


ABSTRACT
Cutaneous metastasis of colorectal cancer is uncommon. Therefore, in this case study, we present a unique case of cutaneous metastasis of signet ring adenocarcinoma. The patient presented with generalized asymptomatic subcutaneous nodules 2 years after primary tumor diagnosis. Skin metastasis appeared 3 months before the liver and lung metastasis. However, the patient died 4 months later. Therefore, clinicians should observe signs of distant metastasis of colorectal cancer to enhance survival and improve outcomes.
Colorectal cancer is one of the most prevalent and deadliest malignancies worldwide in both genders. It is the second most prevalent cancer in Saudi Arabia, based on the 2018 statistics of the Saudi National Cancer Registry. The most typical sites of colorectal cancer metastasis are the lungs, bone, and liver.1 Cutaneous metastases from rectal cancer are exceedingly rare and may appear as either an early or late sign of the disease, often mimicking benign skin conditions.2 Diagnosing these metastases might be difficult, as they are rarely considered the primary clinical suspicion. Misdiagnosis is common, particularly when lesions are located in atypical areas, like the face or chest, or when they present as isolated skin abnormalities. Furthermore, skin changes in rectal cancer patients may not always indicate metastasis but could also result from conditions like sarcoidosis or treatment-related side effects, such as radiation dermatitis or secondary infections. A comprehensive skin evaluation in rectal cancer patients is essential for detecting cutaneous metastases and monitoring those treated for the primary tumor.2
Therefore, we present the case of a patient with colorectal cancer and cutaneous metastasis who visited our clinic, to emphasize the importance of observing signs of distant metastasis and carefully examining the skin to improve prognosis and enhance survival.
Case Report
A 65-year-old Saudi male sought medical advice in July 2020, after developing nausea, vomiting, abdominal pain, and constipation. An abdominal radiograph revealed intestinal obstruction. Therefore, the patient underwent laparotomy and left hemicolectomy with resection and anastomosis.
Histopathology confirmed the diagnosis of mucinous adenocarcinoma of the left colon, and staging was determined as PT3N2Mx in August 2020. The patient was referred to the oncologist and received 6 cycles of oxaliplatin and capecitabine and 2 cycles of capecitabine. The first cycle was in September 2020, and the last cycle was in January 2021. Subsequently, the patient’s condition improved, and he was well.
Moreover, in March 2021, the staging changed to PT3N2M0. However, the patient was lost to follow-up by the oncology team for one year. In February 2022, the patient developed generalized asymptomatic plaques and swelling all over the skin. He presented to the dermatology clinic in April 2022 with generalized scattered painless skin swellings and bumps, which started on the trunk and then extended to involve the upper and lower limbs, scalp, and genitalia, with eroded lesions in the axillae and on the scalp.
Clinical findings
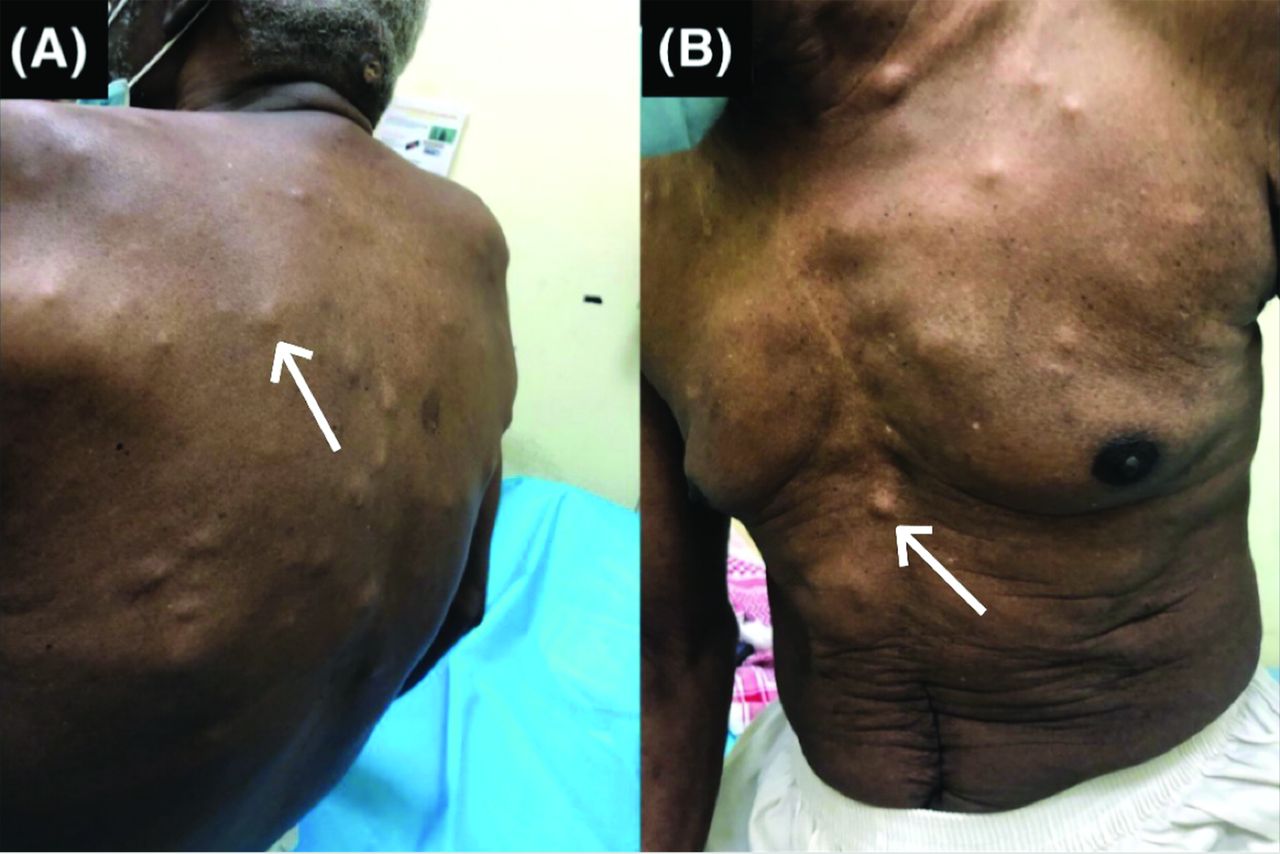
Skin examination revealed generalized skin-colored, rounded, and asymptomatic subcutaneous nodules, mainly over the anterior and posterior trunk; however, the upper and lower extremities, genitalia, and scalp were also involved (Figure 1). Notably, some of the nodules were firm, hard, and varied in size from 1.1-6.6 cm. The lesions on the scalp and in the left axilla were ulcerated plaques and nodules, with a large ulcerative tumor of 7.7 cm in the left axilla (Figure 2).

- Physical examination shows generalized skin-colored, rounded, and asymptomatic subcutaneous nodules over the: A) posterior trunk and B) anterior trunk.

- Large ulcerative tumor 7.7 cm in the left axilla.
Diagnostic assessment
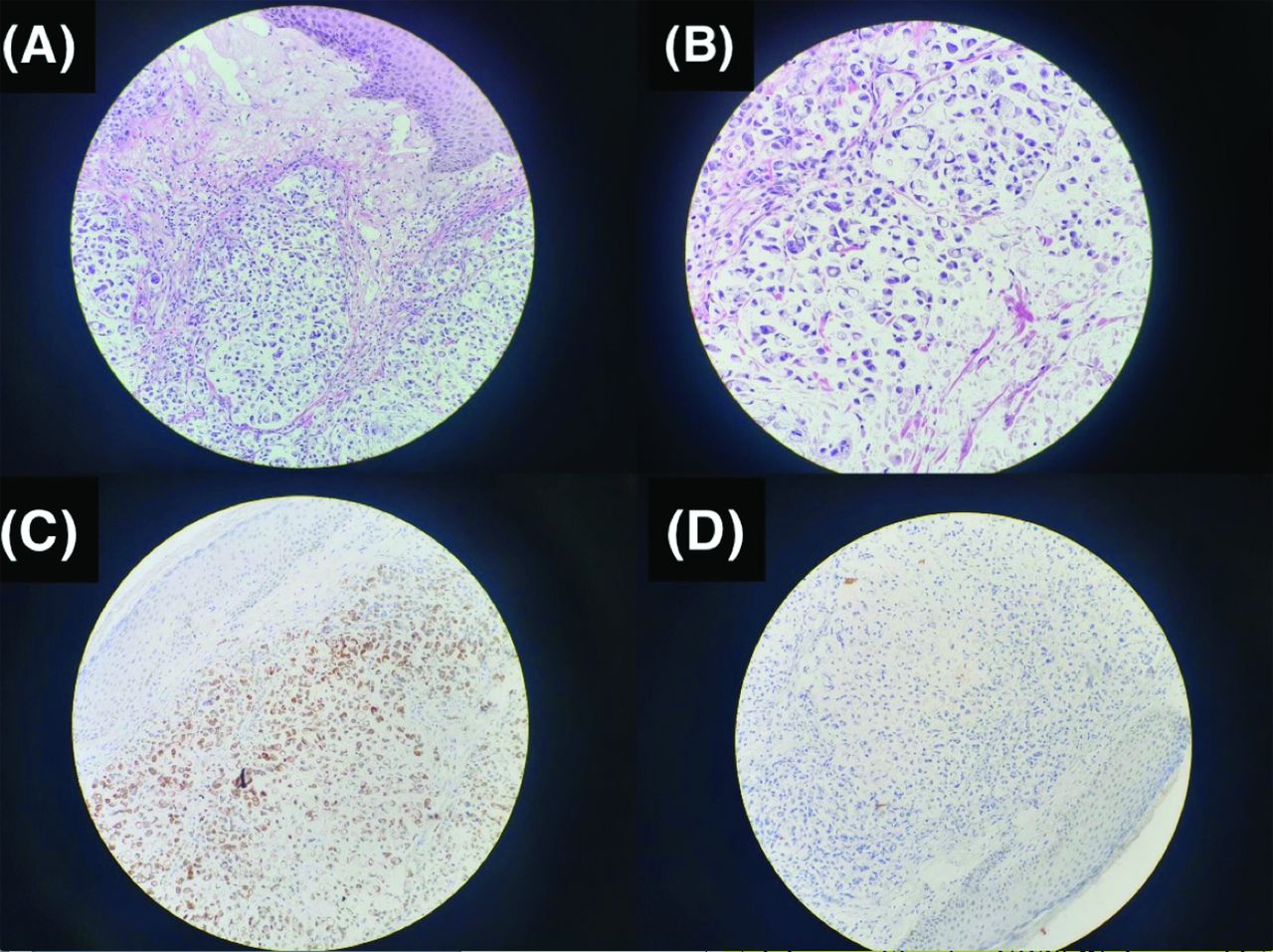
Skin biopsies were obtained, one from the nodule and another from the ulcerated lesion in the left axilla. The morphological findings were consistent with signet ring adenocarcinoma that had spread (Figures 3A&B). The immunohistochemical staining exhibited positivity for cytokeratin 20 (Figure 3C) and negativity for cytokeratin 7 (Figure 3D), thus affirming the colorectal origin.

- Histopathology shows: A) malignant neoplasm composed of clusters of discohesive epithelial tumor cells infiltrating the dermis (hematoxylin & eosin ×100); B) tumor cells with hyperchromatic nuclei pushed aside by intracytoplasmic mucin exhibiting signet ring morphology (hematoxylin & eosin ×400); C) immunohistochemical staining positive for CD20; and D) immunohistochemical staining negative for CK7.
Therapeutic intervention
Notably, few lesions were infected, and they were treated with topical and systemic antibiotics.
Follow-up and outcomes
A few days after presenting to the dermatology department, the patient developed dizziness, abdominal pain, and fatigue. He was transferred to the emergency room in May 2022. He was admitted to the hospital and underwent investigations. Abdominal computed tomography (CT) and CT angiography were carried out, which revealed liver metastases and pulmonary embolism in the sub-segmental branches of the right upper and lower lobes with pulmonary metastases. Therefore, the diagnosis of metastatic colorectal cancer and pulmonary embolism was confirmed.
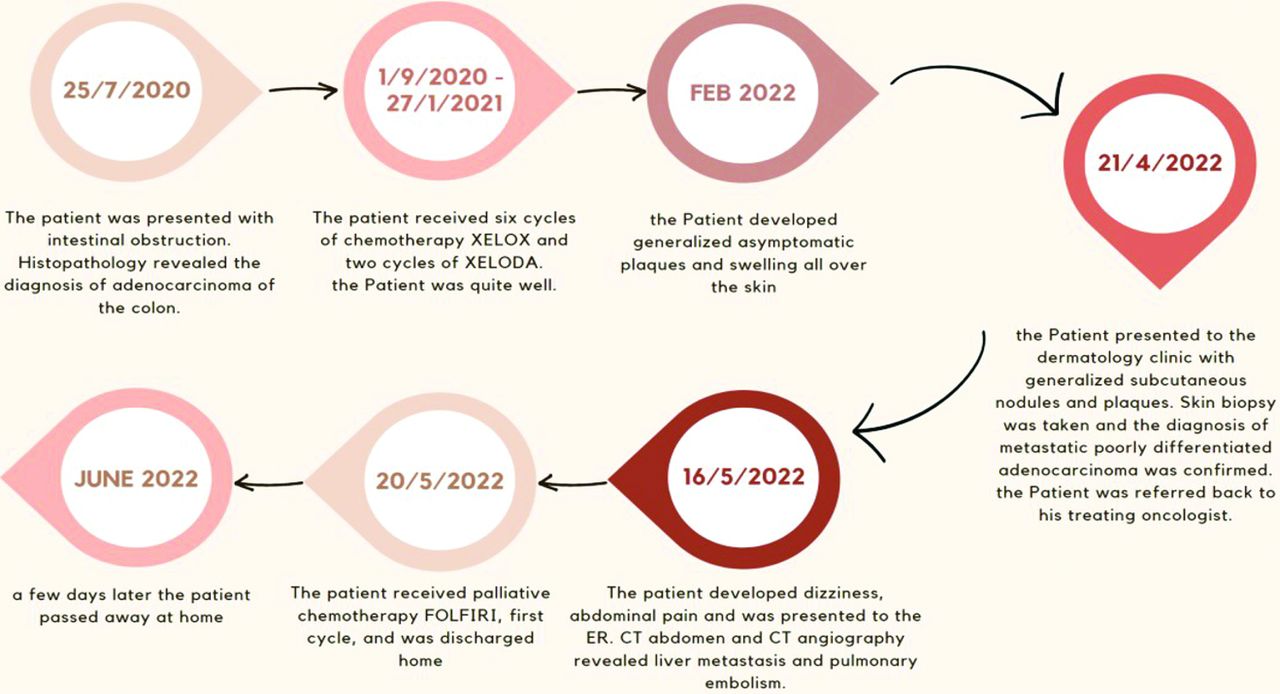
The patient received antibiotics, anticoagulants, and intravenous fluid, and the general condition of the patient improved. The plan of the oncology department at this stage included palliative chemotherapy (FOLFIRI). The patient received the first cycle of the FOLFIRI regimen in May 2022; the therapy was well tolerated, and he was discharged. Unfortunately, the patient died at home a few days later. The key clinical findings and follow-up for this patient are summarized in (Figure 4).

- Timeline of the presented case. ER: emergency room, CT: computed tomography
Discussion
Liver is the most prevalent site of metastasis in rectal cancer, with the lungs and bone following in that order. Therefore, metastasis to locations other than the liver and lungs is rare, and if it develops, it is usually as extensive as liver and lung metastases.1 The skin may be affected in approximately 5% of cases, ranking as the seventh most prevalent cancer in women and the third most prevalent cancer in men. Similar to metastases to other visceral organs, skin metastasis is seen as an indicator of advanced-stage colon cancer.1 The most common presentation of cutaneous metastases is a single lesion (70%), while multiple lesions occur less frequently (30%).3 Cutaneous metastases are linked to a poor prognosis, with an average survival time of approximately 8.5 months following the identification of skin lesions.2
The process of cutaneous metastasis remains unclear. However, spreading through direct expansion of the original tumor to the skin above is involved since these secondary growths appear near the primary tumor.4 This is most frequently observed in the abdomen, particularly near the surgical scars from the excision of the initial tumor. Metastasis can also arise through lymphatic spread, dissemination through the bloodstream, and extension along embryonic remnants like the urachus.4
The surgical scar in the abdomen resulting from the excision of colon cancer is the most typical site for cutaneous metastasis. Metastasis may also arise in pre-existing, unrelated surgical scars; however, reported cases are limited. Furthermore, “Sister Mary Joseph nodule” or umbilical metastasis may be commonly observed. Other cutaneous locations, listed in descending order of prevalence, include the pelvis, back, limbs, thorax, head, and neck.5
Therefore, skin metastasis is identified based on visual characteristics, histomorphology, and immunohistochemistry of the growth.4
A single cutaneous metastasis requires surgical removal. However, for patients with widespread cutaneous metastases, the treatment is exclusively palliative, as they are associated with substantially higher rates of distant metastases, uncontrolled local disease, and decreased survival rates.5
Herein, we present a rare case of skin metastases originating from colorectal cancer. The patient developed asymptomatic cutaneous lesions 3 months before liver and lung involvement, making cutaneous metastasis the first sign of distant metastasis after treating the primary tumor.
A study reviewing 51 cases of rectal cancer with cutaneous metastases observed a gender distribution of 35 (68.6%) males and 16 (31.4%) females. The average age at rectal cancer diagnosis was 57.5 years, ranging from 19-84 years. The average duration between the detection of the primary tumor and the appearance of skin metastases was 17.9 months. In 2 cases, skin metastases were identified simultaneously with the diagnosis of rectal cancer.2
In conclusion, this case report highlights the importance of prompt dermatological examination by the clinician and management of any suspicious cutaneous lesions in patients with visceral cancer, especially colorectal cancer. This would help alter the prognosis, improve the outcome, and allow any changes to the treatment plan.
Acknowledgment
The authors gratefully acknowledge Dr. Maha Hafiz, King Fahad Hospital, Al-Madinah Al-Munawwarah, Kingdom of Saudi Arabia, for her help in reviewing and clarifying patient’s imaging. The authors also would like to thank Editage (www.editage.com) for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 15, 2024.
- Accepted January 26, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.