


Abstract
Malleostapedotomy (MS) is an evolving otology procedure that involves attaching prosthesis to the malleus on one end and the stapes footplate on the other end. It has multiple indications and requires skills and experience. We present 2 cases operated in our center (King Abdullah Ear Specialist Center, Riyadh, Saudi Arabia) in which intraoperative incus injury occurred, and MS was used to reconstruct the ossicular chain with good postoperative outcomes and patient satisfaction. As the procedure was surgically difficult and time consuming, many otologists prefer not to do it. Nevertheless, we believe that all surgeons dealing with stapes surgery should be familiar and gain confidence in performing MS considering that intraoperative incus dislocation is a complication that can happen even with great caution.
Malleostapedotomy (MS), also known as malleovestibulopexy or malleus grip stapedotomy, is an otologic procedure in which the prosthesis is attached to the malleus on one end and the stapes footplate on the other end. This procedure was first introduced by Fisch et al.1,2 Malleostapedotomy is performed mainly in revision cases where the lateral ossicular chain is fixed, for management of advanced tympanosclerosis involving the oval window and for cases of eroded incus.1,2 Like any other surgery, MS has its own challenges including selection of the appropriate prosthesis which will have a significant impact on MS success. In a temporal bone dissection study, they have found that the average distance should be 6.3 mm between the site of MS crimp and stapedotomy site (range: 5.75-7.0 mm).1 Moreover, the surgery itself is practically challenging and requiring skills and experience. The end aural microscopic approach was the technique introduced by Fisch et al,2 although transcanal endoscopic procedure has been mentioned in literature for great visualization of the middle ear.
To date, the MS experience is building up and evolving around the world. Therefore, different approaches and surgical techniques with variable prosthesis materials for different indication have been reported. Nevertheless, many otologists still prefer not to do MS due to its surgical difficulties.
We believe that every surgeon practicing stapes surgery should be familiar with MS as intra operative incus dislocation may occur. In this study, we presented case series that were originally planned as classical stapes surgery but ended up with MS procedure where the decision was made intraoperatively due to iatrogenic trauma to the incus.
Case Report
Case 1
A 26-year-old Saudi Arabian man underwent right tympanoplasty in a peripheral hospital in 2013. He then underwent revision of right tympanoplasty 6 months later in the same center. He presented mainly with decreased hearing on the right ear with no improvement at all after the previous surgery. The reason he decided to come to our center was to address that complaint since he did not prefer to use the hearing aid. He reported no family history of hearing loss, or head trauma. There were no other complaints other than the symptoms of allergic rhinitis.
Clinical findings
On physical examination of the right ear, an antero-inferior dry perforation was seen, while the left tympanic membrane was intact with normal appearance. Tuning fork examination was suggestive of conductive hearing loss on the right ear (Rinne test was negative for the right and positive for the left, and Weber lateralized to the right) and the facial nerve was intact bilaterally. The rest of the physical examination including the head, neck and cranial nerves were unremarkable.
Diagnostic assessment
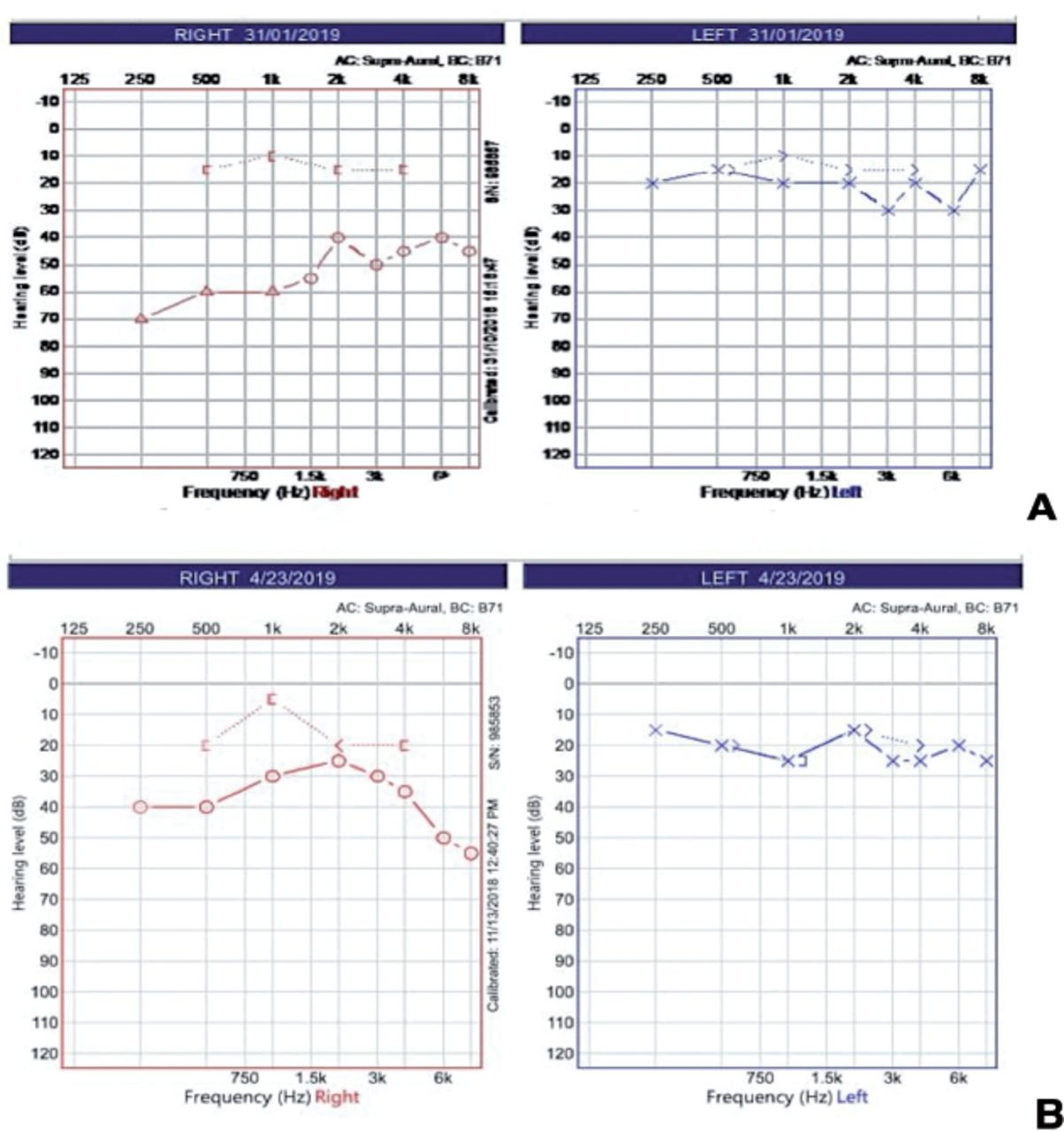
Audiological test was carried out with good reliability as shown in Figure 1A.
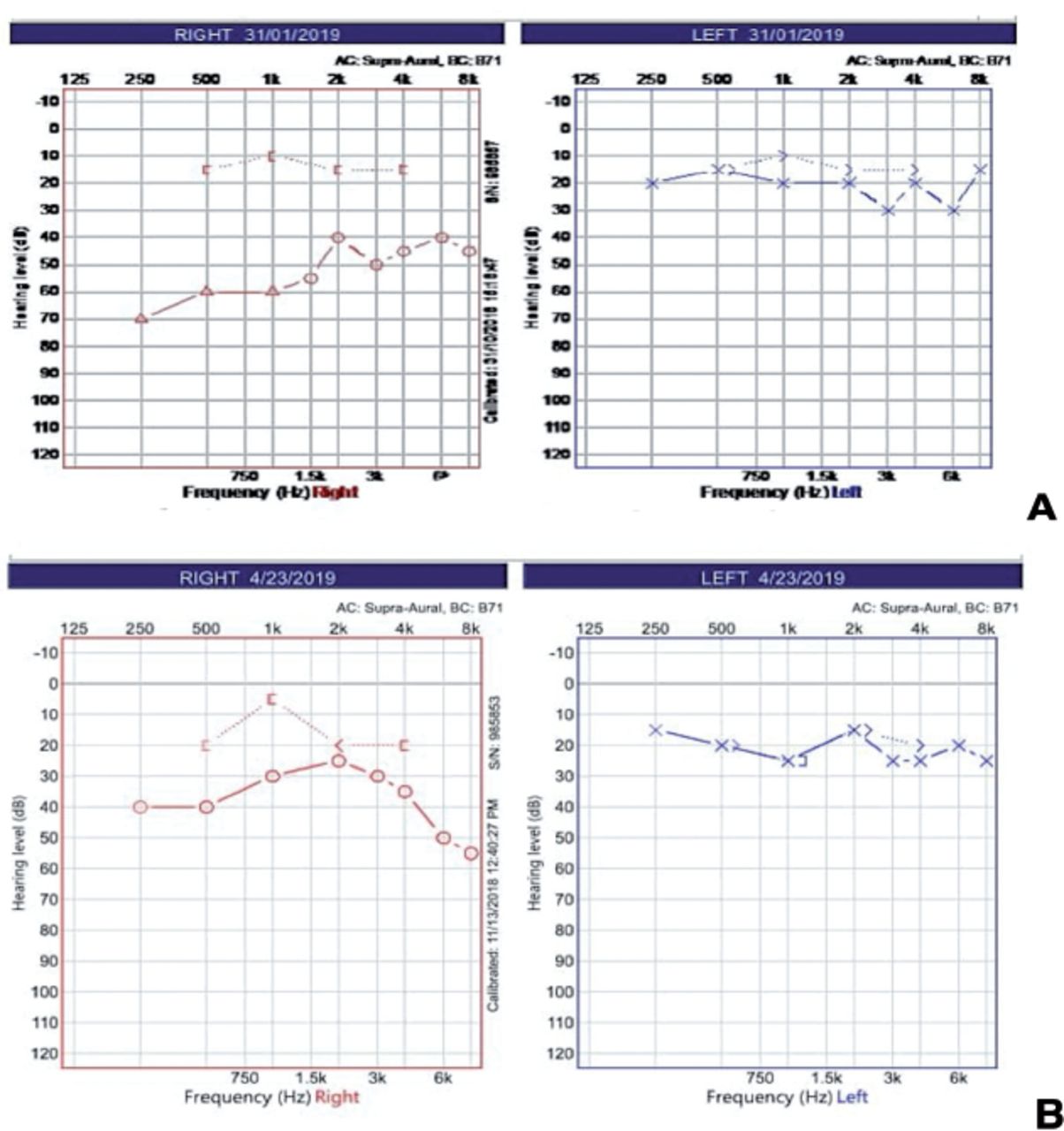
- Audiological test comparing pre and postoperative. A) Pure tone audiometry which was carried out preoperatively showing right hearing with moderately severe up to 2 kHz rising to mild then sloping to moderate conductive hearing loss. Left hearing within the normal level except at 3 kHz with mild hearing loss. The speech reception threshold for right ear was 55 dB HL and 20 dB HL on the left. B) Postoperative pure tone audiometry showing right mild to moderate conductive hearing loss, and the air bone gap improved from 40 dB to 15 dB; hearing in the left side was normal.
Therapeutic intervention
Patient consented for right tympanoplasty and for examination of the right ear with or without ossiculoplasty with post auricular approach. The intraoperative finding was consistent with anterior inferior dry perforation, mobile lateral chain and fixed stapes. At this stage, the primary surgeon decided to do cartilage tympanoplasty and to address the stapes at the same time since the middle ear appeared healthy and also to improve his hearing since it was his main concern.
During the steps for stapes surgery, the incus was dislocated accidently by suction movement. Therefore, tympanoplasty with cartilage graft was performed. We chose to do MS as our second option (Causse LooperativePiston) applied between the handle of malleus and foot plate (below the neck of malleus) and the length between the handle of malleus and foot plate was 6 mm.
Postoperatively, he did well during the hospital stay. There were no vertigo or nystagmus reported and the wound site was clear with no swelling or discharge. Weber test was performed, and the response lateralized to the right ear (operated side); facial nerve was intact. He was discharged home on postoperative day one.
Follow-up and outcomes
Patient was followed up for one month after surgery in our clinic. Hearing improved subjectively without complaints. On examination, the cartilage graft was intact and Weber test lateralized to the right side. Pure tone audiometry performed 2 months postoperatively is shown in Figure 1B. Summarized timeline table of the case shown in Table 1.
- Timeline table for case 1.
Case 2.
A 60-year-old Saudi man with bilateral hearing loss and diagnosed as case of bilateral otosclerosis underwent left stapedotomy in April 2019.
Clinical findings
His ear was examined in our clinic and was within normal range. He was improving postoperatively and requested surgery on the other side as well.
Therapeutic intervention
Seven months after the first surgery, the patient was cleared for right end aural stapedotomy. The diagnosis was confirmed intraoperatively, and the lateral chain was examined and found to be intact. During the surgery, the incus was dislocated accidently; thereafter, intraoperative decision was made to perform MS (using Causse looperativepiston) which was coupled with the handle of malleus, the length was 6 mm and the diameter was 0.4 mm. Then pieces of fascia was inserted around the prosthesis, and the graft was sliced between the tympanic membrane and the prothesis. Postoperatively he did well with no vertigo or nystagmus. The wound site was clear and dry. Weber test showed lateralization to the right ear (operated side), and the facial nerve was intact. He was stable, so he was discharged home in good condition on day one after surgery.
Follow-up and outcomes
During the follow up in otology clinic 4 weeks after surgery, he reported improvement of hearing with no other otological complaint. Examination using microscopic otoscope showed bilaterally intact and normal looking tympanic membrane.
Diagnostic assessment
Pure-tone average (PTA) had good reliability comparing pre and 2 months postoperative in Figure 2. Summarized timeline table of the case shown in Table 2.
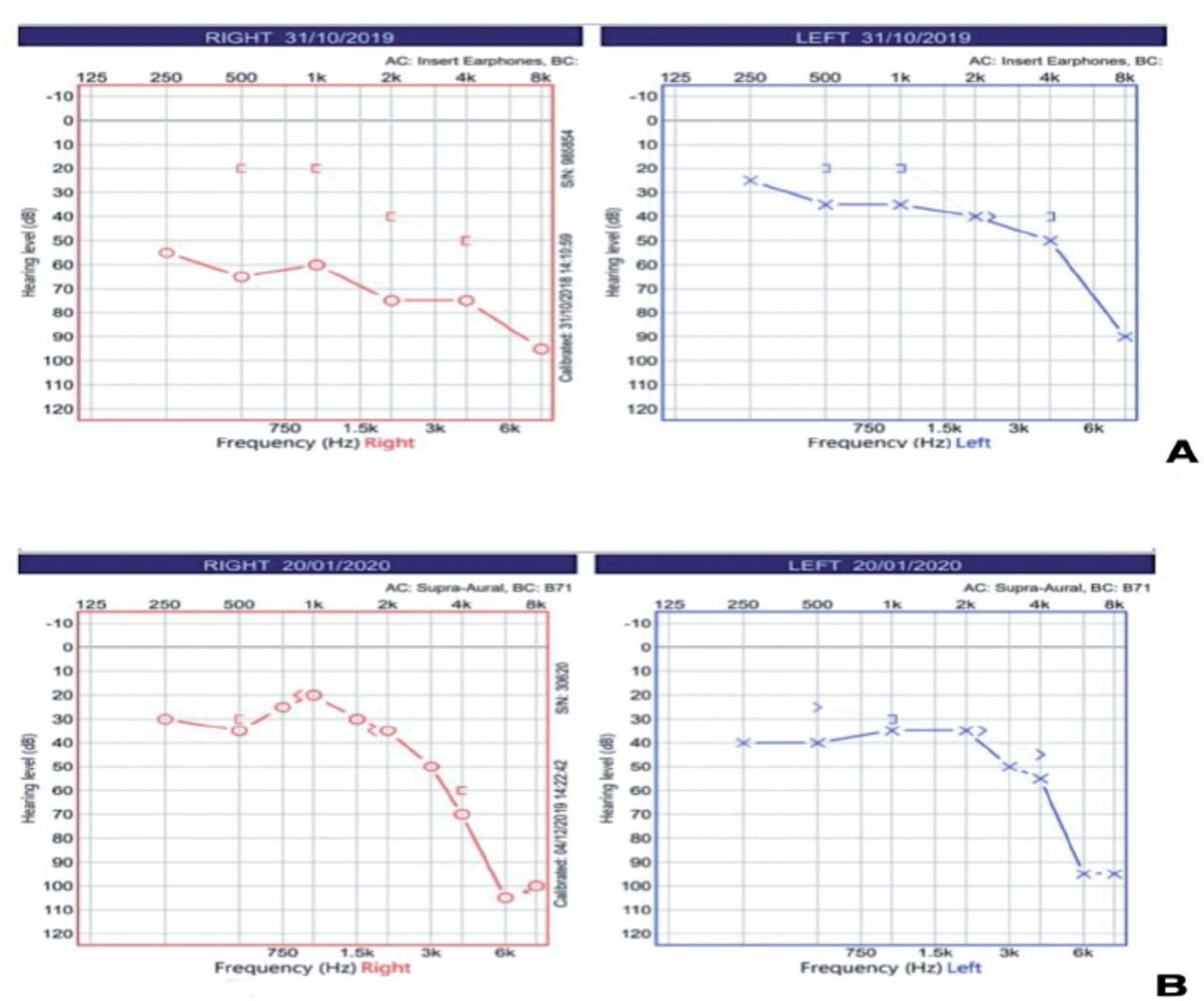
- Audiological test comparing pre and postoperative. A) Preoperative pure tone audiometry showed mild to moderate, up to 3 kHz, slopping to severe mixed hearing loss, and no response at 8 kHz. The left side showed mild to moderate, up to 4 kHz, then slopping to severe mixed hearing loss, and no response at 8 kHz. B) Postoperative pure tone audiometry results showed significant improvement in hearing in right from 250 Hz to 2 kHz with air bone gap improvement from around 40 dB to 0 dB.
- Timeline table for case 2.
Discussion
With this case series, we reported 2 causes of inadvertent intraoperative incus injury resulting to hypermobile incus which was not stable for coupling with the piston prosthesis. The next intraoperative decision made was to choose MS. Interestingly, both patients showed good postoperative audiological outcome. Malleostapedotomy also called as malleus grip stapedectomy or malleovestibulopexy became popular in revision stapes surgery.3,4 Although the main description of MS is in revision surgery, it can also be considered in primary surgery when there are additional pathologies of the incus precluding fixation of a piston such as anomaly or fixation or if incus was accidently subluxated intraoperatively. Even when MS was deemed as a good option for such cases, the surgeons who are used to incus grip may be reluctant to go for MS because of the technical difficulties of the operation. Part of which is related to the difference in the plane of the malleus crimp site and the footplate, hence it cannot be viewed within a single field of focus.1 Furthermore, the shaft of the prosthesis usually has to be bent to allow perpendicular placement of the prosthesis to the stapedotomy fenestra. Another challenge is to choose the appropriate size and type of the prosthesis.
Kwok et al5 in 2009 published a temporal bone study to assess the malleus morphology for the attachment of 3 most commonly used prostheses. They concluded that in order to achieve the appropriate position of the prosthesis to stapedotomy site, individual adaptation should be considered in situ. In our series, the designed MS prosthesis was not available and the options for long and flexible prosthesis guided us to choose the Causse LooperativePiston for both patients. However, it is important to keep in mind the individual approach to choose the proper prosthesis for each case and the concept of “one size fits all” in MS surgery is associated with the risk of improper fit since the distance between crimp site at the malleus and footplate varies in each patient.1,6 Another important point in MS surgery is to choose the proper site for grip in the malleus. Most authors use the handle, but other reports use the neck to reduce the risk of prosthesis displacement or extrusion.7 As in standard incus grip stapes surgery, MS surgery showed favorable outcomes in large percentage of subjects with air bone gap closure to within 10 dB.3 Rambousek et al4 reported an even better hearing outcome for primary MS surgery compared to the revision group. Both of the patients presented in this case series achieved significant hearing improvement postoperatively and had documented audiological improvement comparable to the literature results.
When reviewing the evidence for such cases, we encountered one study discussing intraoperative incus injury.8 They reported that in 15 patients with otosclerosis, the incus was accidentally luxated intraoperatively. One of which dislocated the incus completely, MS was then performed, and auto incus was applied. In the other 14 stapedectomies, although the incus was subluxated, it was held in place by its ligaments hence they did delicate repositioning and piston prosthesis insertion on the long process of the incus.
We believe in reporting the unintentional intraoperative adverse incident to help improve transparency by sharing knowledge and experience. Hence, we reported the use of MS as solution for intraoperative incus injury in patients originally planned as standard stapes surgery. Naturally, the chance of such injury can be minimized with careful approach in each stapes surgery. However, this does not mean that it is totally avoidable. Knowing this in advance can help the surgeon accept and deal with it to achieve the desired hearing outcome.
In conclusion, we believe that all surgeons dealing with stapes surgery should be confident in doing MS in cases of unintentional intraoperative dislocation of incus.
Acknowledgment
The authors gratefully acknowledge King Abdullah Ear Specialist Center, Riyadh, Kingdom of Saudi Arabia for the tremendous support. The authors would also like to acknowledge Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 17, 2020.
- Accepted April 20, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.