


Abstract
Objectives: To measure the effectiveness of tranexamic acid (TXA); in total joint arthroplastyin terms of reducing post-operative blood loss.
Methods: A retrospective cohort study in which patients who had underwent total hip arthroplasty (THA) and TKA between 2010-2018 in a single tertiary center. Those had received TXA (group 1) and those who had received no-TXA (group 2) were evaluated. Unpaired student’s t-test was used to compare TXA and no-TXA groups for continuous variables and Chi-square test was used for categorical variables. A p-value<0.05 was considered significant.
Results: A total of 385 patients were included, 180 patients received TXA, and 205 patients received no-TXA. Post-operative blood loss was significantly less in TXA group (13.41±9.51, p<0.001). Total drainage output was significantly lower in TXA group compared to no-TXA (373.98±246.12 vs. 487.11±307.13 mL, p<0.001). Blood transfusion units were significantly less in TXA group than in the control group (20 units; 11.1% vs. 50 units; 24.4%, p<0.001).
Conclusion: Tranexamic acid use in TKA and THA is effective in reducing post-operative blood loss in terms of drop in Hg level, total drainage output and blood transfusion rate.
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) involve extensive soft and hard tissue manipulation and are associated with significant perioperative and post-operative bleeding that can exceed 1000 mL or approximately 20% of the total blood volume rendering the patient anemic and urgently in need for packed red blood cells (PRBCs) unit transfusion which delays patient’s recovery.1 Different pre-operative and post-operative hemostatic measures have been used to minimize surgical blood loss and limit the need for blood transfusion. Tranexamic acid (TXA) is a synthetic lysine derivative that competitively inhibits 5 binding sites of plasminogen, thus reducing fibrin clot degradation by plasmin.2
Recently, multiple double-blinded, placebo-controlled randomized clinical trials have examined the effectiveness of TXA in minimizing blood loss associated with orthopedic surgery mainly in TKA and THA and demonstrated significant reduction in post-operative blood loss, drainage output volume, and the need for allogenic blood transfusion; and also, reported higher post-operative hemoglobin and hematocrit levels.3 A meta-analysis of 25 randomized controlled trial (RCTs) that examined the safety and efficacy of using TXA in THA summarized the estimated effect size which indicated that topical use of TXA reduced the maximum post-operative Hb drop at approximately 1 g/L.4 Different routes of TXA administration have been utilized. The standard and most used route in clinical practice is pre-operative intravenous infusion of TXA. A randomized clinical trial carried out by Zufferey et al,5 concluded that a single pre-operative bolus of TXA is associated with low blood transfusion rates. One study found that pre-operative administration of IV TXA can confer additional functional benefits, shorter length of hospital stay, greater range of motion and improved earlier mobilization and recovery compared to non-TXA patients who underwent TKA.6
In the Kingdom of Saudi Arabia (KSA), a double blind RCT concluded that prophylactic use of large doses of TXA provides a cost-effective measure in reducing blood loss during and after spinal operations.7 A meta-analysis carried out by Al Jami et al,8 has shown TXA to be effective in reducing blood loss and blood transfusion in idiopathic scoliosis correction surgery. This study aimed to assess and objectively measure the effectiveness of using TXA in total hip and total knee arthroplasty in terms of reducing post-operative blood loss, drainage output, the need for blood transfusion, length of hospital stay and development of clinical anemia.
Methods
This retrospective chart review study was approved by the Institutional Review Board. The study was carried out between January 2018 and December 2019 at King Abdulaziz Medical City, Riyadh, Saudi Arabia. Data was retrieved and accessed through the medical records department.
Inclusion criteria was patients aged over 18 years who had underwent primary or revision unilateral or bilateral THA and TKA between 2010-2018. Participants were divided into 2 groups; those had received pre or post-operative intravenous or intra-articular TXA (group 1) and those who had received no-TXA although it was not contraindicated (group 2). Patients were excluded if they are allergic to TXA, had previous thromboembolic events, coagulopathies and bleeding disorders.
All surgical procedures were performed under either general or spinal anesthesia depending on the anesthesiologist team decision and individual patients’ conditions. In the first group, TXA was administered as intravenous injection of 1-2 mg 5-10 minutes prior to incision and another dose was given at least 60 minutes after the first dose either as 1-2 mg intravenous injection or intraarticular TXA irrigation solution (3 gm of TXA mixed with 100 ml of normal saline) based on the surgeons’ preference and the center’s standards of care. Drainage tube was inserted at the end of the procedure prior to closure using either Hemovac or Jackson-Pratt drain for most patients. Local anesthetic infiltration, prophylactic antibiotics and anticoagulants were given based on each surgeon’s preference. Patients were encouraged to mobilize as early as possible after review of post-operative x-rays; and physical therapy was initiated during the hospital stay. Hematology and chemistry profiles were monitored on daily basis during admission course and packed red blood cells (PRBCs) transfusion was given when hemoglobin (Hg) drops below 70 g/L or 70-100 g/L with symptomatic anemia according to the surgeons’ decision and the hospital criteria of blood transfusion. Once medically stable and able to mobilize, patients were discharged home with appropriate assistive devices and a clear follow up plan. The following variables were recorded by the research team members: demographic variables of patients including age, gender, height, and weight at admission; past medical history including comorbidities such as diabetes mellitus, hypertension, and dyslipidemia recorded at the preoperative assessment visit; surgical details including type of procedure, surgical site, length of the procedure in hours calculated from time of incision to time of closure, and estimated blood loss (EBL), which was measured after subtracting the normal saline irrigation volume in the suction container; pre or post-operative TXA use, route, and dose; post-operative blood loss calculated as drop in Hb and hematocrit (Hct) levels on post-operative day (POD) 1-3 subtracted from the baseline (Hg) level which was measured at the pre-operative assessment visit; total post-operative drainage output volume measured by adding drainage outputs on POD1-3; number of received PRBCs units during admission course and length of hospital stay in days.
Statistical analysis
Statistical analysis was performed using Microsoft Excel. Frequencies and percentages were used to describe categorical variables while mean and standard deviation were used to describe continuous variables. Unpaired student’s t-test was used to compare TXA and no-TXA groups directly for continuous variables and Chi-square test was used for categorical variables. A p-value<0.05 was considered significant. The height and weight of the participants were measured to calculate the body mass index (BMI).
Results
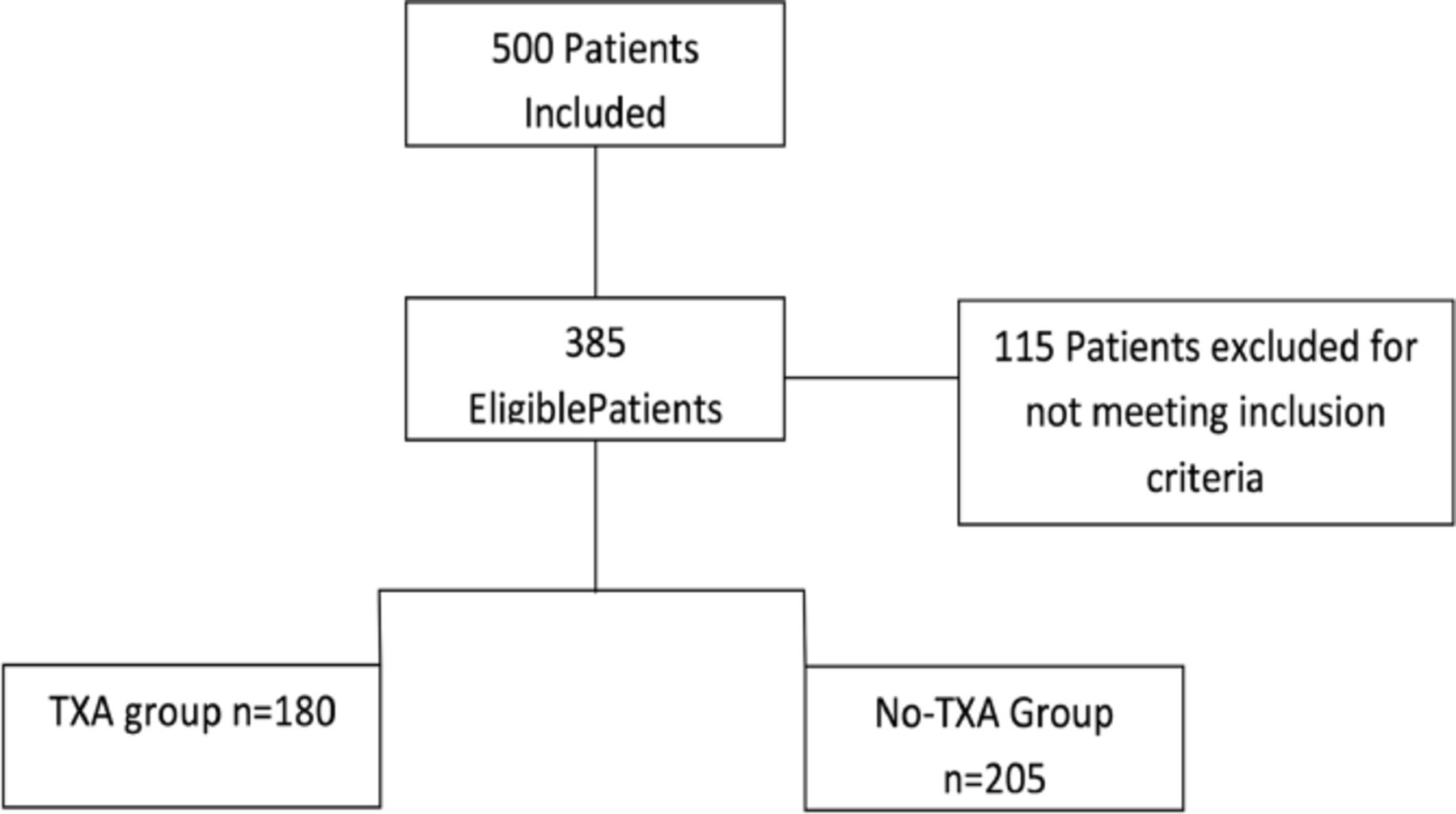
A retrospective chart review of 500 patients underwent elective TKA and THA from 2010-2018 was performed. Out of those patients, 115 patients were excluded for either missing data or not meeting the inclusion criteria. A total of 385 patients were included, of whom 180 patients received intravenous or intra-articular TXA and 205 patients received no-TXA as described in Figure 1. The TXA group comprised 172 primary TKA, 48.3% of them were right sided. The control group included 185 patients who had underwent primary TKA, of whom 47.8% were right sided. Demographic characteristics of the 2 groups are shown in Table 1. No statistical difference was found in mean age or medical comorbidities between the 2 groups (64.5 vs. 66.0 years, p=0.102). Majority of patients were females (81.7% and 65.4%, p<0.001) and BMI was higher than 30 kg/m2 in both TXA and no-TXA groups (35.51±5.68 vs. 33.87±6.49, p=0.008)(Table 1). The mean Hg level of the TXA group was significantly higher compared to the control group on POD-1 (111.43±13.21 vs. 107.53±13.59 g/L, p=0.004) and on POD-2 (100.60±14.91 vs. 95.95±12.48 g/L, p=0.001). Postoperative blood loss measured as drop in Hg from the baseline Hg level was significantly less in TXA group on POD-1 (13.41±9.51, p<0.001). Postoperative total drainage output was significantly lower in TXA group compared to no-TXA (373.98±246.12 vs. 487.11±307.13 mL, p<0.001). Postoperative blood transfusion units were significantly less required in TXA group than in the control group (20 units, 11.1% vs. 50 units, 24.4%, p<0.001). Intraoperative estimated blood loss was similar in both groups (237.22±121.46, vs. 253.17±144.68 mL, p=0.2405) (Table 2). No statistical difference was observed between the 2 groups in terms of duration of surgery (2.92±0.77 vs. 3.00±1.00 hours, p=0.328) and hospital length of stay (10.32±4.67 vs. 11.23±5.12 days, p=0.069) (Table 1).
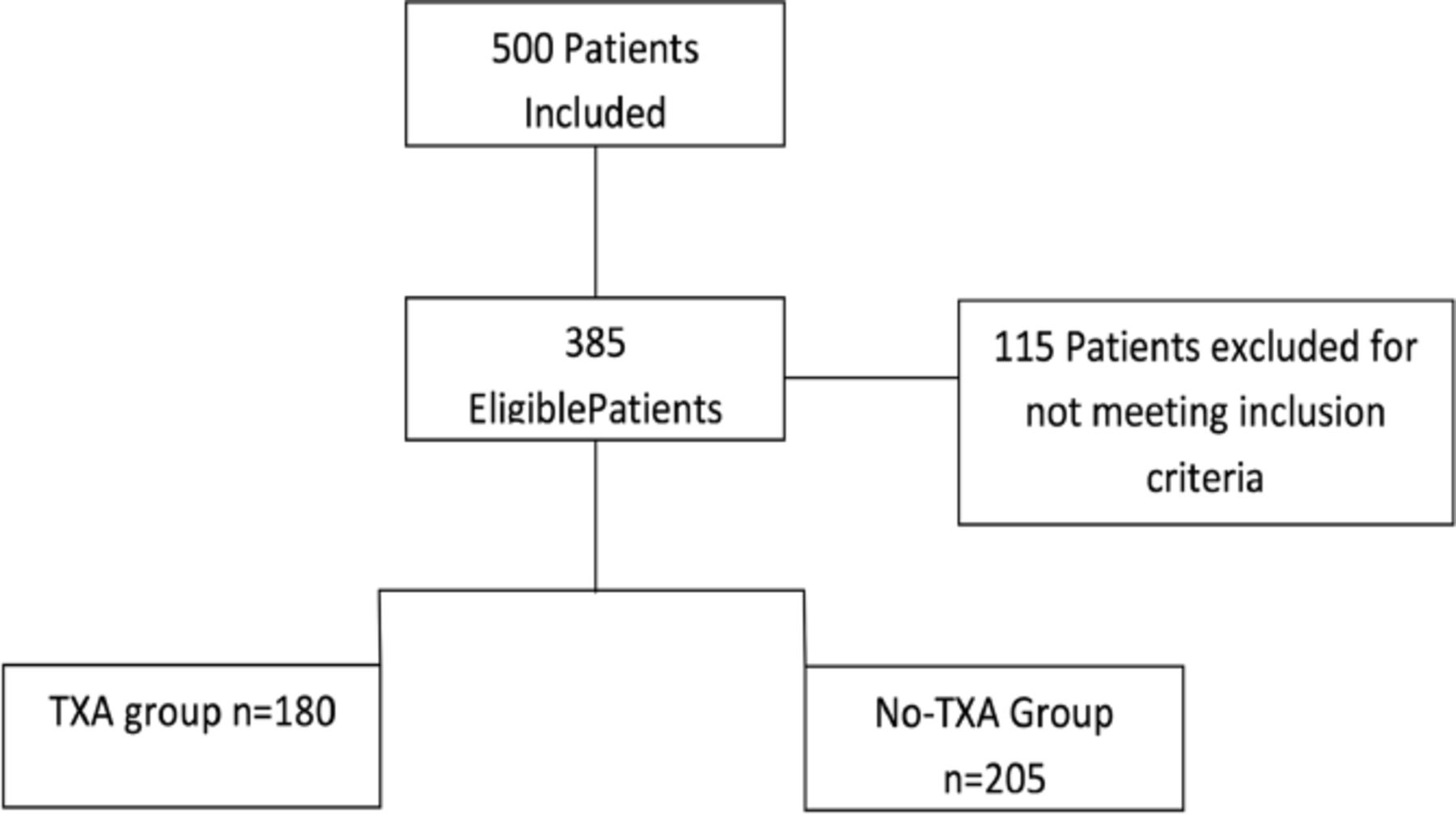
- Flow diagram of included patients. TXA: tranexamic acid
- The frequency distribution of the causes of burns in patients.
- Postoperative blood loss in study cohorts; TXA and No-TXA.
Discussion
Postoperative blood loss comprises a major concern in total joint arthroplasties. Orthopedic surgeons have different enhanced recovery protocols to manage such complications, one of which is using TXA as a hemostatic strategy to reduce bleeding.9 However, a controversy still exists in the efficacy and safety of using TXA in TKA and THA. Some surgeons refrain from using TXA to avoid complications like risk of systemic absorption, increased risk of thromboembolism and development of joint hematoma. Nonetheless, multiple studies have proven that TXA is both safe and effective in controlling bleeding and is associated with significant reduction in postoperative blood loss.10 This study showed consistent data in which the mean postoperative hemoglobin level was higher, and the total drainage output was lower in patients who had received either intravenous or intraarticular TXA.
Different double-blinded randomized clinical trials have investigated the role of TXA in reducing the expected drop in hemoglobin levels and confirmed its efficacy.11,12 In this study, patients who had not received TXA were more likely to develop postoperative clinical anemia, losing up to 17 units of hemoglobin from their baseline level. Data presented in this study showed higher rates of blood transfusion in patients who had not received TXA, supporting existing evidence. A comparative retrospective study be Sandri et al,13 reported significant reduction in blood transfusion rates (65% vs. 37.5%, p=0.011) and lower mean blood volume transfused (450 mL vs. 240 mL, p=0.009) in patients who received TXA. Multiple studies have demonstrated a strong association between TXA use and early ambulation and short hospital length of study.10,14 In this study, majority of patients expected to stay for at least one week post-operative. Moreover, small percentage of the TXA group underwent bilateral or revision total joint arthroplasty (TJA) which required longer admission as well as encouraged early discharge in uncomplicated TJA among the control group.
Study limitations
In this study, TXA use was in accordance with the surgeon’s decision which might be linked to increased likelihood of selection bias. Another limitation was that mean Hg levels were not measured on consecutive days as some patients were discharged earlier and rather recording of any postoperative. Three laboratory results within one week of admission was performed. However, the main goal of this study was to measure early postoperative changes following TXA administration and augment findings of this experience with previously investigated literature.
In conclusion, TXA use in total hip and knee arthroplasty as intravenous or intraarticular administration appears to be effective and recommended to reduce postoperative blood loss in terms of drop in hemoglobin level, total drainage output and the need for blood transfusion.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 2, 2021.
- Accepted June 1, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.