


Abstract
Objectives: To assess the impact of sarcopenia and vitamin D levels on the severity of lower urinary tract symptoms (LUTS).
Methods: A total of 193 male patients, aged 60 years and above, who visited the geriatric outpatient clinic at Ibn-i Sina Hospital in Ankara, Turkey, between December 2019 and March 2021, were enrolled. Sarcopenia was diagnosed according to the criteria set by the European Working Group on Sarcopenia in Older People. The presence and severity of lower urinary tract symptoms were assessed using the International Prostate Symptom Score questionnaire, categorizing symptom severity as mild or moderate-to-severe.
Results: The median patient age was 71 years (range: 66-77). Sarcopenia affected 24.9% of the population studied. Mild LUTS was observed in 43.5% and moderate-to-severe LUTS was observed in 56.5% of patients. Sarcopenia prevalence was significantly higher in the individuals with moderate-to-severe LUTS compared to those with mild-LUTS (p=0.021). After adjusting for Charlson comorbidity index and age, only vitamin D levels were significantly associated with increased odds of moderate-to-severe LUTS (odds ratio [OR]=0.95, 95% confidence interval [CI]: [0.92-0.98], p=0.002). Sarcopenia was not significantly associated with the severity of LUTS (OR=2.04, 95% CI: [0.94-4.45], p=0.070). An inverse linear trend was observed between quartiles of 25 (OH) vitamin D and LUTS severity. As 25 (OH)vitamin D levels increased, the proportion of patients with moderate-to-severe LUTS decreased (p=0.023).
Conclusion: Sarcopenia did not significantly impact LUTS severity, but low vitamin D levels were associated with moderate-to-severe LUTS.
As individuals age, the likelihood of having lower urinary tract symptoms (LUTS) significantly increases, leading to a notable rise in prevalence. It was found that 44.7% of men worldwide were affected by LUTS, and in various studies, the prevalence was reported to be as high as 70% in those aged 80 years and above.1 Lower urinary tract symptoms can result from structural or functional abnormalities in the lower urinary tract, as well as from abnormalities in the peripheral or central nervous systems. Although benign prostate hyperplasia (BPH) related bladder outflow obstruction is the most common cause of LUTS in elderly men, various neurological diseases, as well as neuromuscular issues such as detrusor muscle weakness or overactivity, prostate or other urinary tract infections, and prostate cancer, may also significantly contribute to the development of LUTS.2 Lower urinary tract symptoms are classified as categories: storage, voiding, and post-micturition symptoms. Feeling of urgency, frequent urination during the day, nocturia, urinary incontinence, and unusual sensations in the bladder are related to urine storage. Voiding symptoms include a weak urine stream, stopping and starting during urination, difficulty initiating urination, straining to urinate, dribbling at the end of urination, and dysuria. Post-micturition symptoms involve a sense of incomplete emptying of the bladder after urination and dribbling of urine after urination.2 Despite not being a life-threatening condition, LUTS can markedly influence quality of life, leading to increased use of medication, higher risk of falls, social isolation, anxiety, and depression, particularly among elderly men.1,3
Vitamin D acts via vitamin D receptors (VDR) throughout the body and exerts important beneficial effects beyond the skeleton, including on muscle health.4 Vitamin D binds to the VDR on muscle fibers, promoting muscle hypertrophy and thereby enhancing muscle strength and physical performance.5 This relationship between vitamin D levels and the loss of muscle mass and decline in muscle strength with aging, is independent and increases the risk of developing sarcopenia, particularly in older individuals.6 Sarcopenia, defined by gradual reduction in skeletal muscle mass, strength, and function, poses a heightened risk for falls, fractures, limitations in mobility, and mortality in older adults.7,8
In vivo investigations have revealed the presence of VDR within the urothelium and smooth muscle layers of the bladder wall, prompting extensive investigation into the possible connection between vitamin D levels and LUTS.9 Nonetheless, it is crucial to acknowledge that current research on this subject remains limited and inconclusive. Sarcopenia and LUTS are multifactorial conditions with complex pathogenesis, sharing potential etiological factors such as age-related changes, hormonal imbalances, inflammation, and neuromuscular alterations. Given these common factors and existing knowledge gaps, our research intends to explore the impact of sarcopenia and vitamin D levels on the severity of LUTS in older males.
Methods
The data analyzed in this cross-sectional study were collected as part of a previously reported research project, assessing patients who attended the geriatric outpatient clinic at Ibn-i Sina Hospital, Ankara, Turkey, from December 2019 to March 2021.10 Therefore, the methods are identical to those published in the previous publication. The inclusion criteria encompassed men aged 60 years or above who could engage in verbal communication, possessed the cognitive capacity to comprehend and respond to questionnaires, and were capable of walking unaided. Those patients meeting these criteria were enrolled in the study. We excluded individuals who met any of the following conditions: I) patients with a diagnosis of physical impairments (namely, limb amputation, hearing loss, speech difficulties, post-stroke conditions, or bedridden status), malignancies, chronic kidney disease necessitating hemodialysis, major psychiatric illnesses, and advanced dementia; II) patients currently undergoing corticosteroid treatment, androgen synthesis inhibition, or receiving testosterone replacement; III) individuals who had undergone transurethral resection of the prostate or had a previous history of pelvic surgery; IV) patients with medical conditions that may hinder the accuracy of bioelectrical impedance analysis (BIA) for assessing skeletal muscle mass. These conditions include the existence of implants such as prostheses, mechanical heart valves, pacemakers, substantial edema in the extremities or sacral region, or significant disruptions in electrolyte balance.
The ethics committee at Ankara University granted approval for this study (approval number: İ6-280-19), and all participants willingly gave written informed consent in accordance with the guidelines established in the Declaration of Helsinki.
We gathered comprehensive medical histories from all patients, which included information regarding their tobacco use, alcohol consumption, and substance use, prior surgical interventions, underlying health conditions, and both prescribed and over-the-counter (OTC) medications. Patients were categorized as having BPH based on whether they were currently receiving any BPH treatment (alpha blockers), as indicated by their medication list. Each patient’s Charlson comorbidity index (CCI) was determined and recorded.11
A comprehensive geriatric assessment was carried out for all patients. Katz activities of daily living (ADL) scale and the Lawton instrumental activities of daily living (IADL) scale were utilized to evaluate the patients’ physical activity levels and functional capacities. Disability in either ADL or IADL was defined as the inability to carry out one or more activities as outlined in the respective scale.12,13 Cognitive status was evaluated using the mini mental state exam test, with scores below 24 points indicating cognitive dysfunction.14 The Yesavage geriatric depression scale was used to assess depression, with scores above 4 points indicating depression.15 We assessed malnutrition by employing the mini nutritional assessment test. Patients scoring 11 points or less in the initial screening section underwent additional evaluation through the assessment component. Patients achieving a total score exceeding 24 points were classified as having a “normal nutritional status,” those falling within the range of 17-23.5 points were classified as “at risk of malnutrition,” and individuals scoring below 17 points were categorized as “malnourished”.16
Each patient’s height, body weight, upper arm circumference, and calf circumference were measured and documented. Calf circumference measurement was carried out by encircling the broadest part of the left calf with a tape measure while the patient was seated, with their knees bent at a 90-degree angle and both feet resting flat on the floor. The mid-upper arm circumference was measured on the patient’s left arm while they were seated, with their elbow flexed at a 90-degree angle. Arm circumference was assessed by positioning a tape measure between the olecranon and the acromial process and measuring from this midpoint.
Patients underwent an assessment to determine the existence and severity of LUTS, employing the international prostate symptom score (IPSS). The IPSS is a well-established measure intended to assess disease severity and treatment outcomes. The IPSS questionnaire comprises 7 inquiries aimed at evaluating voiding symptoms experienced within the previous month. Depending on the overall score, symptom severity is categorized as either mild (scoring between 0-7), or moderate to severe (scoring between 8-35).17 In this study, we merged these 3 categories into 2: mild (0-7) and moderate to severe symptoms (8-35 points).
Three-step criteria of European working group on sarcopenia in older people (EWGSOP2) were used for the sarcopenia diagnosis.7 Patients’ hand grip strength (measured in kilograms) was assessed with the use of an electronic hand dynamometer (Takei Scientific Instruments, Niigata, Japan). The measurements were obtained while the patients were seated with their elbows flexed at a 90-degree angle. They were instructed to exert their maximum force on the dynamometer, with 3 measurements recorded for both the right and left hands, allowing adequate intervals for rest. The recorded hand grip strength was based on the highest value obtained. We identified low muscle strength by referring to the cut-off values specific to the Turkish population.18 Individuals with muscle strength values below 32 kg were classified as belonging to the low muscle strength group.
Each patient’s muscle mass was evaluated in the morning, following an overnight fast and after completely emptying their bladder, using a portable BIA device (BodyStat QuadScan 4000, Douglas, Isle of Man, UK). Prior to the measurement, the device underwent calibration based on the patients’ age, gender, height, and weight. During the assessment, patients were positioned in a supine posture without any conductive materials on their bodies, and the measurement was carried out using an 800 mA current with a 50 kHz frequency. We computed skeletal muscle mass (SMM) by applying the subsequent formula:19
SMM (kg) = [(height (cm)2 / resistance (ohms) × 0.401) + (gender ×3.825) + (age (years) × -0.071)] + 5.102. (For gender man=1)
We computed the skeletal muscle mass index (SMMI) by dividing SMM (in kilograms) by the square of the patient’s height (in square meters).20 The SMMI values less than 9.2 kg/m2 in men were classified into the group with low muscle mass.18 We assessed the patients’ physical performance using a 4-meter usual walking speed examination, during which we measured gait speed with a stopwatch and recorded gait timing. Individuals with a gait speed not exceeding 0.8 m/sec were placed in the group characterized by low physical performance.18 After the assessments, individuals demonstrating diminished muscle strength (below 32 kg) and reduced muscle mass (SMMI<9.2 kg/m²) were identified as having sarcopenia. Individuals with diminished muscle strength but intact muscle mass were categorized as having dynapenia. Participants who were diagnosed with sarcopenia and additionally exhibited diminished physical performance were classified into the severe sarcopenia group.7
We measured and recorded the patients’ levels of total testosterone, 25 (OH) vitamin D, serum calcium, C-reactive protein (CRP), and sedimentation rates. Blood specimens were collected between 08:00-09:00 am, following an overnight period of fasting. We determined the total testosterone level using an automated chemiluminescence immunoassay system via the UniCel Dxl 800 autoanalyzer (Beckman Coulter, CA, USA), which had an analytical sensitivity of 10 ng/mL. Total prostate-specific antigen (PSA) level was assessed by using the Access Hybritech PSA kit on the Beckman Coulter DXI immunoassay. We determined the serum 25(OH) vitamin D level through the application of high-performance liquid chromatography (Immuchrom GmBH, Heppenheim, Germany). The coefficients of variation for intraassay was less than 3% and for interassay was less than 5%.
Statistical analysis
Categorical variables were expressed using frequencies and percentages, while continuous variables were described using the median and interquartile range (IQR). We used Chi-square tests or Fisher’s exact tests to analyze categorical variables, and the Wilcoxon rank-sum test was applied to evaluate disparities in continuous variables across the 2 groups. To account for potential factors that could influence the severity of LUTS, we carried out a multivariate logistic regression analysis and computed odds ratios (ORs). The outcome variable was the severity of LUTS and the independent variables were presence of sarcopenia, vitamin D levels, and clinically relevant variables that may act as confounders. We regarded p-values below 0.05 as indicative of statistical significance. We used the Statistical Package for the Social Sciences statistics for Windows, version 18.0 (SPSS Inc., Chicago, Ill, USA) to carry out all statistical analyses.
Results
The study included 193 individuals, all aged 60 years and above. Among the patients, 84 (43.5%) exhibited mild LUTS, while 109 (56.5%) presented with moderate to severe LUTS. Table 1 displays the main features of the patients categorized by the severity of LUTS. The patients had a median age of 71 years, with ages ranging from 66-77 years. Patients with mild LUTS symptoms had a median age of 70, while patients with moderate to severe LUTS had a median age of 73 (p<0.001). Marital status and smoking status exhibited consistent characteristics within the various LUTS severity categories. Notably, none of the patients indicated alcohol consumption. While BMI and upper arm circumference did not significantly differ based on LUTS severity, patients with moderate to severe LUTS exhibited a significantly lower calf circumference (p=0.048). Patients with moderate to severe LUTS demonstrated higher CCI levels (p=0.002). A total of 69 (35.8%) of the patients participating in the study were diagnosed with BPH and were currently receiving alpha blocker treatment. The prevalence of BPH was higher among patients with moderate to severe LUTS (p<0.001). Table 2 presents the patients’ geriatric assessment results according to the severity of LUTS. Patients with moderate to severe LUTS showed increased dependence on ADL (p<0.001) and IADL (p=0.003). Additionally, they demonstrated a higher incidence of polypharmacy (p=0.037), depression (p<0.001), urinary incontinence (p<0.001), and falls within the past year (p=0.049). Nevertheless, there were no notable distinctions between the groups regarding malnutrition (p=0.065) and cognitive impairment (p=0.332). Sarcopenia was identified in 48 (24.9%) patients. The moderate to severe LUTS group exhibited a significantly higher prevalence of sarcopenia than the mild LUTS group (p=0.021). Among the group with mild LUTS, sarcopenia was observed in 14 (16.7%) patients, whereas among the group with moderate to severe LUTS, 34 (31.2%) patients had sarcopenia. Upon separate evaluation of the components contributing to sarcopenia, it became evident that muscle strength, gait speed, and muscle mass exhibited lower values within the group characterized by moderate to severe LUTS. The median muscle strength was 31.1 kg in the mild LUTS group, whereas it was 29.3 kg in the moderate to severe LUTS group (p=0.045). The median gait speed was 0.67 m/sec in the mild LUTS group, contrasting with 0.57 m/sec in the moderate to severe LUTS group (p=0.007). The median muscle mass was 10.4 kg/m² in the mild LUTS group and 10.1 kg/m² in the moderate to severe LUTS group (p=0.028).
- Main features of the patients based on the lower urinary tract symptoms severity.
- Comprehensive geriatric assessment results according to the lower urinary tract symptoms severity.
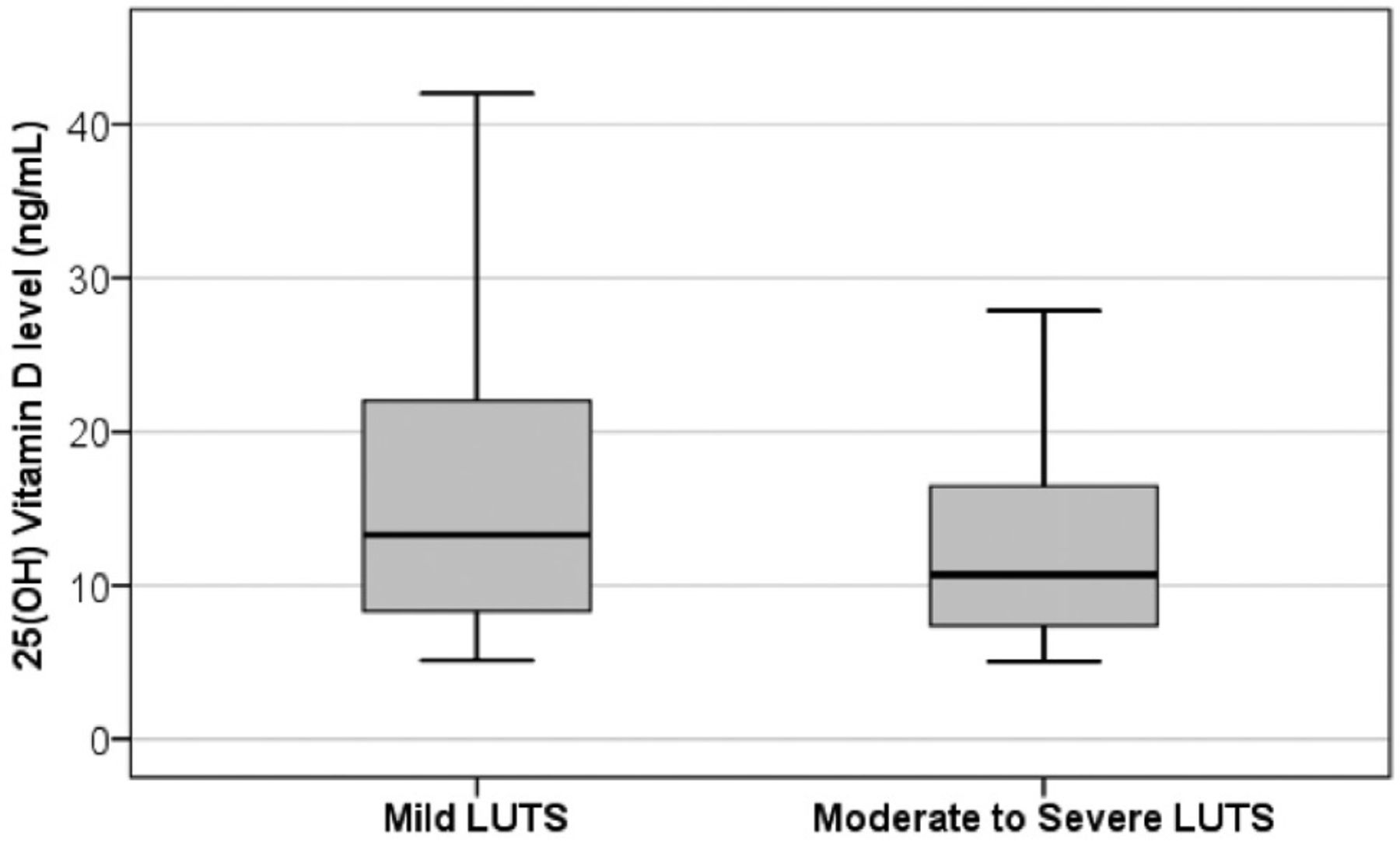
The median serum 25(OH) vitamin D levels were significantly reduced in the moderate to severe LUTS group compared to the mild LUTS group (10.7 vs. 13.3 ng/mL, p=0.027). Furthermore, there was an evident inverse linear association observed between the quartiles of 25(OH) vitamin D and LUTS severity, signifying that the number of patients with moderate to severe LUTS decreased as the quartiles of 25(OH) vitamin D increased (p=0.023; Figure 1).

- Associations of serum 25 (OH) vitamin D levels with lower urinary tract symptoms severity. LUTS: lower urinary tract symptoms
Serum total testosterone, total PSA, serum calcium, CRP levels, and sedimentation rates were similar between the groups. Table 3 provides detailed information on 25(OH) vitamin D levels and additional laboratory results in the mild and moderate to severe LUTS groups.
- The 25 (OH) vitamin D levels and other laboratory results according to the lower urinary tract symptoms severity.
In the multivariate logistic regression analysis, adjusting for age and CCl, there was a significant correlation between vitamin D levels and higher odds of experiencing moderate to severe LUTS (OR=0.95, 95% CI: [0.92-0.98], p=0.002). However, presence of sarcopenia did not exhibit a significant association with the severity of LUTS (OR=2.04, 95%CI: [0.94-4.45], p=0.070; Table 4).
- Results of univariate and multivariate analysis of predictors of lower urinary tract symptoms severity.
Discussion
In this research, we investigated how sarcopenia and vitamin D levels influence the severity of LUTS in older male individuals. Our findings indicate that sarcopenia did not have a significant impact on the severity of LUTS. However, we observed a link between diminished vitamin D levels and moderate to severe LUTS, irrespective of advanced age, a high CCI, and the presence of sarcopenia.
Conflicting findings in the literature complicate the understanding of the relationship between low levels of vitamin D and LUTS. A previous study involving more than 2000 men over 20 years old reported that individuals with low vitamin D levels experienced at least one LUTS.21 It is important to note, though, that not all LUTS were examined in that study, unlike in ours. In another study, it was found that low levels of vitamin D correlated with increased overactive bladder (OAB) symptom scores in men, but did not correlate with higher IPSS scores.22 The expression of VDR has been observed in the smooth muscle layers of the bladder wall and urothelium.9 Therefore, there may be a potential link between the development of LUTS and low vitamin D levels through the manifestation of OAB or urinary incontinence, which can result from abnormal detrusor contractions characterized by either hypercontractility or weakness. Vitamin D has the ability to stimulate the expression of occludin and claudin-14, which are tight junction proteins located at the intercellular junctions of urothelial cells and provide a barrier function. Additionally, the production of cathelicidin and certain other antimicrobial peptides depends upon vitamin D levels, particularly during the infection process.23,24 Consequently, the enhanced expression of these proteins mediated by vitamin D may serve to mitigate bacterial invasion, reduce the occurrence of recurrent urinary tract infections, and potentially alleviate LUTS. Vitamin D could exert various effects on prostate tissue, which could contribute to the prevention of LUTS in men. The presence of the 1α-hydroxylase enzyme in the prostate epithelium allows for the synthesis of 1,25(OH) vitamin D, making it an autocrine hormone within the prostate.22 It was demonstrated that VDR agonists exhibit antiproliferative and proapoptotic effects in BPH cells.25 These protective effects are achieved by inhibiting the inflammatory response through the COX2/PGE2 and NF-KB pathways.26 Furthermore, a specific variant of the vitamin D receptor has been found to have a protective effect against LUTS in men.27 Considering the influence of vitamin D on prostate tissue, particularly in men with LUTS attributed to BPH, reduced vitamin D levels may correlate with the severity of LUTS.
The recent findings from studies indicate that low lean body mass in men is linked to an elevated risk of LUTS, but no significant association has been found between pelvic floor muscle activity and the severity of LUTS.28,29 These results are inconsistent, and there is still limited research on the specific relationship between sarcopenia and LUTS. In contrast to our study, a case-control study carried out with patients diagnosed with systemic sclerosis revealed a significant association between sarcopenia and LUTS.30 However, this study had a relatively small sample size (n=42), consisting of both male and female patients, and included a comparatively younger population (median age of 61 years). These demographic characteristics, as well as the assessment of sarcopenia, differed from those of our study cohort. Another study investigated the association between sarcopenia and OAB in elderly patients with diabetes mellitus, revealing a significant correlation between OAB and sarcopenia.31 However, this study did not assess muscle mass; instead, it relied on a questionnaire for diagnosing sarcopenia. In a separate study exploring the relationship between sarcopenia and OAB, researchers identified sarcopenia as an independent risk factor for OAB.32 But this study included both male and female patients, who were significantly younger (with a mean age of 39) than the participants in our study. Furthermore, sarcopenia was defined using an index derived from the ratio of muscle mass, measured via Dual-energy X-ray absorptiometry, to BMI. Additionally, these studies primarily investigated the association between vitamin D levels and OAB, rather than LUTS.
Both smooth and skeletal muscles play critical roles in maintaining normal urination and urine storage. While sarcopenia may impact pelvic floor skeletal muscles and the external urethral sphincter, which are also skeletal muscles, its role in the development of LUTS in men, particularly in older men, seems to be limited. Moreover, our study’s findings suggest that the relationship between vitamin D deficiency and the severity of LUTS is governed by a distinct mechanism separate from sarcopenia and its impact on skeletal muscles. Considering the existing research that establishes a link between low vitamin D levels and LUTS, our study’s investigation of the relationship between sarcopenia and LUTS in older males, even in the absence of a direct link, contributes to our understanding of these complex factors affecting LUTS.
Study limitations
Lower urinary tract symptoms severity was assessed using a self-assessment questionnaire, and we did not carry out uroflowmetry tests or measure post-void residual urine. These omissions may have inherent limitations in terms of capturing objective measurements, potentially impacting the accuracy and reliability of the results. The study did not consider additional potential variables, such as the presence of urinary tract infections, prostatitis, or the use of medications like diuretics and anticholinergics, which could potentially influence the severity of LUTS. Additionally, it’s essential to note that this cross-sectional study is unable to establish a definitive causal link between low vitamin D levels and the severity of LUTS.
In conclusion, while the presence of sarcopenia did not demonstrate a significant influence on the severity of LUTS, our findings highlight the association between low vitamin D levels and moderate to severe LUTS. Therefore, monitoring serum 25(OH) vitamin D levels in older male patients with LUTS and ensuring appropriate treatment for vitamin D deficiency may offer benefits in managing LUTS, regardless of whether they have sarcopenia or not. However, further prospective trials are needed to explore the roles of sarcopenia and vitamin D in relation to LUTS.
Acknowledgment
The authors gratefully acknowledge EnglishEdited for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 26, 2024.
- Accepted May 6, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.