


Abstract
Objectives: To evaluate the sexual function of women with urinary incontinence (UI) and double incontinence (DI) comparing with a healthy control group by using the Female Sexual Function Index (FSFI).
Methods: This study was designed as a retrospective study consisting of UI, DI, and a control group, each containing age-matched 40 patients. Statistical comparisons were made among the UI, DI, and control groups in terms of the FSFI total score as well as each domain’s score.
Results: The FSFI total scores were found to be 22.92, 20.53, and 20.32 for the control, UI, and DI groups, respectively, and no statistically significant difference was found among the groups. A statistically significant difference existed among the groups only in terms of satisfaction and pain. Significantly higher pain was found in the UI and DI groups compared with the control group (p=0.007 and p<0.001). Although there was significantly lower satisfaction in the DI group compared with the control group (p=0.012), no significant difference was found between the UI and control groups.
Conclusion: The pain in the UI group and the pain and the low satisfaction in the DI group might be parameters that cause sexual dysfunction.
Urinary incontinence (UI) and fecal incontinence (FI) are important clinical conditions that impair women’s sex lives and thus negatively affect their quality of life. Approximately 25–45% of women will experience UI and 2.2–16.8% will experience FI during their lifetimes.1,2 Sometimes, both UI and FI occur simultaneously, which is known as double incontinence (DI) and affects approximately 6.3% of the female population.3 Urinary incontinence and FI can be encountered in different clinical presentations. Urinary incontinence in women can present as one of 3 types: urgency, stress, or mixed UI. Fecal incontinence can present as isolated flatal, liquid, or solid incontinence. When UI and FI occur together, many different combinations of these clinical presentations can be observed.
The Female Sexual Function Index (FSFI), a 19-question multidimensional self-report instrument, was developed to measure female sexual function (FSF). Measurements are made over 6 different domains, namely desire, arousal, satisfaction, lubrication, orgasm, and sexual pain. The FSFI has been validated in many languages and is used as the gold standard method for evaluating FSF.
Female sexual dysfunction (FSD) is a multidimensional health problem with sociological, psychological, and biological components. Its exact prevalence is not known, but it is thought to be quite common in the general population. Approximately one out of every 2 sexually active women has sexual complaints.4 Furthermore, UI and FI can negatively affect women’s sexual activity and well-being even if they do not occur during sexual activity. Incontinence-related impaired body self-image, self-confidence, and sensuality can influence sexual function.5 Although the prevalence of sexual dysfunction in sexually active women with UI differs according to the scales used and incontinence subtypes, it has been reported to be in the range of 23–56%.6 In women with FI, data on prevalence are insufficient due to the scarcity of studies on sexual dysfunction.
Moreover, several studies have evaluated sexual function in women with UI or FI; however, no studies have compared UI and DI patients in terms of FSF. Therefore, we aimed to evaluate the sexual function of women with UI and DI comparing with a healthy control group by using the FSFI.
Methods
This study was designed as a retrospective study including 120 sexually active women and conducted between 2020 and 2022 in the Urology Department, Gazi University School of Medicine, Ankara, Turkey. Patients with pure stress or stress-predominant mixed incontinence were included in the UI group. Patients who applied to our clinic with a UI diagnosis and were found through anamnesis to leak gas or stool (solid or liquid) were included in the DI group. After matching by age at a 1:1 ratio, the case sample randomly included 40 patients with UI and 40 patients with DI. Furthermore, an age-matched control group included 40 sexually active volunteer women working as healthcare professionals in our center without any genitourinary complaints or known diseases. The inclusion criteria for the selected participants were as follows: aged 18–60 years, sexually active, able to complete the questionnaires, and willing to participate in the study. The exclusion criteria were pregnancy, neurologic dysfunction, pelvic organ prolapse greater than stage II, acute urinary tract infection, acute diarrhea, and cognitive dysfunction. All participants were asked to complete the self-report FSFI questionnaire and were informed on their anonymity and confidentiality. The minumum sample size was determined by power analysis.
Clinical data, including age, menopause status, type of UI, and type of FI were retrieved from the female urology database of Gazi University School of Medicine, Urology Department University Female Urology Department database retrospectively. The presence of both UI and FI was defined as DI. Urinary incontinence was assessed through anamnesis, the International Consultation on Incontinence Questionnaire-Urinary Incontinence-Short Form (ICIQ-UI-SF), and the cough stress test. Fecal incontinence was assessed through anamnesis and the Fecal Incontinence and Constipation Questionnaire (FICQ). The FSFI was used as a reference gold standard measurement tool for evaluating FSF. For the definition of FSD in the FSFI, values <26.55 were used.
All participants signed an informed consent form. Ethic approval was obtained from the local ethics committee of our university.
Statistical analysis
All statistical analyses were performed with R version 4.0.4 through R Studio version 1.4.1106. Statistical comparisons were made among the UI, DI, and control groups in terms of the FSFI total score as well as for each domain’s score using the Kruskal–Wallis test. The Mann–Whitney U test was used for post-hoc analysis. A significance level of α=0.05 was set for the analysis.
Results
The median (interquartile range [IQR]) age of the women who participated in this study was 48 years (45-52), and no statistically significant difference existed among the UI, DI, and control groups (median [IQR] =49[46–52.5], 46.5 [43.7–51.2], and 47 [43.7–51.2], respectively, p=0.125). In the UI group, 22 of the 40 patients had pure stress incontinence and 18 had stress predominant mixed UI, whereas in the DI group these figures were 13 and 27, respectively. In the DI group, 14 of the 40 patients had stool (± gas) incontinence, while 26 of the 40 only had gas incontinence.
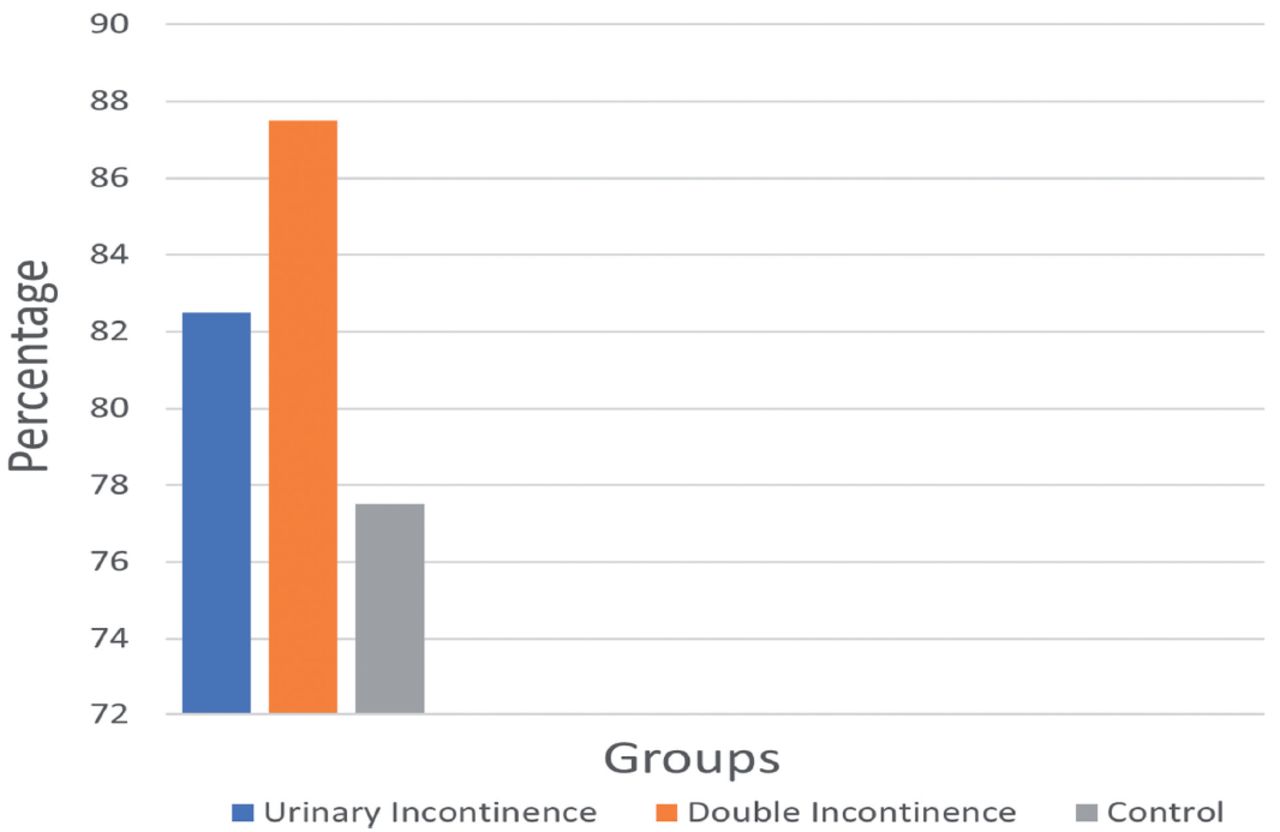
Table 1 presents a comparison of the total FSFI score as well as each domain’s scores among the control, UI, and DI groups. The FSFI total scores were found to be 22.92, 20.53, and 20.32 for the control, UI, and DI groups, respectively, and no statistically significant difference was found among the groups. When the cut-off value for FSD was taken as 26.55, we observed that the median values of all three groups were below this cut-off value, and the FSD was seen in 31 (77.5%), 33 (82.5%), and 35 (87.5%) individuals for the control, UI, and DI groups, respectively (Figure 1). Moreover, a statistically significant difference existed among the groups only in terms of satisfaction and pain. In the post-hoc analysis, significantly higher pain was found in the UI and DI groups compared with the control group (p=0.007 and p<0.001). Although there was significantly lower satisfaction in the DI group compared with the control group (p=0.012), no significant difference was found between the UI and control groups. In terms of these 2 parameters, no statistically significant difference existed between UI and DI groups.
- Comparison of the total Female Sexual Function Index score and the each domain scores among the groups.

- Sexual dysfunction rates in urinary incontinence, double incontinence and control group
Discussion
In the literature, there are many cross-sectional and case-control studies on the effects of UI on FSF.5 In these studies, various scales have been used to evaluate FSF, such as the PISQ-12, FSFI, and FSDS.6 Although different parameters have been used to detect and express sexual dysfunction in women with UI, the inevitable result of systematic reviews that have included these studies is quite clear. That is, UI negatively affects FSF either directly during intercourse or indirectly through the avoidance of intercourse.5,6 Another result is that the most negatively affected group in terms of sexual function is women with mixed UI.5,6 This is because different forms of incontinence may occur at different stages of sexual intercourse in mixed UI. In one study, incontinence during penetration was associated with stress UI, whereas incontinence at orgasm was associated more often with detrusor overactivity.6
We believe that the high FSD rates in both groups were also due to the absence of isolated urge incontinence cases. In addition, it was not questioned whether there was fecal incontinence during intercourse. If this were known, it would be easier to explain these results. The results may also have been worse, as having DI indicates that pelvic floor functions are severely affected. The extent of pelvic damage can affect FSF.
Furthermore, since there was a healthy control group in our study, we used the FSFI instead of disease-related scales to evaluate FSF. In our analysis, we found lower FSFI scores in the UI and DI groups compared with the control group, which was expected; however, the differences were statistically nonsignificant. We also found that the pain score was significantly higher in the UI group compared with the control group. In support of this finding, studies have reported a higher FSFI pain score or more dyspareunia, while other studies have indicated that the pain score did not change significantly.7-9 In general, decreased desire, arousal, lubrication, and satisfaction are observed in stress and mixed UI.6
Moreover, we found more pain and less satisfaction in women with DI compared with the control group. However, no differences existed for the UI group. Compared with UI, sexual dysfunction in women with FI and DI has been the subject of less research, and data are currently lacking, insufficient, and controversial. Studies of patients undergoing sphincteroplasty were early investigations in this area. In 2006, Trowbridge et al10 reported that FI scores and FSD scores after anal sphincteroplasty were not correlated, whereas Pauls et al11 reported that FI after sphincteroplasty was associated with poor sexual function. In 2012, Imhoff et al12 conducted a study on 2269 women using the FSFI and found that FI was associated with pain, decreased lubrication, and difficulty achieving orgasm. However, the authors reported that these symptoms did not lead to the avoidance of sexual intercourse. It has also been reported that women with isolated gas incontinence have similar sexual function to women without incontinence. We found no significant differences in FSFI scores between the UI and DI groups in our study, which may be due to the patients with only gas incontinence included in the DI group. In 2017, Li-Yun-Fong et al13 evaluated the effect of pelvic floor dysfunction on sexual functions and found pelvic organ prolapse, FI, and obstructed defecation to be associated with women not enjoying sex. In support of this, we found significantly higher pain and lower satisfaction rates in our DI group.
Study limitations
This study was a retrospective study. The number of patients was low because we do not encounter many patients with DI complaints in daily practice. We selected the control group from healthy female healthcare professionals at our center, but we encountered a high FSD rate. The control group could have instead been selected from individuals other than healthcare professionals. The control group may have been the biased control group. Since coital incontinence due to detrusor overactivity is also observed during orgasm, women with isolated urge incontinence could also have been included in this study.
In conclusion, we determined that pain in the UI group and pain and low satisfaction in the DI group might be parameters that cause sexual dysfunction. We did not detect any significant difference between the UI and DI groups in any of the parameters. High-volume prospective studies with a well-selected control group are required to obtain clearer results.
Acknowledgment
The authors would like to thank Scribbr for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 8, 2023.
- Accepted December 5, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.