


Abstract
Objectives: To present an unusual major mechanical complication of central venous catheterization (CVC).
Methods: Between January 2016 and January 2017, data of the patients who underwent CVC in Cumhuriyet University in Sivas, Turkey, were retrospectively reviewed. The patients who experienced an unusual mechanical catheter-related complication are included in this study. Other complications of central venous catheter placement, except mechanical catheter complications such as infection or thrombosis, were excluded from the study.
Results: A total of 236 consecutive patients who had undergone CVC were found. Nine patients (3.8%) were found to have unusual major mechanical catheter complications. Most noteworthy complications occurred when the catheter was placed in the arcus aorta, ductus thoracicus, pleural cavity, and abdominal cavity. The most common observation in patients with major complications was that CVC had been carried out in the absence of ultrasonic or fluoroscopic guidance owing to emergency situations.
Conclusion: The use of CVC is associated with potential major complications occurring particularly during emergency situations. We believe that the use of radiological guidance during CVC could reduce unusual major mechanical complication rates even during an emergency situation.
Central venous catheterization (CVC) is frequently necessary to treat critically ill patients admitted to both emergency and intensive care units.1 A continuous increase in the population of critically ill patients has led to an increase in the number of patients requiring CVC. Central venous catheters are an essential part of vascular access that are useful for rapid fluid or blood replacement, parenteral nutrition, hemodynamic monitoring, administration of drugs which can likely induce phlebitis, placement of a temporary cardiac pacemaker, and hemodialysis. Although CVC is an essential part of medical treatment in patients admitted to the emergency unit or ICU, the procedure for placing this catheter is associated with adverse events including patient fatality and high medical costs.2,3 It has been reported that mechanical complications occur in 5-19% of patients who undergo CVC.4,5 Mechanical complications are of high concern because their effects include arterial puncture, failure of catheter placement, pneumothorax, pulmonary embolism, and death. Complications such as pneumothorax or hemorrhage that warrant specific therapeutic procedures such as chest tube insertion for pneumothorax or blood transfusion/surgical procedure for hemorrhage, were defined as major mechanical complications. The unusual major mechanical complications such as intra-arterial cannulation, extravascular catheterization, or intravenous misplacement of the catheter tip can lead to more serious and life-threatening conditions that could be both fatal and expensive to treat. In this study, we aimed to emphasize the unusual mechanical complications of CVC.
Methods
The study was approved by the local ethics committee (2017-04/07). Between January 2016 and January 2017, the hospital medical records and electronic database of all patients who underwent CVC were retrospectively reviewed by a researcher. We found 236 consecutive patients who had undergone CVC. Details regarding the catheter, indications of catheter placement, and mechanical catheter complications were obtained from patient hospital records. Nine patients were found to have major mechanical catheter complications. All patients who experienced mechanical catheter complication were included in the study. Other complications of CVC, except mechanical catheter complications, were excluded from the study.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Science software (SPSS) for Windows, version 22.0, (IBM Corp., Armonk, NY, USA). Descriptive statistics were expressed in mean, standard deviation (SD), number, and percentage. Selected demographic and clinical data such as gender, catheter placement technique, patient situation during CVC, and catheterization site were analyzed with the χ2 test. A p-value of 0.05 or less was considered to be statistically significant.
Results
After reviewing the medical records between January 2016 and January 2017, we found 236 consecutive patients who had undergone CVC. Indications of CVC were hemodialysis 163 (69.1%), fluid replacement and chemotherapy 69 (29.2%), and hemodynamic monitoring 4 (1.7%). The mean age of the patients was 68.93±14.29 years, and 119 patients were females while 117 were males. Two hundred (84.7%) central venous catheters were of the non-tunneled temporary type, and 36 (15.3%) were of the cuffed tunneled type having implantable venous access ports. A total of 128 (54.2%) catheters were placed using the anatomic landmark method without ultrasonic or fluoroscopic guidance. Table 1 summarizes the data of our CVC patients.
Patient characteristics.
Nine patients (3.8%) were found to have major mechanical catheter complications. We calculated estimate CVC complication rate as 0.038 (95% CI, 0.019; 0.079). These complications varied from intravenous misplacement of the catheter tip to intra-aortic or extravascular placement of the catheter. In all the patients having major CVC complications, CVC was performed in the emergency department in the absence of ultrasonic or fluoroscopic guidance because of the urgent need to treat patients owing to profound hypotension or hypovolemic shock or to perform CPR. Table 2 shows the characteristics of CVC patients with unusual major mechanical complications.
Characteristics of CVC patients with unusual mechanical complications.
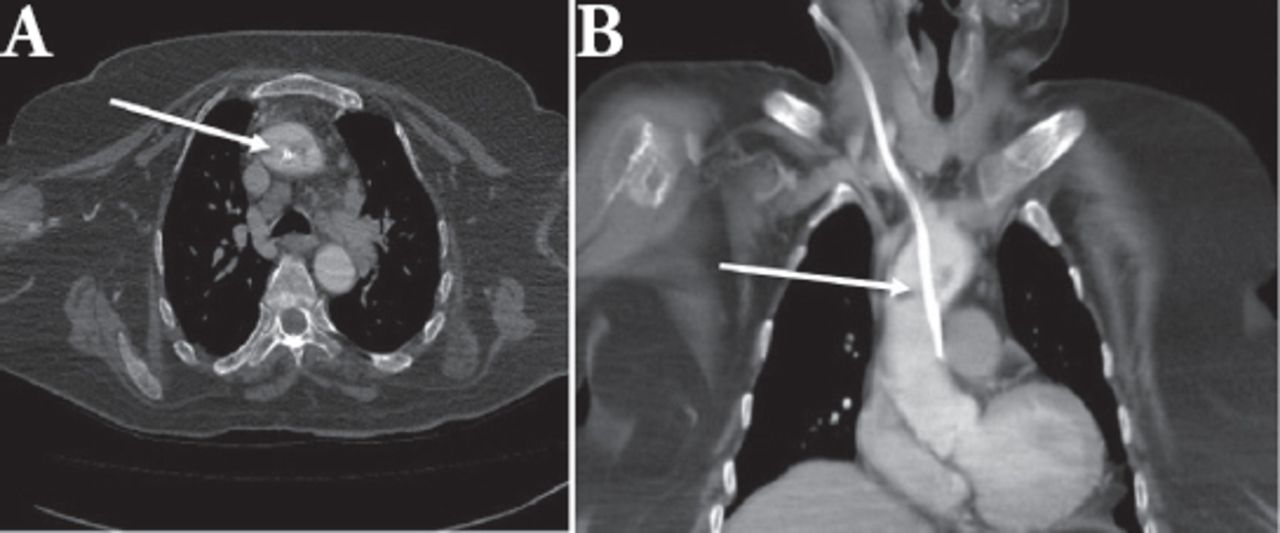
In our study, the most interesting complication occurred due to accidental aortic catheterization via the right carotid artery. One case was of an 80-year-old female patient who had chronic kidney disease and diabetes mellitus. She was admitted to the emergency department owing to the complaints of profound hypotension and arteriovenous fistula thrombosis. Due to this emergency situation, a central venous catheter was placed through the right jugular vein at the emergency unit of the hospital. After multiple hemodialysis sessions and medication, it was observed that the patient’s blood pressure became normotensive, and then the central venous catheter pulsation became synchronized with the heartbeat. Thoracic computed tomography (CT) showed that the central venous catheter was inserted in the right carotid artery and that the catheter tip was placed in the arcus aorta (Figure 1). Interestingly, the patient did not experience any neurological complications or embolism.
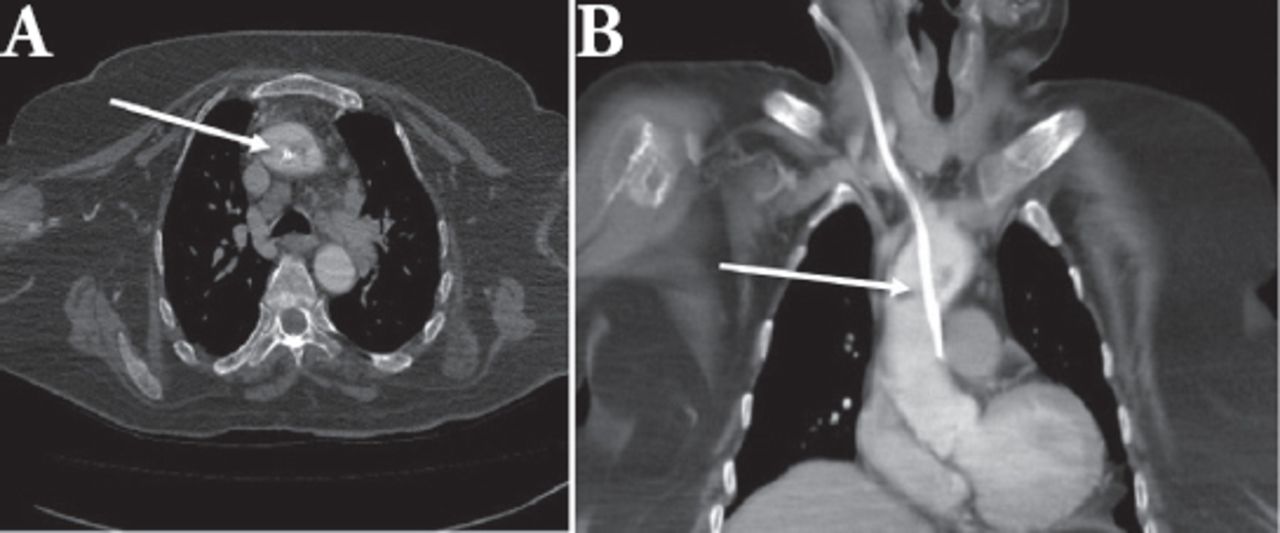
Catheter tip placed in the ascending aorta. A) axial plane, B) coronal plane of computed tomography images.
Another case was of a 71-year-old male patient who had a history of prostate cancer and who was admitted to the emergency unit of the hospital owing to acute kidney failure. Insertion of the central venous catheter through the left jugular vein was performed at the emergency unit, and the patient was subsequently transferred to the hemodialysis unit. A nurse at the hemodialysis unit observed that initially, blood was drawn into the syringe from the catheter following which the color of aspiration fluid became clear and milky/pinkish white (Figure 2a). Thoracic CT showed that the catheter tip was placed at the ductus thoracicus. Because of brachiocephalic vein thrombosis, the aspiration material drawn from the catheter was intensive lymphatic fluid mixed with blood (Figure 2b).

Catheter tip placed at the A) ductus thoracicus, B) color of aspiration fluid was milky/pinkish white.
Discussion
Central venous catheterization is not always an easy procedure, especially in an emergency situation. It is a surgical procedure that cannot be postponed in patients admitted to the emergency unit or ICU, regardless of the risk involved. It may result in adverse outcomes that are both hazardous and expensive to treat.2 The studies have shown that mechanical complications occur in approximately 19% of the patients.2,4,5
Arterial puncture is the most frequent mechanical complication of CVC that can cause hematoma, when the catheter insertion is performed using the blind landmark method.3 Some anatomical landmarks are beneficial for locating the target vessel according to the selected catheterization region.5,6 The apex of the 2 heads of the sternocleidomastoid muscle, carotid artery, ipsilateral nipple, and clavicle are anatomical landmarks that are used while performing CVC via the jugular veins. However, these landmarks are not always clearly visible in all patients. Especially, in obese patients, the apex of the 2 heads of the sternocleidomastoid muscle cannot be easily visualized. Although arterial puncture can be easily identified in patients with normal blood pressure and normal arterial oxygen saturation level, in case of profound hypotension or arterial desaturation, it is challenging to identify whether the needle tip is being targeted to the artery or vein. Therefore, CVC can be misplaced intra-arterially. This is the most serious complication that can lead to arterial injury (femoral, iliac, or carotid arteries), cerebrovascular embolism, or embolism in other organs. In one of our cases, in a patient who had profound hypotension, CVC was inserted into the ascending aorta via the right carotid artery using the blind landmark method. After multiple hemodialysis sessions and after the patient’s blood pressure became normotensive, we noticed that the patient’s central venous catheter was placed in the aorta.
We noted in our study that all the CVC procedures that led to major complications were performed during emergency situations. Although it may be considered that there is insufficient time to use ultrasonography while performing CVC in an emergency situation, studies revealed that the use of ultrasound guidance during CVC instead of a blind landmark method reduces CVC time and rates of unsuccessful catheterization as well as the incidence of carotid artery puncture and hematoma.7,8
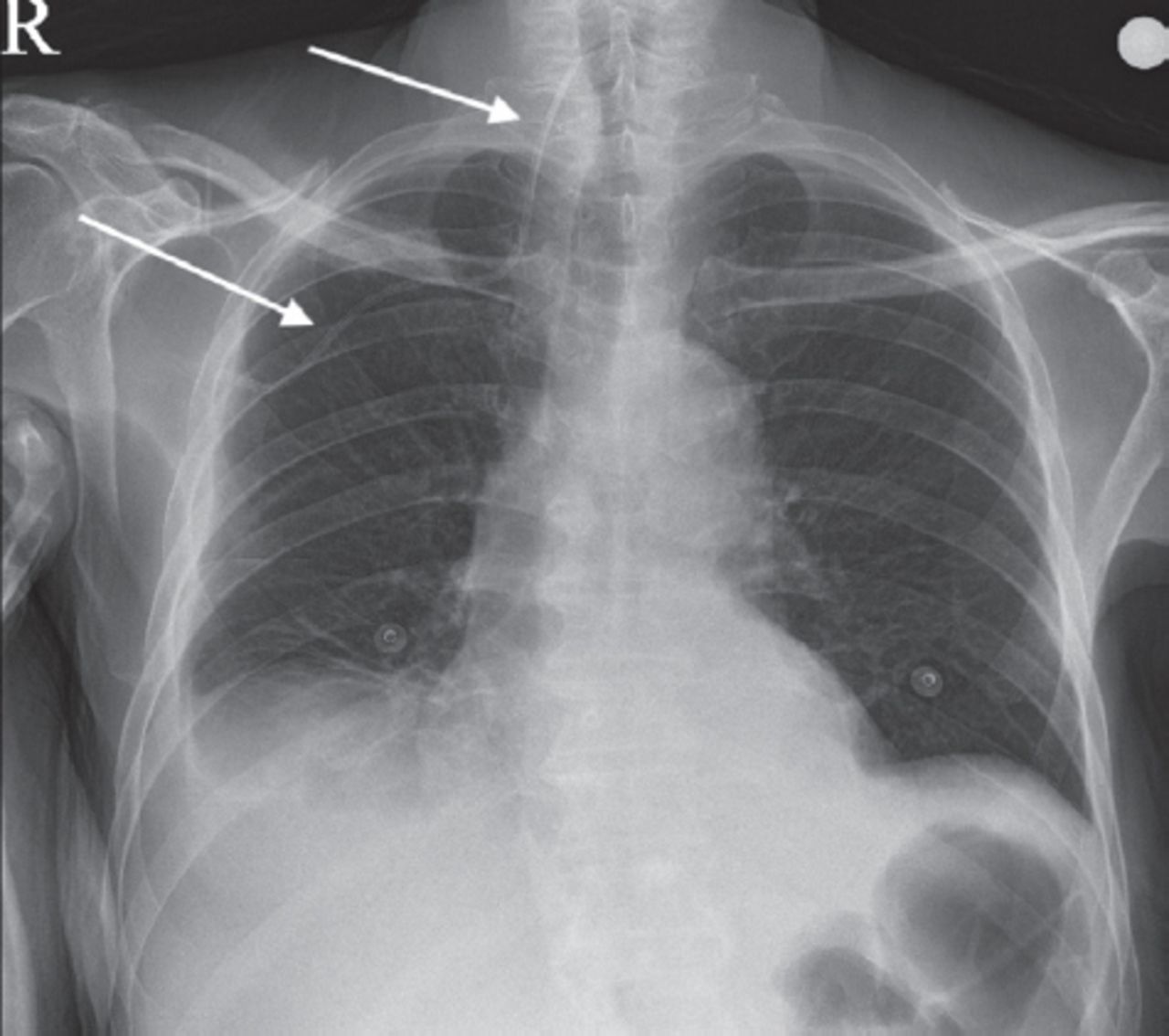
Intravascular or extravascular malposition of the catheter tip is another important unusual major mechanical complication of CVC. Intravenous misplacement of the catheter tip can lead to traumatic vascular complications, thrombosis, and impaired catheter function. In our study, 3 catheters tips had been incorrectly placed, which necessitated catheter removal. One of them, due to the brachiocephalic vein occlusion tip of subclavian catheter was turned into jugular vein (Figure 3), another femoral venous catheter tip was in the hepatic vein related catheter patient mismatch and catheter tip in ductus thoracicus. The function of the 3 catheters was impaired and thus all the catheters were removed. Deitel and McIntyre9 suggested that the malposition rate of catheters which were inserted in the absence of fluoroscopic guidance was as high as 29%. For CVC performed using fluoroscopic guidance, it is important to ensure that the tip of the catheter is placed in the correct position. Due to the critical condition of patients during an emergency or of those admitted in ICUs, it is not possible to carry out CVC under fluoroscopic guidance for all the patients. However, we believe that catheter tip misplacement rates can be reduced by performing CVC under fluoroscopic control at least for all the eligible patients.

Tip of subclavian catheter turned into jugular vein.
In conclusion, complications were observed after CVC and unusual major mechanical complications are obviously related to CVC placement, especially in emergency situations. We believe that the use of ultrasonic guidance or fluoroscopic guidance during CVC placement could reduce unusual major mechanical complication rates even during emergency situations.
Acknowledgment
We would like to thank Prof. Dr. Cesur Gümüs and Dr. Senor Elbir for reviewing the radiological images. We also would like to thank Wordvice (https://wordvice.com.tr/) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 9, 2018.
- Accepted January 16, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}