


ABSTRACT
Objectives: To estimate the incidence of AP and determine potential predictors and the outcomes. Elevated lipase level of <3 times the upper limit of normal (ULN) cause diagnostic confusion for acute pancreatitis (AP).
Methods: A multicenter, 6-year retrospective study enrolled adult patients who were detected with lipase level of 80–240 IU/L in the Emergency Department (ED). The Revised Atlanta Classification was used to identify AP within 72 hour (hr) from the first ED visit.
Results: Of 1082 patients, 68 (6.3%) had AP, 393 (36.3%) were hospitalized, 64 (6%) required intensive care unit admission, and 2 (0.2%) died. Most AP cases were confirmed using computed tomography CT; 47 (69.1%), followed by repeated lipase level 15 (22.1%) and ultrasound 14 (20.6%). Alcohol exhibited the highest adjusted odds ratio of predicting AP (3.9–45.6), followed by white blood cell count (1.340–6.222), male gender (1.451–4.308), and higher lipase level (1.009–1.02). Among AP cases, 11.8% required ICU admission and 1 died within 72 hr. Chronic heart disease, obesity, fever, and tachycardia were associated with these critical outcomes.
Conclusion: Among the study sample, 6.3% were diagnosed with AP. Most of the cases confirmed by CT and alcohol was the strongest risk factor in predicting AP. A prediction score system to stratify AP risk when lipase is <3 ULN is warranted.
Acute pancreatitis (AP), which is an acute inflammatory process of the pancreas, is one of the prevalent emergency diseases causing hospitalization.1 Globally, the incidence of AP has increased over time and is associated with significant morbidity and mortality.1,2 Early diagnosis and appropriate severity stratification can prevent disease progression.3,4 The Revised Atlanta Classification indicated meeting 2 out of three criteria to confirm AP diagnosis.5 These criteria included acute upper pancreatic pain, elevated serum lipase that is more than triple the upper limit of normal (ULN), and any radiological finding consistent with AP. An elevated lipase test is carried out to diagnose AP with a sensitivity of 80%–91% if it is increased more than 3 times the ULN.3,6 Lipase starts to increase within 4-8 hours (hr) of the onset of AP symptoms, peaks at 24 hr, and returns to normal within 8-14 days.7
An elevated lipase can be clinically categorized for acute upper abdominal pain according to the elevation as a significant elevation of >3 (ULN), which is diagnostic of AP, and high lipase but <3 ULN are less specific and may not be indicative of AP.8,9 The uncertainty of this category causes diagnostic confusion in emergencies, where rapid decision-making is crucial.8,9 Emergency physicians may discharge the patient and try to arrange close monitoring of repeat lipase, whereas others admit the patient for further evaluation.8,9 Some experts recommended doing a computed tomography (CT) contrast study before the discharge to detect pancreatitis, thereby resolving this diagnostic dilemma.8 Computed tomography is >90% sensitive and specific to diagnosing AP but is not always available in the Emergency Department (ED) or urgent care clinic and is still not free from risks.9 Therefore, others recommend the use of abdominal ultrasound (US) first, and if AP is not confirmed, then CT will be performed.3
A retrospective study for nonspecific abdominal pain was conducted to identify appropriate investigation of patients with mild elevations of amylase or lipase of <3 ULN in the outpatient clinic.10 After extensive radiological investigation and according to the cost-effectiveness balance the study recommend against the investigations for these group patients. However, this study was conducted for outpatient clinics and may not apply to emergency patients with acute abdominal pain.
Another retrospective study for a mild increase in amylase/lipase levels investigates the assumption that lower enzyme levels indicate a milder form of acute early pancreatitis.11 The patients were categorized according to their initial high lipase levels (lipase: ≤3 UNL and >3 UNL). They revealed that the severity and progression of AP are independent of the initial level of elevated amylase/lipase. They found that some clinicians frequently overlooked or underestimated the severity of patients with lipase levels of ≤3 UNL.11
Coronavirus disease 2019 (COVID-19) complicated the interpretation of lipase. Previous studies revealed that COVID-19 is associated with Hyperlipasemia and the majority of them <3 ULN.12,13 It was not clinically associated with AP despite this high prevalence of hyperlipasemia among patients with COVID-19.
This study is to estimate the percentage of those patients who end up diagnosed with AP and to risk stratify them by evaluating the possible predictors guiding safer dispositions as the literature contains no conclusive evidence regarding the diagnostic approach of the emergency patient with mildly elevated lipase.
Methods
This study was conducted in accordance with the principles of the Helsinki Declaration, and the Institutional Review Board (IRB) of Alhabib Medical group approved this study. This study did not involve any experiments on human or animal participants. This is a multicenter, retrospective cohort, observation study of 6 years from January 2017 to January 2023, from the ED of the 4 branches of Dr. Sulaiman Al-Habib Medical Group (HMG) in Riyadh, Saudi Arabia.
The data was retrieved by information technology representatives of our institute as they extracted data for all adult patients (≥18 years) with mild elevated lipase of 80–240 IU/L in the ED from the electronic medical records using the hospital automation system. In our institution, the ULN for lipase was 80 IU/L, whereas 240 IU/L represents 3 ULN, which is consistent with another diagnostic study cut-off14. Our data collector gathered the remaining data by accessing the medical records electronic system (VIDA) by determining the medical record number date and time of the visit and gender. We exclude known cases of patients with chronic pancreatitis or recurrent attacks of pancreatitis (defined as >2 episodes of AP), patients without abdominal pain, abnormal high liver function tests, or patients discharged against medical advice from ED. The abnormal high liver enzyme is defined as elevated alanine transaminase (ALT) of more than triple or elevated direct bilirubin of >50% of high total bilirubin with tripling alkaline phosphatase (ALP) and gamma-glutamyl transferase (ggt), consistent with obstructive jaundice.
Data, including patient demographics, comorbidity, chief complaint, signs and symptoms, laboratory results, CT findings within 72 hr, US findings within 72 hr, mortality rate within 72 hr, repeated lipase within 72 hr, and disposition, were obtained. All of our data collectors were physicians to improve the quality of data collection and the interpretation of the final diagnosis and clinical course. Additionally, we standardize them with an online data collection sheet (Google Sheets), and all the data collectors read the research proposal and attend online meetings to explain the data collection process. The primary investigator frequently monitored the data collection process to notify about any extreme result or missed important element.
The outcome of focus is the highest repeated lipase level within 72 hr and radiological finding within 72 hr. We label the patient as a confirmed case of AP according to the Revised Atlanta Classification if the repeated lipase of >240 or the US or CT finding is consistent with AP. All the radiological report is performed by the radiologist consultant in our institute.
Statistical analysis
Data was analyzed using Statistical Package for the Social Sciences version 26 (IBM Corp., Armonk, N.Y., USA). The descriptive statistics were expressed as frequency, percentages, mean, and standard deviation (SD). The Chi-square test was conducted to find out the association between pancreatitis and pancreatitis respect to categorical demographic of the patients, while independent sample t-test used to find out continues data and logistic regression was presented by crude odd ratio and adjusted odd ratio, with a 95% confidence interval (CI) for both tests. A value of p<0.05 was considered statistically significant.
Results
This study analyzed 1082 patients, of whom 6.3% had AP according to The Revised Atlanta Classification. Additionally, 36.4% of patients were admitted to the hospital, 6% required ICU admission within 72 hours, and 0.2% died. It is evident that the mean age of the whole study population was 46 years, and the gender distribution revealed slightly higher number of male patients (male: 52.1%; females: 47.9%). Moreover, Table 1 shows that 27.8% patients had diabetes mellitus, 24.9% had hypertension, 5.2% had chronic heart disease, 6.5% had ischemic heart disease, 6.4% had chronic renal disease, and 21.1% had gallstone.
- Comparison of demographic, clinical, and laboratory variables between patients with and without acute pancreatitis.
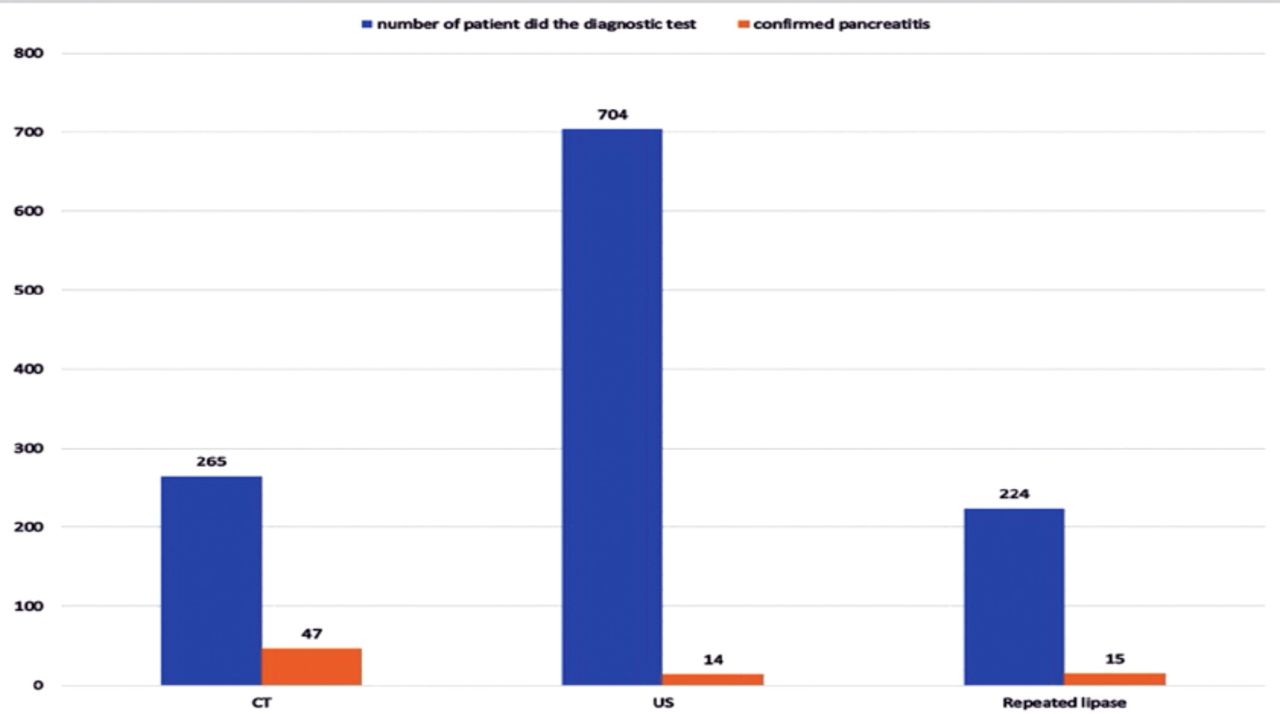
Figure 1 illustrates the number of patients and confirmed AP cases. The statistics indicated that 47 (17.7%) of 265 patients tested by CT exhibited pancreatitis, only 2% of patients using US had AP, and 6.7% patients undergoing repeated lipase tests demonstrated pancreatitis. A total of 7 (10.3%) cases were diagnosed solely by repeated lipase.

- Distribution of the number of patients with confirmed acute pancreatitis according to diagnostic tests. CT: computed tomography, US: ultrasound
Table 1 shows an analysis of the comparison of AP predictors with the Chi-square test and independent sample t-test. Male patients represent 52.1% (n=564 of 1082) of the cases, including 72.1% (n=49) in the pancreatitis group and 50.8% (n=515) in the non-pancreatitis group (p<0.05). Lipase level had a mean (SD) of 123.5 (42.6), and the comparison across the two groups in terms of outcomes demonstrated a high statistically significant difference in a mean (SD) of 156.0 (46.4) for the pancreatitis group and 121.4 (41.4) for the non-pancreatitis group (p<0.05). White blood cell (WBC) count was statistically different in both continuous and categorical variables with a cut-of value of <3 or >14.9 mm3. White blood cell comparison indicated a mean (SD) of 10.1 (4.4) mm3 in the pancreatitis group and 8.3 (3.4) mm3 in the non-pancreatitis group (p<0.05), and the comparison of categorical variables revealed 13.2% (n=9) of patients with pancreatitis and 4.7% (n=48) with no pancreatitis (p= 0.002). This is the opposite with urea, with a cut-off value of 8.92 mmol/L. Urea demonstrated a mean (SD) of 6.0 (6.5) mmol/L. The comparison revealed a mean (SD) of 4.2 (1.9) mmol/L in the pancreatitis group and 6.1 (6.7) mmol/L in the non-pancreatitis group (p<0.05), and categorical analysis indicated that 1.9% (n = 1) of patients had pancreatitis, whereas 11.3% (n = 91) had no pancreatitis (p=0.030).
The comparison across for ALT between the two groups revealed significant differences with a mean (SD) of 43.5 (78.4) in the pancreatitis group and 30.8 (34.7) in the non-pancreatitis groups (p=0.016). Calcium demonstrated a statistical difference in categorical, with a cut-off value of 8 g/dL (p<0.05), but urea indicated an association in those without AP. AP, statistically significant differences for hospital admission requiring intensive care unit (ICU) admission, and mortality indicated p-values of 0.000, 0.037, and 0.023, respectively.
Table 2 presents associated factors using logistic regression with outcomes being binary: pancreatitis or non-pancreatitis. Male was considered a statistically significant factor (p=0.001) with a crude odd ratio (OR) of 2.499 and 95% CI of 1.451–4.304. The OR of male was 2.5 (95% CI: 1.451–4.308) after adjusting for age. Remarkably, alcohol was associated with pancreatitis, with the highest crude OR of 17.956 and the adjusted OR of 13.267. Pulse rate exhibited a statistically significant risk factor as continuous variables (p=0.030, crude OR: 1.019, 95% CI: 1.002–1.036; adjusted OR: 1.020, and 95% CI:1.003–1.037). Moreover, lipase level (continuous) demonstrated a high statistically significant risk factor (p=0.000 for both crude and adjusted ORs). WBCs were highly statistically significant for continuous analysis, with a cut-off of <3.0 or >14.9 mm3, a crude OR of 1.116 (95% CI: 1.055–1.180), and an adjusted OR of 1.103. Furthermore, WBCs with a cut-off of <3.0 or >14.9 mm3 indicated a statistically significant association with an OR of 3.070 and an adjusted OR of 2.887.
- Comparison of AP predictor using logistic regression.
Table 3 represents an analysis of mortality or ICU admission predictor within 72 hr among AP cases, categorizing them into 2 groups of mortality or ICU admission (critical group) and no mortality or ICU admission (non-critical group). Chronic heart disease was observed in 4.5% (n=3 of 68) of the cases, including 22.2% in the critical group and 1.7% in the non-critical group (p=0.006). Furthermore, pulse rate indicated a statistically significant difference (p=0.025), including 22.2% of patients in the critical group and 3.4% in the non-critical group. Finally, body mass index (BMI) (continuous analysis) exhibited a strong statistically significant difference in mortality or ICU admission within AP (p=0.041, with a mean [SD] of 41.8 [0.1] in the critical group and 28.1 [5.0] in the non-critical group.
- Predictor of mortality or ICU admission within 72 hr among acute pancreatitis cases.
Discussion
This is the first study to describe patients with mild lipase elevation in ED. This multicenter study revealed that 1082 patients met our inclusion-exclusion criteria with a mean initial lipase level of 123.5 ± 42.6 IU/L. Their mean age was 46 years and approximately one-third of patients were admitted to the hospital (n=393) and 6.3% were diagnosed with AP (n=68).
Most AP cases were confirmed using CT (69.1%), followed by repeated lipase levels (22.1%) and US (20.6%). From a different perspective, AP was diagnosed in 17.7% of patients who underwent CT scans, 7% of those who had repeated laboratory tests, and 2% of patients who did ultrasounds. This indicated the higher yield of CT in the ED compared to other diagnostic modalities, not only confirming AP faster but also rolling out other deferential that cause high lipase. We concur with the case series of eight AP cases in the ED with completely normal initial lipase as they revealed that serially trending lipase was less likely to yield to diagnostic level, and they recommended early CT.15 Remarkable finding in the current study about the CT utilization in which only (24.5%) of the patients underwent CT within 72 hours for their abdominal pain, which is below what was reported in a cross-sectional study which found (83%) confirmed AP cases had CT performed in ER or during their hospital course.16 Therefore, we recommend against admitting these cases for monitoring the lipase for the diagnosis while CT is feasible.
Among AP cases, 55 (80%) were admitted from the first ED visit, indicating that approximately 20% of AP cases were prematurely discharged without picking the appropriate diagnosis and the diagnosis was made in the follow-up clinic or after repeated ED visits within 72 hr. This confirms that some clinicians still underestimate the cases with mildly elevated lipase levels.11
We determined predictors that are associated with AP to be male gender, alcohol intake, higher lipase level, abnormal WBC count, and higher ALT. Male gender and alcohol intake are risk factors for pancreatitis, and our result revealed an adjusted OR of 1.387–4.153 for the male gender, whereas the highest adjusted OR was associated with alcohol intake at 3.9–45.617. Gallbladder stone is another known risk factor for biliary pancreatitis, and this explains our negative correlation as we excluded cases with labs consistent with obstructive jaundice. Table 2 shows that the clinical presentation failed to predict AP, which can be explained by the nonspecific signs and symptoms mimicking AP and the symptomatic management that may mask the diagnosis. A retrospective study from Thailand was conducted to predict AP without relying on lipase or diagnostic radiological tests.18 Consistent with our study, they revealed that clinical manifestations of the surgical abdomen, such as guarding and rebound tenderness, cannot predict AP, whereas a history of alcohol drinking increases the likelihood of the diagnosis. However, they demonstrated that pain characteristics and vomiting indicate a diagnosis that was not found in our study, which may be attributed to different inclusion and exclusion criteria. Our study agreed with others that amylase did not help and failed to add diagnostic value to lipase levels.19,20
Among our 68 confirmed AP cases, 8 (11.8%) required ICU admission and only 1 patient died within 72 hr. Interestingly, this percentage is higher than 2 studies conducted in Saudi Arabia reported an ICU admission rate of 5%–9%.21,22 This may be attributed to the clinician’s decision when the lipase of <3 ULN delayed the full management or hesitated to do the workout determining the etiology that causes disease progression. In other respects, this may be attributed to the lower threshold of ICU admission in the private sector. However, recent multicenter international studies revealed the rate of ICU admission at 7.6–13.3%.23,24
Regarding our patients with AP, we revealed an association between ICU admission and chronic heart disease and obesity, fever, and heart rate of ≥109 bpm. Furthermore, an earlier literature revealed that obesity increase the risk of worse outcome among AP cases.25,26 Thus, we recommend lowering the threshold for ICU admission for those patients with one or more of these risk factors or considering starting the management empirically if confirming the diagnosis is subject to delay. The remaining classical risk factors for deterioration that were adapted from various severity scoring systems failed to predict ICU admission. We highly recommend establishing a special prediction score system for risk stratification of AP with lipase of <3 ULN.
This research has some limitations despite being a multicenter study. First, all of the study centers were located in one city in Saudi Arabia (Riyadh), which affected the generalizability of the study results. We faced difficulty collecting data in several aspects due to the retrospective nature of the study. Specifically, not all patients had regular follow-ups within 72 hours at our institutes. Therefore, we cannot definitively label the 6.3% confirmed cases of pancreatitis as the true incidence rate, which may actually be higher. Additionally, some emergency department documentation was poor or not fully detailed regarding clinical presentation, and not all important laboratory results were ordered during the initial visit. Furthermore, we did not specify the staging of reported comorbidities, especially in relation to chronic renal disease and whether the patient was on dialysis, which could affect lipase interpretation. Finally, the uniqueness of this emergency department study challenges us to place our findings in the context of comparison in order to validate our recommendations.
In conclusion, this study found that among emergency patients with mild lipase elevations (<3 ULN), 6.3% were diagnosed with AP. Given the higher diagnostic yield of CT, we recommend integrating CT scans into the diagnostic protocols for those patients. Alcohol was the strongest risk factor that predicted the diagnosis. Among the confirmed AP cases 11.8% required ICU admission within 72 hr. We urge clinicians to lower the threshold for ICU admissions in patients with risk factors for deterioration, and emphasizing the need for a proactive approach in managing AP. We recommend establishing a special prediction score system to risk stratify AP when the lipase <3 ULN.
Acknowledgment
This study was supported by the College of Prince Sultan Bin Abdulaziz for Emergency Medical Services, Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia. We would like to express our appreciation to the Deanship of Scientific Research at King Saud University.The authors acknowledge Enago (Crimson Interactive Inc.) for providing professional English language editing services for this manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 14, 2024.
- Accepted March 2, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.