


Abstract
Objectives: To assess the quality of life (QoL) in patients with vitiligo in central Saudi Arabia using the dermatology life quality index (DLQI).
Methods: A cross-sectional study spanning over 6 months was conducted on 253 adult patients with vitiligo at the outpatient dermatology clinics of the National Center of Vitiligo (Light Clinics) and King Khalid University Hospital, Riyadh, Saudi Arabia. The patients were asked to complete a self-administered questionnaire using an Arabic version of the DLQI to measure the impact of vitiligo on their QoL. The association between the demographic and diseases characteristic to the median DLQI scores was investigated using binary logistic regression.
Results: The median DLQI score was 4, the range 25, min 0 - max 25 and percentiles 2-8. The unadjusted odds ratio (95%CI) showed the median DLQI score was significantly higher in married subjects 2.29 (1.33-3.94) (p<0.01), non-segmental vitiligo 2.10 (1.16-3.79) (p<0.01), and the progressive vitiligo 1.87 (1.09-3.18) (p<0.02) than their counterparts. However, after adjustment only married status predicted the high DLQI score 2.08 (1.11-3.61) (p<0.01).
Conclusion: The QoL in vitiligo patients in Saudi Arabia is adverse than those with lighter skin, in other countries. Therefore, in Saudi Arabia, better management modalities to improve patients’ QoL and prevent subsequent mental distress are needed.
Vitiligo is a long-standing idiopathic depigmentary disorder which is progressive destruction of melanocytes.1,2 Among depigmenting disorders, vitiligo is the most prevalent, with a proximate prevalence of 0.5-2% of the world’s population.2 While vitiligo is not a life-threatening disorder, it disfigures the patient’s appearance leading to discrimination due to infection fear or just disgust. Patients with vitiligo tend to have poor body image, low self-esteem, impaired quality of life (QoL), and psychological problems such as depression, anxiety, and social phobia.3-6 Quality of life in dermatology refers to the subjective perception of the patients toward their skin condition.7 In vitiligo, QoL is one of the primary outcomes of the treatment.8 The most widely used tool to assess the QoL in patients with dermatological disorders is the Dermatology Life Quality Index (DLQI).9-11 It has been used to measure vitiligo QoL in many countries and has been used to monitor the treatment’s effectiveness in several randomized clinical trials.3,8 The widespread use of DLQI and its availability in different languages and cultures allows cross-cultural comparison and facilitates more straightforward interpretability and utility of the data obtained from international studies, especially clinical trials.12
Previously published studies do not have enough literature on QoL in patients with vitiligo in Saudi Arabia, therefore, we conducted this study at the National Center of Vitiligo (Light Clinics) and King Khalid University Hospital, Riyadh, Saudi Arabia to assess the QoL in Saudi vitiligo patients and determine the association between their QoL and demographic and disease characteristics.
Methods
This is a cross-sectional study on 253 adults with vitiligo at the outpatient dermatology clinics of the National Center of Vitiligo (Light Clinics) and King Khalid University Hospital, Riyadh, Saudi Arabia. From April to September 2020, patients were included if they: a) had a confirmed diagnosis of vitiligo by dermatologists, b) 16 years old and above, and c) Saudis of both genders. Patients were excluded if they: a) had cognitive problems, b) refused to participate, and c) were difficult to communicate with. This study aimed to assess QoL in patients with vitiligo in Saudi Arabia. The expected prevalence of QoL impairment based on previous studies was 90.1%.13 So taking 5% precision and 95% confidence level, the estimated sample size was 138. We increased our sample to increase precision and avoid bias. First, consecutive adult vitiligo patients attending the previously named clinics completed a self-administered questionnaire.
A validated Arabic version of the DLQI questionnaire was used. We obtained the permission of A.Y. Finlay (University of Wales College of Medicine, Cardiff, U.K.) to use the questionnaire. The DLQI composed of 10 questions and the score of each question ranges from 0 to 3. The range of the total DLQI score is from 0 to 30; high DLQI score indicates more impairment in QoL. Dermatology Life Quality Index classified according to the effect on patient QoL, representing no effect at all with scores from 0 to one, small effect from 2 to 5, moderate effect from 6 to 10, very large effect from 11 to 20, extremely large effect from 21 to 30.10-12 The patients’ demographic data (age, gender, level of education, marital status, and occupational status) were collected. Furthermore, the characteristics of the disease (vitiligo type, vitiligo stability, and disease duration in years) were recorded. The patients stated the number of affected parts of their body-scalp, face, neck, hands, arms, abdomen, chest, back, genital area, thighs, legs, and feet.
The Institutional Review Board approved this study at the College of Medicine, King Saud University, Riyadh, Saudi Arabia (Research Project No. E-20-4705). All participants signed and submitted their informed written consent.
Statistical analysis
The authors used the IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, N.Y., USA) for analysis. Descriptive statistics (frequencies, percentages, median, range) were used to describe the categorical and quantitative variables. Since the normality test showed the DLQI score median is 4, the range 25, min 0 - max 25, and percentiles 2-8. Skewness 1.342 and Kurtosis 1.6. We used Mann Whitney U and Kruskal-Wallis test to compare the median scores among the various demographic and disease characteristics groups. Also we categorized the DLQI score into <median and >median (%) to conduct Bivariate relationships of each categorical variable with DLQI score groups. This association was examined by the Chi-square test. While the binary logistic regression was applied, in which DLQI score status was taking as the dependent variable and other variables as independent variables. The probability of high DLQI score over the probability of low DLQI score was presented in the form of an odds ratio. A p-value <0.05 and 95% confidence intervals were used to report the statistical significance and precision of the results.
Results
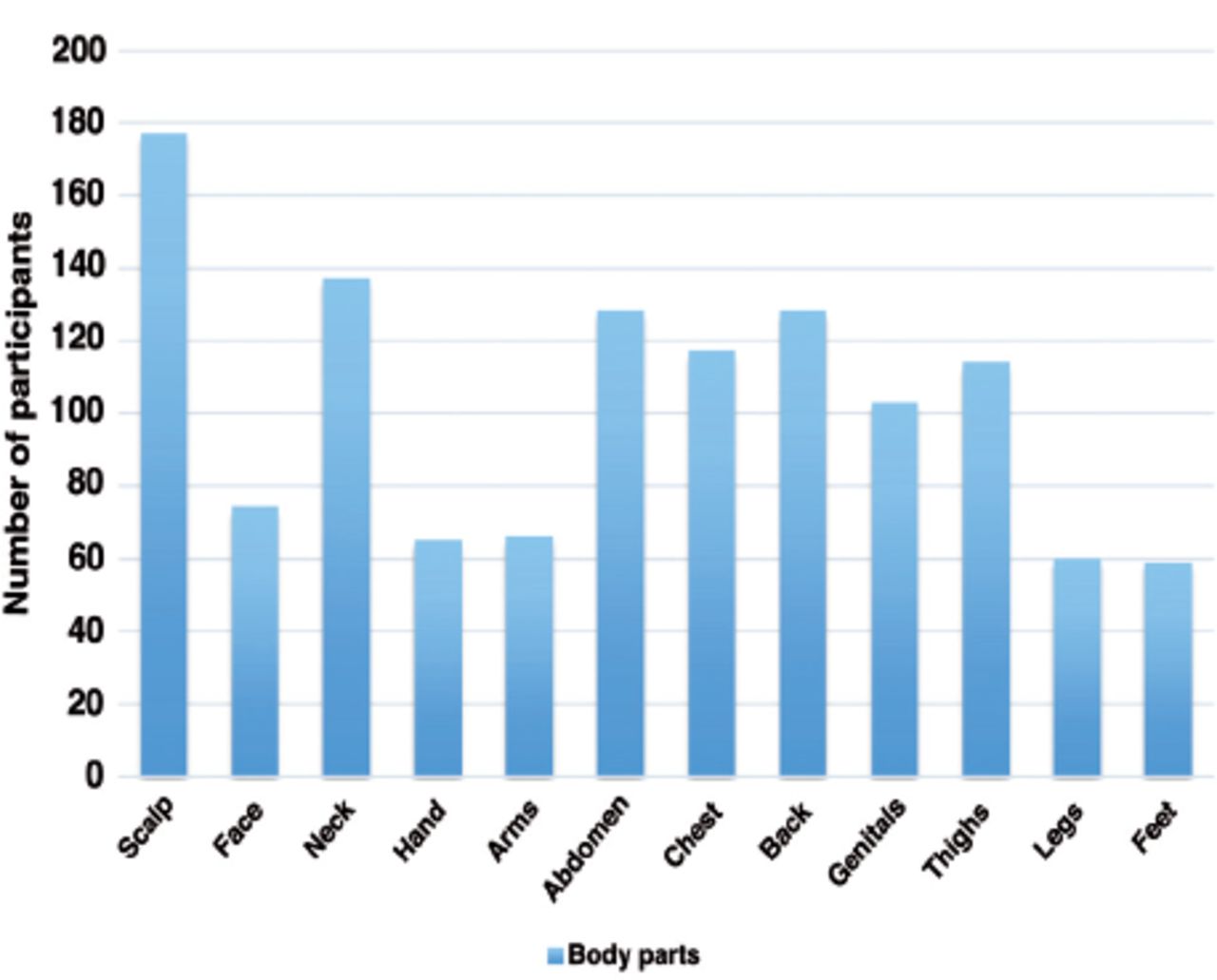
A total of 253 subjects with vitiligo were recruited in the survey. Most of the patients were single (68%) and under 30 years old (62.1%), approximately two-thirds were female (65.6%). Most of the patients had a high educational level (67.6%), and almost two-thirds were employees (34.4%) or students (34.8%). Regarding disease characteristics, most of the patients had non-segmental vitiligo (74.7%), with approximately two-thirds suffering from progressive vitiligo (66.4%). The median and range of the number of affected parts and duration of the disease in years were 7 (4-10) and 9 (4-17), respectively. We used Mann Whitney U and Kruskal-Wallis test to compare the median scores among the various demographic and disease characteristics groups. It was found that married subjects, patients with non-segmental or progressive vitiligo scored higher medians than their counterparts groups p<0.05 (Table 1). Figure 1 illustrates the body parts affected by vitiligo.
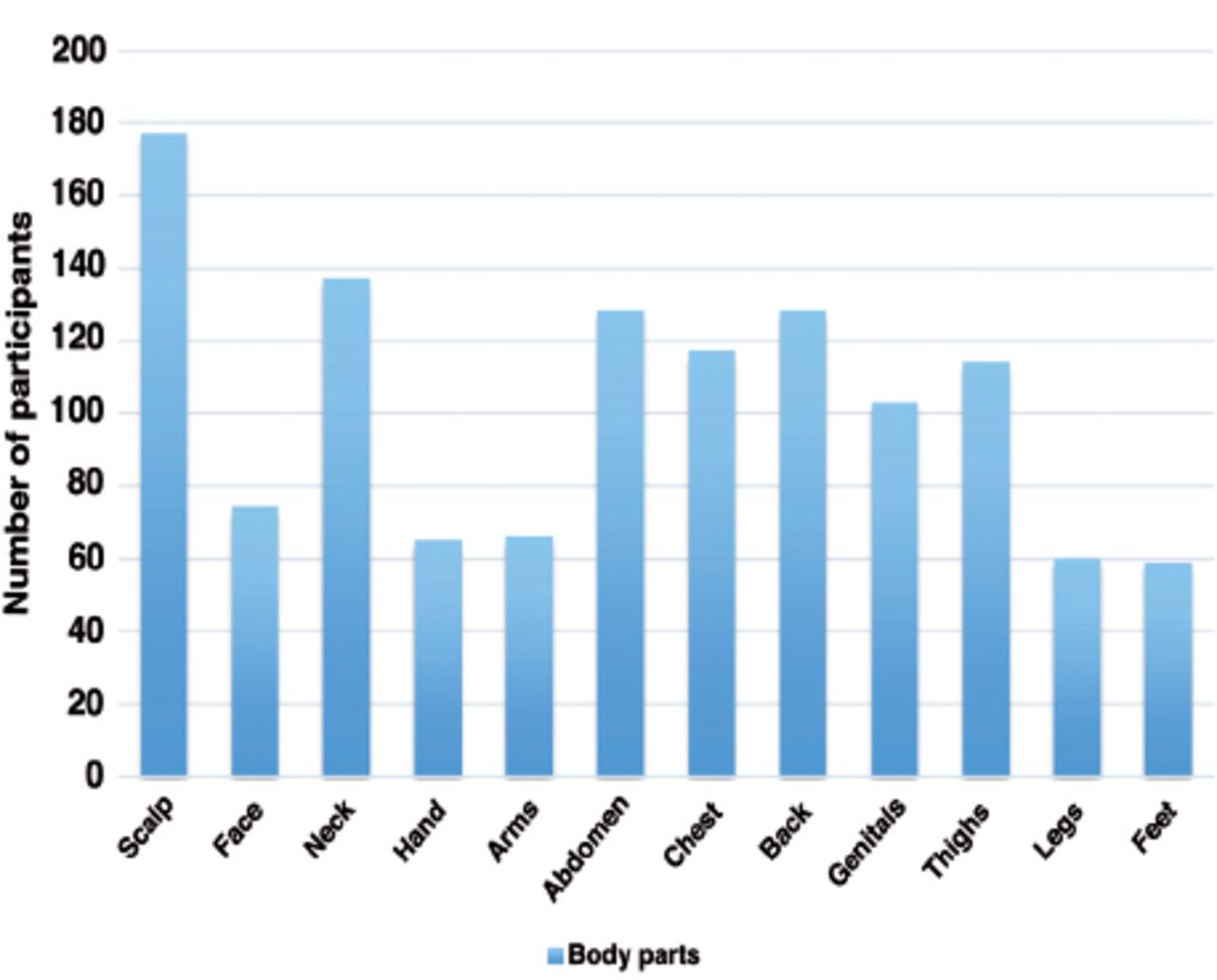
- Body parts affected by vitiligo.
- Demographic data and disease characteristics by median Dermatology Life Quality Index (DLQI) scores (N=253).
Table 2 describes the number and percentage of patients according to vitiligo involved areas and their DLQI score classification. Vitiligo involved areas classified into exposed areas (scalp, face, neck, arms, hands, legs, and feet) and unexposed areas (abdomen, chest, back, genitals, thighs). Approximately 75% patients with face, hand and feet involvement have various impairment effect of DLQI. The highest proportion of patients who have involvement of abdomen 94 (44.1%), chest 85 (39.9%), back 93 (43.7%), genitals 76 (35.7%), and thighs 81 (38%) have no effect on the QoL. The majority of the patients (45.5%) visited their primary dermatologists, one to 2 times in 6 months. However, 22.5% attended their primary dermatologists, 8 times or more.
- Exposed and unexposed and visits and Dermatology Life Quality Index (DLQI).
The DLQI score median was 4, the range 25, min 0 - max 25, and percentiles 2-8. Skewness 1.342 and Kurtosis 1.6. Binary logistic regression: influence of the demographic characteristics, type and stability of vitiligo on the risk of high DLQI scores were presented in Table 3. The median DLQI score was significantly higher in married subjects than singles, the unadjusted OR= 2.29 95%CI: 1.33-3.94 (p<0.01). Furthermore, there was a statistically significant increase in the median DLQI score of non-segmental vitiligo over segmental ones, the unadjusted OR= 2.10, 95%CI: 1.16-3.79, (p<0.01). Also the progressive vitiligo had higher median score than the stable ones, the unadjusted OR= 1.87, 95%CI: 1.09-3.18, (p<0.02). The patients’ age, gender, education level, and occupation failed to predict the DLQI score status (Table 3).
- Binary logistic regression: influence of the demographic characteristics, type and stability of vitiligo on the risk of high Dermatology Life Quality Index (DLQI) scores.
Discussion
The global prevalence of vitiligo ranged from 0.5-2%.2 It is not easy to assert the prevalence of vitiligo in Saudi Arabia since we only found one study from the Eastern province. This study published in 2006 reported the prevalence of vitiligo among female school children as 0.4%, which is lower than the global prevalence.14 Also the prevalence of vitiligo in the surroundings countries varied from 1.49% in Kuwait to 3.55% in Jordan.15,16
As far as we know, a few studies have evaluated the QoL of patients with vitiligo in Saudi Arabia.13,17,18 These studies were conducted at the outpatient clinics of the King Khalid University Hospital; National Center for Vitiligo, Riyadh; and Qassim Medical College clinics, Qassim, Saudi Arabia. Also there were no studies evaluated QoL in patients with vitiligo in the other golf countries. We think that the studies are scarce in this area for a condition that affect patients QoL adversely.
Since most of the published studies internationally used the mean score of the DLQI, we reported the mean score of the DLQI for the sake of comparison with these studies. The mean DLQI score in our study was 5.64 ± 5.2 SD, which indicates a small to moderate effect on patients’ life. This mean score was lower than those in the 2 previous studies (9 ± 6.5 SD and 14.72 ± 5.173 SD) conducted in Saudi Arabia.13,18 Globally, DLQI mean scores ranged from 1.82 to 15 with a total mean DLQI score of 8.2, which indicate a moderate effect.3 However, our finding was higher than the mean scores of other studies conducted in Germany with mean DLQI scores of 4.9, Italy 4.3, and Estonia 4.7.13,18-21 This discrepancy among our study, previous local and international studies could be due to the variation in awareness of vitiligo in the community. Middle Eastern countries tend to have higher DLQI scores compared to European countries, and this variation is likely due to the influence of skin color, amount of disease education, and cultural stigma.22
However, the test of linearity in our study showed that the DLQI score median was 4, the range 25, min 0 - max 25, and percentiles 2-8. Skewness 1.342 and Kurtosis 1.6. So for further analysis of our data, we used the median.
The unadjusted OR (95%CI) showed the median DLQI score was significantly higher in married subjects, non-segmental vitiligo, and progressive vitiligo than their counterparts. However, after adjustment, only married status predicted the high DLQI score. Our finding contradicts a previous study in Saudi Arabia reported that single patients with vitiligo had higher impairment in QOL than married patients.17 This dissimilarity could be due to the difference in the assessment tools used to assess QoL in the 2 studies. More studies assessing the associations of QoL impairment in patients with vitiligo are needed in Saudi Arabia.
We found that the involvement of body parts most exposed, such as face, hands, and feet, has the most adverse effect on the QoL. This finding is compatible with other studies that report high DLQI scores in patients with facial involvement.23,24
Lower QoL in patients with vitiligo is associated with poor mental health and vice versa.25 The prevalence of depression, anxiety, social phobia, and specific phobia were higher in patients with vitiligo than in healthy people.6 In Saudi Arabia, the prevalence of depressive symptoms in vitiligo patients varied from 14% to 54% and anxiety symptoms from 29% to 57%.26,27
For a non-life-threatening disease with significant psychological effects, vitiligo management should focus primarily on improving patients’ QoL.28 There are insufficient data on the role of dermatological and psychological interventions in the improvement of vitiligo patients’ QoL.8 However, it has been shown that cognitive-behavior therapy may help patients to cope with vitiligo and improve their QoL.29
The relatively low QoL among patients of vitiligo in the Middle Eastern countries warrants a study on the effect of psychological interventions in greater depth and possible corporation among dermatologists, psychiatrists, and psychologists for managing vitiligo effectively.
Study limitations
Although, DLQI provides a broad idea of QoL impairment in vitiligo patients, it does not detect subtle distinctions as to how patients with vitiligo handle the overall burden of the disease. The study was conducted in Riyadh and is not generalizable to other regions in the Kingdom of Saudi Arabia.
In conclusion, vitiligo patients in Saudi Arabia have a poorer QoL than vitiligo patients with light-skin in other parts of the world. Therefore, better management modalities to improve patients’ QoL and prevent subsequent mental distress are much needed in Saudi Arabia.
Acknowledgment
We would like to thank Editage (http://app.editage.com/) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 7, 2021.
- Accepted April 7, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.