


Abstract
The horseshoe kidney (HSK) is a common renal abnormality mostly asymptomatic. This may be linked to chromosomal and organ anomalies. A 27-year-old male patient presented with mild recurrent lower abdominal pain associated with dysuria. No history of renal disease. Laboratory investigations revealed red blood cells (RBC), white blood cells (WBC), and bacterial growth in the urine. A CT urogram showed an HSK with a unilateral left-sided ureter. The patient was diagnosed with a urinary tract infection (UTI) and managed with regular follow-up. This report describes a rare case of an HSK with a unilateral left-sided, typically implanted ureter and highlights the radiological findings and management. Asymptomatic HSKs may present with or without associated anomalies. UTI is a common asymptomatic presentation. An HSK with a unilateral left-sided normally implanted ureter is rare. The present case of HSK was associated with recurrent UTI, which was managed accordingly.
The horseshoe kidney (HSK) is a common renal abnormality and is common among males.1 Horseshoe kidney can be located anywhere along the expected direction of normal ascent, from the pelvis to the mid-abdomen. It is characterized by three morphological anomalies: ectopia, malrotation, and changes in vascular supply. Fusion is more common at the lower pole (90% of the cases) and forms a U-shaped HSK.2 Upper pole fusion has been reported in lower percentages, resulting in inverted HSK, while fusion at both poles can cause a disk kidney.2,3 A crossed-fused kidney is described as one crossed to one side and fused by the lower pole of the kidney above and the upper part of the lower pole. In such cases, the ureters maintain their normal insertion into the urinary bladder.3
In 80-85% of HSK cases, the isthmus (site of fusion) contains functioning parenchymal tissue, while the remaining cases contain fibrous tissue.4 The presence of functional parenchymal tissue poses a challenge for surgical intervention. Commonly, the isthmus receives blood supply from the kidneys and, in a few cases, from a separate branch from the aorta, common iliac artery, or inferior mesenteric arteries.5
The HSK is commonly located in a lower position under the inferior mesenteric artery and less commonly between or behind large vessels. The widely accepted theory regarding the development of HSK is the abnormal migration of nephrogenic cells (ureteric bud and metanephric mesenchymal blastema) across the midline, resulting in renal approximation and, consequently, fusion. Another theory describes the alteration of alteration of cell signaling from the abdominal aorta, which acts as a morphogenetic signaling center. Disruption of signaling can disrupt metabolic cell migration.4
The HSK is associated with a broad pattern of variation in the upper urinary tract.6 The variations include the presence of calyces in the upper two-thirds of each kidney, an independent ureter, or an external calyx for the isthmus. Ureters show variations in course, number, and ectopic opening. Although HSK has been reported in identical twins and siblings within the same family, no racial or genetic factors have been linked to HSK.7
Most reported cases of HSK involve bilateral, unilateral, double, or single ectopic ureters.1,4,6,7 This report describes a rare case of an HSK with a unilateral left-sided, typically implanted ureter and highlights the radiological findings and management.
This case was reported in compliance with Helsinki Declaration and approved by the Ethical Approval Committee for Research and Study (King Abdulla Hospital, Bisha, Saudi). The patient signed a consent to publish this report, and his data was used anonymously.
Case Report
Patient Information
A 27-year-old Saudi male patient was referred to the urology outpatient department (KAH-Bisha) from a primary health center with complaints of mild recurrent lower abdominal pain associated with dysuria for further evaluation.
Clinical findings
Upon further evaluation, no history of other lower urinary tract symptoms, gross hematuria, constitutional symptoms, or family history of kidney disease were observed. The physical examination findings were unremarkable.
Diagnostic assessment
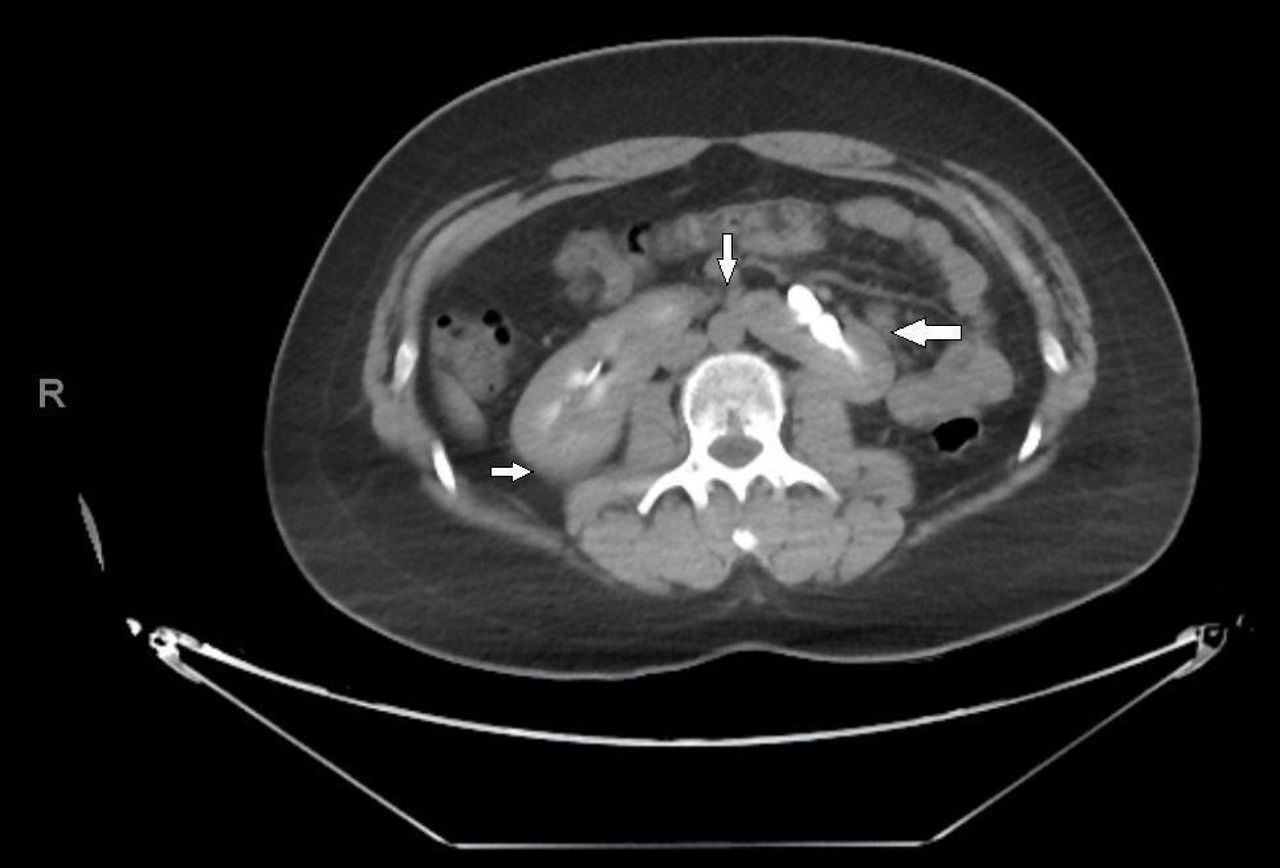
Blood investigations and renal function test (RFT) results were within the normal reference values for gender and age. Urinalysis revealed red blood cells and white blood cells. Urine culture revealed the growth of Escherichia coli. Computed tomography (CT) urogram with a delayed film showed a horseshoe kidney (Figures 1 & 2) with a unilateral left-sided single ureter (Figures 3). A re-evaluation was performed upon detection of HSK. General screening revealed no organ anomalies.

- Axial section of computed tomography urogram with a delayed film of a 27-year-old Saudi male. The section shows fused kidneys in the midline (a horseshoe kidney) (white arrows). The contrast appears bright white in the renal pelvis.

- A coronal section of a computed tomography urogram with a delayed film of a 27-year-old Saudi male. The section shows fused kidneys in the midline (a horseshoe kidney) (white arrows). The contrast appears bright white in the renal pelvis.

- A coronal section of a computed tomography urogram with a delayed film of a 27-year-old Saudi male. The section shows a single left-side ureter (white arrows). The contrast appears bright white in the renal pelvis and the left-side ureter.
Therapeutic intervention
He was counseled regarding HSK, a high-risk urinary tract infection (UTI), and its symptoms. He was advised to urinate frequently, drink water, and consume acidic juices to deter bacterial growth. He was educated on proper wiping. He was prescribed oral antibiotics based on urine culture and sensitivity test results.
Follow-up and outcomes
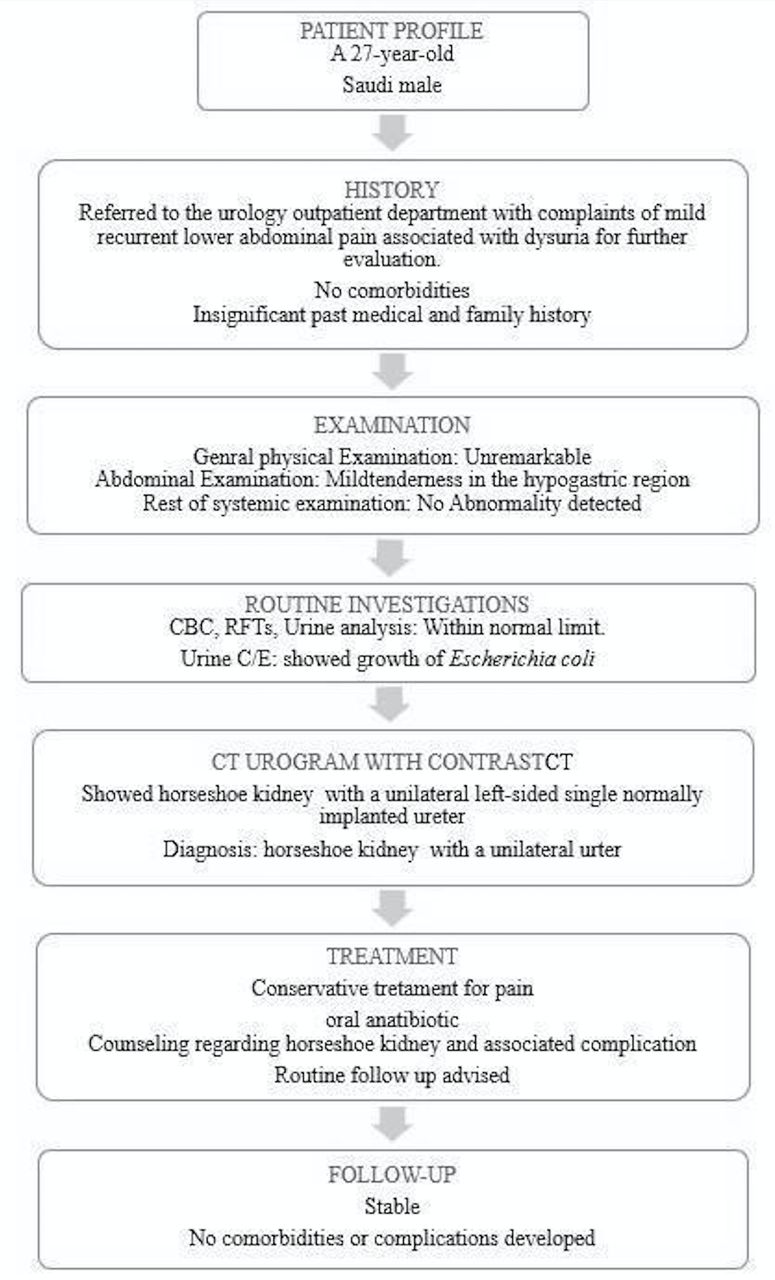
He was planned for a one-year follow-up. The timeline of the his first clinical presentation to follow-up is shown in Figure 4.

- Timeline summarizing the patient’s profile, history, examination, routine investigations, ultrasonography, computed tomography with contrast, diagnosis, treatment, and follow-up.
Discussion
In the current report, he was presented with recurrent UTI symptoms, and HSK was detected during the clinical work-up. Approximately 30% of HSK cases remain asymptomatic, and HSK is commonly detected incidentally during routine investigations with no other anomalies.4 Among the remaining 70%, the most common causes of presentations are UTI, vesicoureteric reflux, ureteropelvic junction obstruction (UPJO), hydronephrosis, and nephrolithiasis.3,4 The UPJO can also cause bacterial infections. Uureteropelvic junction obstruction and hydronephrosis are frequently encountered in HSK, which may result from high ureter insertion into the renal pelvis, abnormal course over the isthmus, atypical vascular supply to the kidney, and intrinsic pathogenesis.2,8 Ureteropelvic junction obstruction can cause a decrease in urine flow down the ureter and an increase in fluid pressure within the kidneys. A decreased urine flow or a decrease in production can precipitate the development of UTI. Patients with both UPJO and UTI may present with the same complaints, including back and lower abdominal pain, nausea, vomiting, and hematuria.8
Radiological findings revealed a unilateral left-sided single ureter that was normally implanted. The presentation of HSK with a single-system ectopic ureter is extremely rare.9 A literature search in PubMed, Google Scholar, and MEDLINE using the keywords “horseshoe, kidney, unilateral, single ureter” gave one case report. Siddiqui et al9 (2023) reported that HSK with a single-system ureter was associated with right-sided hydronephrosis and anorectal malformations. The case reported by Agarwal et al10 (2018) had bilateral ureters, one of which was ectopic. The presence of a unilateral ureter suggests that 2 ureters were developed and one disappeared, or only one ureteric bud developed and then divided into 2 buds that failed to form separate kidneys.
In the present case, the patient presented with UTI symptoms, and the UTI was confirmed by urine culture. UTI is a common presentation of asymptomatic HSK if no other associated anomalies exist. Anatomical abnormalities and disruption of the collecting system in HSK have been described as causes of recurrent UTI and the development of renal stones.2 Asymptomatic HSK may present with UPJO; surgical intervention is not required in such cases unless UPJO is a complication.8
Depending on the urine culture and sensitivity test results, the patient was prescribed an oral antibiotic and scheduled for a one-year follow-up. The clinical analysis did not reveal any other anomalies. The management of HSK is case-dependent based on the clinical presentation. Cases discovered accidentally (asymptotic) can be monitored during regular follow-ups to detect any symptoms of UPJO. Patients with recurrent UTIs should be screened for UPJO, as it can cause UTIs.
In conclusion, HSK with a single, left-sided, normally implanted ureter is a rare congenital condition. Horseshoe kidney can be symptomatic or present as recurrent UTIs. All patients with recurrent UTIs can be screened for HSK. Management of HSK is case-dependent. In the current case, the treatment was conservative with antibiotics for UTI and consulting.
Acknowledgment
The authors acknowledge the patient who participated in this case report and allowed the use of his medical data. They also acknowledge the help and support of their colleagues at King Abdulla Hospital in Bisha and the College of Medicine at the University of Bisha. The authors acknowledge and thank the Department of Radiology King Abdulla Hospital-Bisha for managing and interpreting the radiological images. The authors acknowledge and thank the administration of King Abdulla Hospital-Bisha and the College Dean and Administration of the College of Medicine (University of Bisha, Saudi Arabia) for helping and allowing the use of facilities and resources. We would like to thank www.editaege.com for English language editing for their service.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 25, 2024.
- Accepted December 18, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.