


Abstract
Objectives: To assess the impact of body weight and body mass index (BMI) on pregnancy outcome.
Methods: This prospective cohort study included 3026 pregnant women attending Bakhsh Hospital, Jeddah, Saudi Arabia between July 2017 and June 2019. They were classified according to BMI into normal, overweight, and obese, and were followed up until delivery. The normal group was used as control. Fetal indicators (gestational age at delivery, birth weight, congenital anomalies, Apgar score at 1 and 5 minutes, and admission to neonatal intensive care unit), and maternal indicators (cesarian section, incomplete placental removal, and blood loss volume during labor) were compared between groups.
Results: Prevalence rates of diabetes mellitus and hypertension were higher among overweight and obese women than women with normal BMI (p<0.001). Incidence rates of macrosomia (p=0.002), cesarean sections (p<0.001), incomplete and manual removal of placenta (p<0.011), and >300 ml blood loss (p<0.001) were higher among overweight and obese women than in women with normal BMI.
Conclusion: Overweight and obese pregnant women are at high risk of adverse pregnancy outcomes and need careful periconception, antenatal, in labor, and postpartum care. We also recommend weight control.
Female obesity has become one of the major public health concerns of the past century, due to its growing incidence and impact on pregnancy.1,2 Prevalence of female obesity in 2016 globally according to the World Health Organization was 15.1%.3 Obesity is rapidly increasing in all countries including Saudi Arabia.3 Elevated maternal body mass index (BMI) is associated with numerous adverse pregnancy outcomes such as pre-eclampsia, eclampsia, pre- and post-term birth, labor induction, macrosomia, childhood obesity, cesarean section, and postpartum hemorrhage.4,5
The National Academies Institute of Medicine in the United States proposed in 1990 that maternal weight gain during pregnancy should be based on pre-pregnancy BMI. This was updated in 2009. For women with an underweight BMI (<19.8 kg/m2), a weight gain of 12.5-18 kg was suggested; for women with a normal BMI (19.8-24.9 kg/m2), a weight gain of 11.5-16 kg; for women with an overweight BMI (25.0-29.9 kg/m2), a weight gain of 7-11.5 kg; and finally for women with an obesity BMI (>29.9 kg/m2), a weight gain of 5-9 kg was proposed.6 For many years the literature has advised an individualized approach to nutritional counseling concerning women’s access to food, socioeconomic status, race-ethnicity and cultural food choices, and BMI; although this was geared to uncomplicated pregnancies. Therefore, lifestyle modifications have been recognized as essential for a healthy peripartum period.7 Recently, more evidence on the ‘fetal programming hypothesis’ has improved understanding of the importance of the intrauterine environment in pregnancy continuity and neonatal outcomes. Its subsequent long-term impact on women’s health and offspring development has also been noted.8 In multiple publications, body weight has been identified as one of the core maternal factors influencing the intrauterine environment and its health.9
In this study, we investigate the impact of body weight and BMI on pregnancy course and outcome in patients attending Bakhsh Hospital, Jeddah, Kingdom of Saudi Arabia (KSA).
Methods
This prospective cohort study comprised 3026 pregnant women attending Bakhsh Hospitals in Jeddah, KSA from July 2017 to June 2019. Inclusion criteria included pregnant women aged 16-50 years. Those aged less than 16 and older than 50 years were excluded.
They were classified according to BMI into normal (BMI <25), overweight (BMI 25-29.99) and obese (BMI ≥30) and were followed up until delivery. The normal BMI group was used as control. The fetal indicators were as follows: gestational age at termination of pregnancy, birth weight of the pregnancy outcome, congenital anomalies in the outcome, Apgar score at 1 and 5 minutes, and admission to the neonatal intensive care unit (NICU). The maternal indicators were: cesarian section (C/S), incomplete placental removal, and volume of blood lost during labor. Indicators were compared between normal BMI (<25 kg/m2) and overweight or obese (BMI ≥25 kg/m2) groups.
The study was approved by the Department of Obstetrics and Gynecology in Bakhsh Hospital, and verbal consent was obtained from the patient. Study was carried out according to Helsinki declaration.
Statistical analysis
Data were analyzed using the Statistical Package for Social Sciences Version 21 (IBM Corp., Armonk, N.Y., USA). Categorical variables were presented as numbers and percentages, and compared using the Chi square or Monte Carlo test. Continuous variables before and after pregnancy were presented as means ± standard deviations and were compared using a paired t test. Relative risk was calculated to assess the impact of obesity on pregnancy outcome after classification according to BMI. All tests were 2-tailed, and p<0.05 was considered statistically significant. Correlations were tested using Spearman’s correlations.
Results
Of the women studied, 35.5% were normal, 32.9 overweight and 31.6 were obese (Table 1). The demographic characteristics of the sample are summarized in Table 2. More than half of the participants were in the age groups 26-30 and 31-35 years, with most of them in the normal BMI group (40.8% and 32.4%). Nearly 32% of both age groups were overweight, and 27% and 34% of both age groups respectively were obese. There was a significant difference between the 3 BMI groups (p<0.001). Most participants had been pregnant 2-4 times (gravidity 2-4) and of these 35.9% had a normal BMI, 33% were overweight, and 31% were obese. Nearly 42% of the primigravida had a normal BMI, and 30% were overweight with a significant difference regarding gravidity between the 3 groups (p<0.001). Most participants had delivered 2-4 times previously (parity 2-4), and of these 32% had a normal BMI, 33.5% overweight, 34% were obese. Of the nullipara, 40.7% had a normal BMI, 31% were overweight, and 28% were obese with a significant difference regarding parity between the 3 groups (p<0.001). More than 2/3 of participants had not previously had an abortion, and of these 37.7% had a normal BMI and 31.7% were overweight. Most of those who had previously had an abortion had undergone only one. Of those who, 36% were overweight and 33.7% were obese. Of those who had undergone 2-4 abortions, most were overweight (37.4%) and obese (36.2%) with a significant difference between the 3 groups (p=0.002). Most participants had not previously suffered a stillbirth. Of those who had previous history of stillbirth, 35.5% had a normal BMI, 32.8% were overweight and 31.7% were obese. Of those who had undergone 2-4 stillbirths, 50% were obese, 37.5% were overweight, and 12.5% had a normal BMI, but there was no significant difference between the groups (p=0.841). Most participants did not have any disease, although most participants with medical diseases had diabetes mellitus. Of these with diabetes, 39.3% were overweight, 36% were obese, and 24.6% had a normal BMI. Of those with hypertension, pre-eclampsia, and eclampsia, 59.2% were obese, 22.5% were overweight, and 18.3% had normal BMI, with a significant difference (p<0.001) between the groups (Table 2).
- Prevalence of obesity among participants (N=3026).
- Demographic and medical characteristics of participants according to pre-pregnancy body mass index (N=3026).
The highest mean pre-pregnancy and in labor weights were found in the 36-40 age group (71.47-78.81 kg) and the 41-45 group (75.46-82.08 kg). The largest weight increases were found in the 16-20 age group (13.7%) and the >40 group (13%) and these were statistically significant different in terms of BMI (p<0.001). As regards to stillbirth, the highest increase was in those who had not previously suffered a stillbirth (11.5%), and the difference was statistically significant (p=0.001). The highest pre-pregnancy and in labor weights were found in those who had both DM and hypertension (91.46-96.5 kg), but the highest increase was found in those free of medical diseases (12.4%), with a statistically significant difference (p<0.001) (Table 3).
- Comparison of pre-pregnancy and in labor weight according to sample characteristics (n=3026).
In most participants, birth weight ranged from 2.6 to 3.5 kg. More than 40% of those who had babies with a birth weight < 2.5 kg had a normal BMI; 63% of those whose birth weight was 4.1-4.5 kg were overweight and 80% of those whose birth weight was >4.5 kg were obese. The difference between the 3 groups was significant (p<0.001). Most participants whose babies had a birth weight <3.5 kg had a normal BMI, but most participants where birth weight was >3.5 kg were obese or overweight (p value regarding birth weight <0.001) (Table 4, Figure 1).
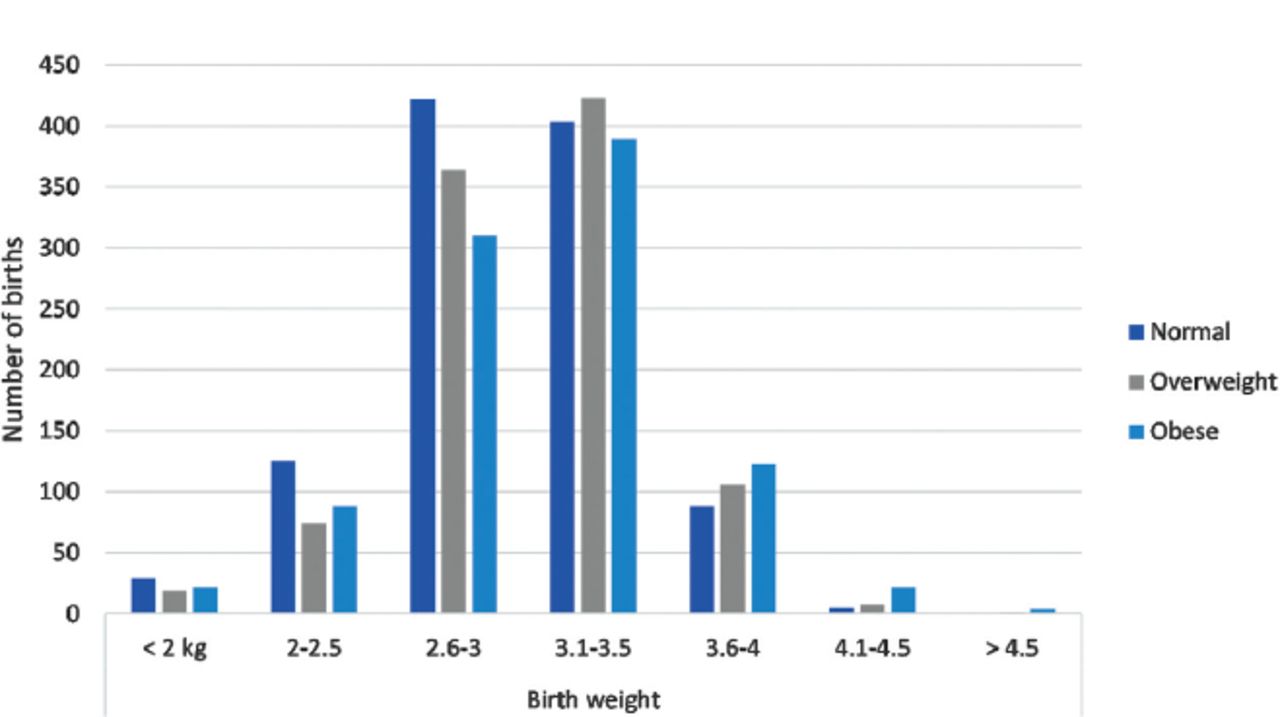
- Birth weight in kg according to body mass index.
- The effect of maternal BMI on the outcome of pregnancy.
There was no significant difference between the 3 groups as regards to gestational age, congenital anomalies, Apgar score at 1 and 5 minutes, or admission to NICU. Of those who delivered vaginally, 42% had a normal BMI. Of those who delivered by elective C/S (41%) and emergency C/S (35%) were obese; and the difference was significant (p<0.001). Of the participants with manual placental removal, 39% were obese and the difference between the 3 BMI groups was significant (p=0.036). Most of those who had a blood loss volume >300 ml were obese, with a significant difference between the 3 BMI groups (p<0.001) (Table 4).
Macrosomia occurred 3.8 times more among overweight and obese pregnant women than in those with a normal BMI (p=0.002). There was no significant result between BMI groups for Apgar score at 1 and 5 minutes. Cesarean sections occurred 1.510 times (CI: 1.366-1.668) more among overweight and obese pregnant women than in those with normal BMI (p<0.001). Incomplete and manual removal of the placenta occurred 1.436 times (CI: 1.082-1.905) more among overweight and obese pregnant women than in those with normal BMI (p=0.011). Blood loss >300 ml occurred 1.499 times (CI: 1.294-1.738) more in overweight and obese pregnant women than in those with normal BMI (p<0.001) (Table 5).
- Relative risk of adverse pregnancy outcome due to obesity.
Discussion
Obesity in women is one of the major public health concerns of the past century due to growing evidence of the negative impact on maternal and fetal outcomes of pregnancy. Our study found similar results to other studies indicating major pregnancy complications due to obesity, including gestational diabetes, hypertension,10 C/S, fetal macrosomia and increased risk of later childhood obesity.1,5 Risks during pregnancy also include stillbirth and congenital anomalies.11,12 This study indicates that the incidence of macrosomic babies increased substantially in obese and overweight women, compared to women with a normal BMI. These results also support a study which suggested that babies from mothers with a higher BMI have higher risks for childhood obesity.13 This long-term impact of maternal body weight has also been supported by another study, which suggested the effect of maternal obesity on offspring health increasing the risk of coronary heart diseases, DM, asthma and childhood obesity.14
The Apgar score is a widely-used indicator of fetal wellbeing. It provides information about the prognosis of neonatal survival especially among preterm infants.15 The present study did not find significant differences in Apgar score at 1 and 5 minutes between groups of obese and overweight women compared to the group of women with normal BMI, unlike the existing literature. For example, 2 studies suggested that children from obese pregnant women had an increased risk of low Apgar scores at 1 and 5 minutes.16,17 Therefore, further research is needed to investigate possible reasons for this disparity.
In addition, one study reported that maternal obesity could increase the risk of infants admitted to NICU.10 Moreover, this study also found Apgar score discrepancies that normalized within 10 minutes of delivery, which suggests a transient decrease in the condition of the neonate at the time of delivery. Increased incidences of fetal acidosis were observed in babies of mothers with morbid obesity compared to babies from non-obese mothers. These complications were suggested to result from conditions such as dysfunctional labor or placental insufficiency, which are more prevalent in obese mothers, as dysfunctional labor or placental insufficiency could increase the rates of fetal acidosis and consequently lower Apgar scores.
Regarding the incidence of C/S, our study suggests that it increases with maternal BMI. There is a statistically significant relationship between maternal BMI and the number of C/S performed, as found by a study of 112,309 women in 2016.18 It concluded that women with a higher BMI than normal also had higher incidences of cesarian delivery, pre-labor cesarean delivery, intrapartum cesarean delivery, cesarean delivery after induction, and cesarean delivery after spontaneous labor. The authors also reported a higher incidence of induction of labor in cases of overweight and obese mothers. Our results also support a previous study which suggests an increased rate of C/S among obese mothers with odds ratio of 2:1.
In our study, incomplete and manual removal of the placenta occurred more among overweight and obese pregnant women than in those with a normal BMI, with a statistically significant difference. Our study also found a significant relationship between maternal BMI and the amount of blood lost during and shortly after delivery. It further supports the current evidence that elevated BMI increases the incidence of postpartum hemorrhage which may differ according to the delivery mode.19 Another study suggest that obese women had higher quantities of blood loss, required more transfused blood units and had more severe morbidity although they had the same management as those with normal BMI.20
However, debate is still ongoing on other such outcomes resulting from pre-pregnancy obesity or obesity occurring throughout pregnancy. Studies described how obesity might predispose for maternal and fetal illnesses either before or during pregnancy.21,22 On contrary, a previous study suggested that pre-pregnancy obesity has a protective effect associated with longer gestation duration and lower risk of preterm or low birth weight.23 Insulin resistance increases during pregnancy especially during the last half of pregnancy. Maternal obesity is one of the factors causing this resistance. However, the causal mechanism is very complex and still not understood completely. If insulin resistance during pregnancy is severe, it may cause short or long term metabolic dysfunction both in the mother and offspring.24
Study limitations
Feeding patterns during pregnancy were not studied, and neither was the knowledge of the sample about the impact of BMI on pregnancy outcomes. The study was carried out in a single tertiary care facility. Results are relevant only to Arab women in Saudi Arabia and those delivering within a tertiary care facility.
In conclusion, overweight and obese pregnant women are at high risk of adverse pregnancy outcomes, such as diabetes mellitus, hypertension, macrosomia, C/S, incomplete and manual removal of the placenta, and high blood loss. They therefore require careful periconception, antenatal, in labor and postpartum care. Obesity in women is one of the few risk factors of adverse pregnancy outcome which is modifiable even before pregnancy, with a noticeable improvement in pregnancy outcome.
This study therefore recommends weight loss before becoming pregnant to improve the health status of the mother and pregnancy outcome. Comprehensive interventions can be carried out to control the obesity epidemic through healthy diet, reducing sedentary life with more exercise and health education about obesity and its impact on maternal health and pregnancy outcome.
Acknowledgment
The author would like to acknowledge all patients included in this study. The author would like to thank Oxford Science Editing for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 17, 2021.
- Accepted September 1, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.