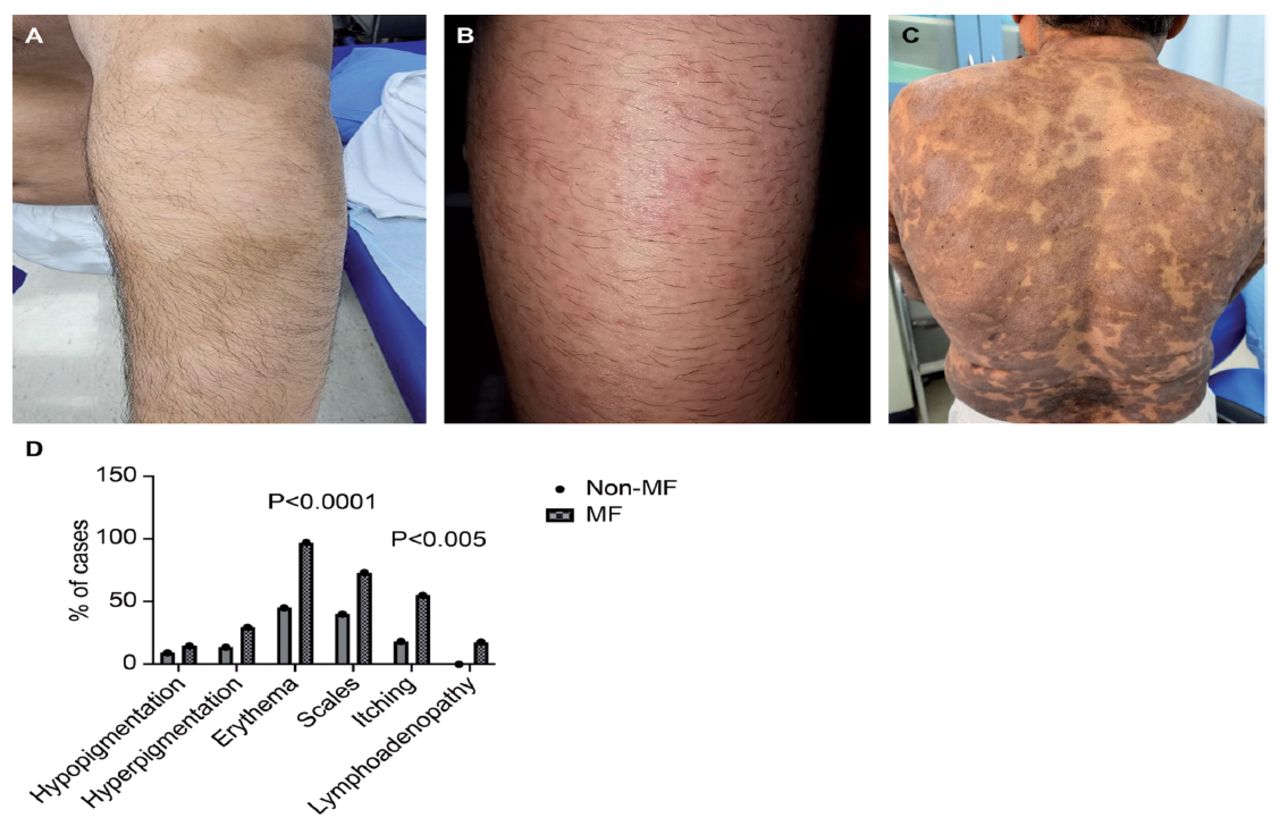
Table 2 presents the profiles, clinical presentations, and clinical characteristics of the 56 patients who were presented with lesions suspicious of MF. Regarding clinical presentations, 20 patients had patches, 22 had plaques, 4 had nodules, 2 had erythroderma, 2 had poikiloderma, 2 had follicular eruptions, and 4 had macules (Figure 1A). Mycosis fungoides diagnosis was confirmed in 60% (34 cases) of the 56 patients: 55% (11 cases) of the 20 patch presentations, 63% (14 cases) of the 22 plaque presentations, 100% of the 4 nodular, 2 erythroderma, and 2 poikiloderma presentations, 50% (1 case) of the 2 follicular presentations, and 0% of the 4 macular presentations (Figures 1B, 1C, & Table 2).
- Profile of 56 patients included in the study.

- Clinical presentations and characteristics of lesions suspicious of MF. (A) Patches present for > 6 months in the upper arm and trunk that were associated with hypopigmentation; the lesions were suspicious of MF. (B) Multiple erythematous papules, accompanied by intense pruritus of the upper arms and H&E-confirmed MF diagnosis. (C) Multiple hyperpigmented scaly patches involving the trunk and H&E-confirmed MF diagnosis. (D) Clinical characteristics of lesions suspicious of MF and their presence in MF cases (n=34) and non-MF cases (n=22). The graph shows that erythema and itching were significantly more common in MF cases than in non-MF cases. H&E: hematoxylin and eosin staining, MF: mycosis fungoides
This finding suggested a high correlation between MF diagnosis and the clinical presentation of nodular, erythrodermic, and poikilodermic lesions. Contrarily, the clinical presentation of macules was not associated with an MF diagnosis.
Patients who did not have an MF diagnosis histologically (n=22) comprised 45% of the 20 patch presentations, 37% of the 22 plaque presentations, 50% of the 2 follicular presentations, and 100% of the 4 macular presentations. This finding showed that the clinical presentations of patches (45%), plaques (37%), and macules (100%) were associated with a high rate of MF rejection.
The MF rejected cases were diagnosed as inconclusive MF or other diseases (n=7, 31% of rejected cases), discoid eczema (n=2, 9% of rejected cases), lichen planus (n=2, 9% of rejected cases), psoriasis (n=4, 18% of rejected cases), stasis dermatitis (n=1, 3.5% of rejected cases), post-inflammatory hyperpigmentation (n=1, 3.5% of rejected cases), tinea corporis (n=3, 13% of rejected cases), and pityriasis alba (n=2, 9% of rejected cases). The average age of patients who presented with malignant lesions was 53 years, and the majority were male (Table 2).
Regarding the clinical characteristics of MF lesions compared to their mimicker lesions, erythema and itching were significantly associated with MF lesions (p<0.5) (Figure 1D).
Histological features analysis of MF and MF mimickers and clinico-histological correlation with MF
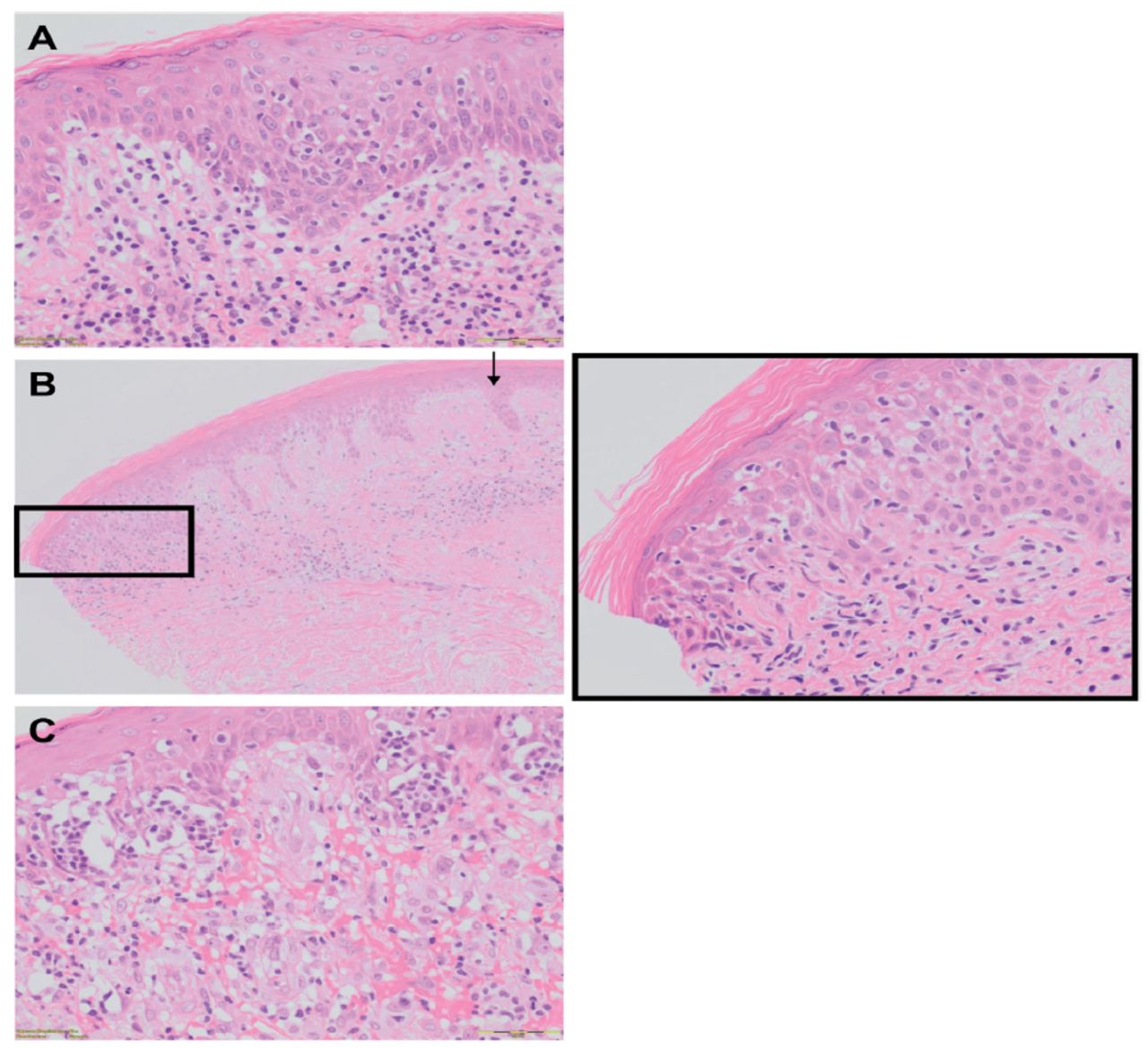
Histological analysis of the skin lesions (Appendix 1) indicated that 6 features were significantly more frequently detected in MF lesions than in MF mimicker lesions, namely epidermotropism, Pautrier’s microabscesses, parakeratosis, dermal fibrosis, atypical lymphocytes, and cerebriform lymphocytes (Figure 2A). In contrast, pigment incontinence, presence of dermal infiltrates, adnexal involvement by infiltrates, and spongiosis did not differ significantly between MF and their mimickers.

- Histological features used in the study to distinguish mycosis fungoides (MF) from non-MF cases. A) Epidermotropism is significantly found in MF cases compared with non-MF cases. B) Spongiosis (Grade 1) is present in MF cases, where it is located at the epidermal sites invaded by atypical lymphocytes (black rectangle). Areas not invaded by atypical lymphocytes show no spongiosis (black arrow). C) Pautrier’s microabscesses are significantly found more in the plaque stage than in the patch stage of MF (original, ´200 all).
Interestingly, in MF cases, grade one focal spongiosis was present at the epidermal sites with atypical T lymphocyte infiltration, in contrast to the epidermal sites that did not contain atypical T lymphocyte infiltration where spongiosis was absent (Figure 2B).
Next, we only selected cases presenting with patches and plaques, because these had sufficient sample sizes to clarify which of the above 6 histological features are important in MF diagnosis. Accordingly, the patch and plaque groups were analyzed separately, and we found epidermotropism and parakeratosis as the key features in the histological diagnosis of MF (Appendix 1).
Additionally, the patch and plaque-specific clinical presentations of MF were compared with the presence of the 10 different histological features. This comparison revealed that, except for Pautrier’s microabscesses (p=0.0472, Figure 2C), these two clinical presentations (patches and plaques) showed no significant difference in histological features or grade severity and that the presence of Pautrier’s microabscesses could be correlated with plaque MF’s clinical presentation.
Immunohistochemistry analysis and TCR arrangement of MF cases
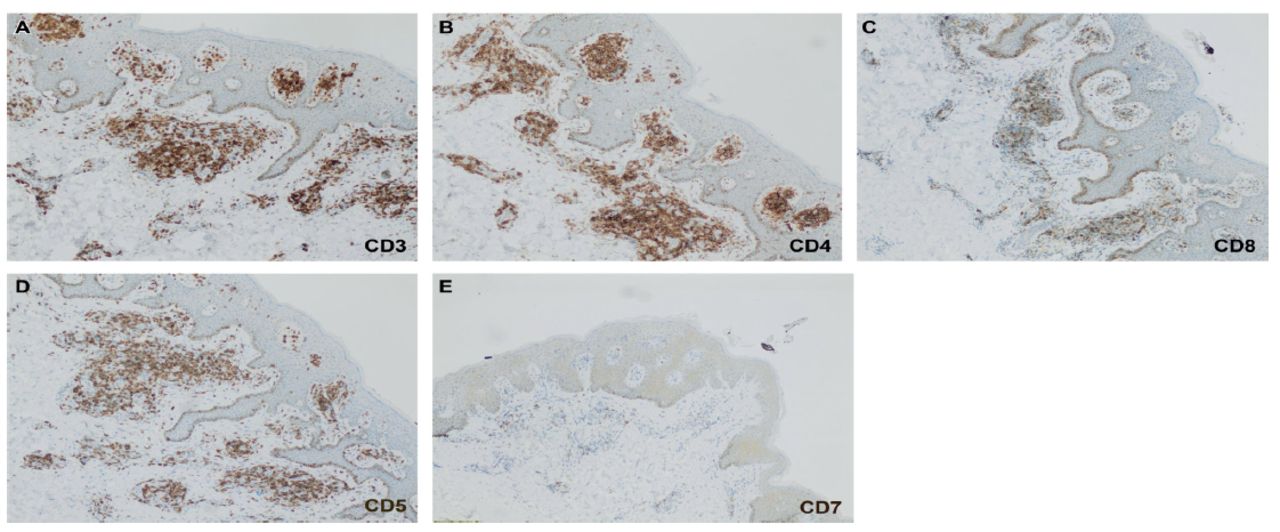
Immunohistochemistry staining performed on MF cases revealed that all cases were positive for CD3 and CD4 and that 2 cases were positive for CD8, with a CD4-to-CD8 ratio of 2.5:1. The clinical presentation and characteristics of these cases were hypopigmented patches (Figure 3A–C).

- Immunohistochemical staining of mycosis fungoides cases. A) Positive expression of pan T-cell markers (CD3). B) Positive expression of CD4. C) Positive expression of CD8 with a ratio of 2.5:1 epidermally. D) Positive expression of CD5. (E) Loss of CD7. (original, ´200 all)
CD5 expression was lost in 35% of cases (including 5 cases with patch or plaque presentations and the remaining 7 cases with erythroderma, nodular, and poikiloderma presentations) and preserved in 65% of cases (Figure 3D), whereas CD7 expression was lost in 100% cases (Figure 3E). Additionally, monoclonality was observed in all examined MF cases (n=13). Overall, according to the TCR clonal rearrangement testing, 2, 5, 2, 2, 1, and 1 patient showed a clinical presentation of patches, plaques, erythroderma, nodules, poikiloderma, and clinical lichenoid eruption, respectively.
Discussion
In this study, almost one-third of the biopsied cases did not histologically show MF features. This high proportion of cases is consistent with that reported by Kelati et al.23 Specifically, in a retrospective cohort of 370 patients with clinically suspected MF, Kelati et al23 found an up to 84% rejection rate based on the histological test results. This suggests that the broad clinical presentation spectrum of MF and inconclusive results that a physician may obtain from a single biopsy remain the major challenges for dermatologists when dealing with cases suspicious of MF.7,24
The finding of clinical presentations of macules, patches, and plaques as the types mimicked by other biopsy-confirmed inflammatory diseases, in contrast to erythroderma, nodules, and poikiloderma, indicates how lesions in early-stage MF can simulate others because of their similar clinical manifestation with other common cutaneous diseases, underscoring the need for reliable diagnostic criteria to distinguish MF from benign dermatosis. Accordingly, we identified erythema and pruritus as 2 significant clinical features that distinguish early-stage MF lesions from benign dermatosis, and our findings are consistent with the criteria described by Kelati et al23 and Vandergriff et al.25
Regarding the epidemiological results of MF in our study, the male predominance and average patient age were in line with the global figures.26,27 However, they were inconsistent with the results collected from local studies showing younger patients to be mostly diagnosed with MF and recent findings that showed a rapid increase in the incidence of MF among young patients globally.28-30 This could be explained by the lack of awareness among primary health physicians and patients regarding the possibility of MF, which leads to a delay in seeking dermatological consultation and, consequently, older age at the time of diagnosis.
Based on the histological features found to differentiate MF from their mimickers in our study, all the features aligned with those previously reported as significant parameters to differentiate MF from non-MF.15,16 The 2 features, parakeratosis and epidermotropism, which specifically differentiate patch and plaque MF from non-MF cases, are consistent with the findings of a research that considered epidermotropism to be the hallmark of MF.31
Regarding the remaining histological features that did not differ between MF and their mimickers, spongiosis was found in MF mimickers and MF lesions—a finding that is unusual in MF histology—and its absence was used to favor the diagnosis of MF.32,33 Shamim et al32 identified epidermotropism with spongiosis to be a central histopathological feature in nine MF cases, and Shapiro et al34 reported that 7% of histology slides in a cohort of 222 patients with MF had spongiosis, highlighting the importance of the spongiotic histological presentation of MF despite its rarity. However, the MF-associated spongiosis in our cases was always found at epidermal sites exhibiting atypical lymphocyte infiltration, compared with the epidermal sites that did not show this type of infiltration; this is a finding that could be explained by the disproportionate epidermotropism. This feature suggests the presence of spongiosis with epidermotropism in MF slides but with less spongiosis in relation to the degree of malignant lymphocyte infiltration.16 Consequently, spongiosis in MF histology is infrequent, and its association with epidermotropism remains a characteristic finding in MF.
In contrast, the clinicopathological correlation of MF showed that the plaque presentation was more significantly associated with Pautrier’s microabscesses than with patch presentations. Our study is consistent with a previous study that described this clustering of atypical lymphocytes in the epidermis as a part of the disease progression from patch skin presentation to the development of thicker plaques.8
Finally, our IHC and TCR gene clonal rearrangement results were consistent with previous findings regarding the rarity of CD8+ T-cells in the epidermis of MF skin and their presentation, preferably in cases of hypopigmented MF, positive CD3 and CD4 in all MF slides, and monoclonal T-cells in the skin tissue with MF.35-37 Regarding the loss of CD5 and CD7 expressions, our findings align with previous findings that showed a greater reduction in CD7 expression in early-stage MF than CD5 expression, confirming the idea that loss of CD7 expression is a finding specific to MF, even in the early disease stages, especially since studies showed that the reduction in CD7 expression in MF reached 80%, compared to CD5 expression loss that did not exceed 10%.3,11,31,38,39
Study limitation
Nonetheless, this study had some limitations, including the small sample size, lack of correlation between the histological features and the stage of each MF lesion, and the absence of IHC and TCR clonal rearrangement results for the MF mimickers.
In conclusion, our study findings indicate that MF diagnosis still poses a challenge among doctors because of MF’s variable clinical picture and its similarity with other common cutaneous diseases. However, our proposed statistically valid clinical and histological diagnostic features, along with those already mentioned in the literature, could assist in diagnosing MF cases and distinguishing them from their mimickers.
Acknowledgment
This research work (Grant Number 2019380) was supported by Deanship of Scientific Research, Imam Abdulrahman bin Faisal University, Dammam, Kingdom of Saudi Arabia. The authors acknowledge Editage (www.editage.com) for the English language editing.
Appendix
- Histological feature analysis of the 56 suspected mycosis fungoides (MF) lesions involved in the study.
Footnotes
Disclosure. This study was supported by Deanship of Scientific Research, Imam Abdulrahman bin Faisal University, Dammam, Kingdom of Saudi Arabia. Grant Number: 2019380
- Received September 11, 2024.
- Accepted October 22, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.