


Abstract
Objectives: To investigate the degree of public awareness, beliefs, and attitudes regarding major depression and available treatment options in the Saudi population.
Methods: A community-based cross-sectional study of 1,188 participants was carried out from March to April 2021 in Ha’il, Saudi Arabia using an online self-administered questionnaire. Using a snowball sampling technique, the authors targeted the Saudi population living in Ha’il region.
Results: Overall, 65.6% of the participants had good awareness regarding depression disorder in total. Of the participants, 72.9% had good awareness regarding general awareness, 85.4% regarding depression symptoms, 12.3% regarding risk factors, and 15.7% regarding treatments. Of the participants, 67.3% believed that depression was caused by lack of faith and 45.5% believed that depression was caused by “the evil eye” or black magic. Of the participants, 56% believed in faith healers as a legitimate treatment approach. Of the participants, 63.9% were willing to work with individuals with depression, 62.7% were willing to establish friendships with them, and 27.9% believed that individuals with depression had weak personalities.
Conclusion: The general population exhibited good general awareness regarding depression and its symptoms, but knowledge of risk factors and treatments was poor. Our findings underscore the need for public educational programs to increase public awareness about the risk factors and treatment options for depression.
Depression is a prevalent illness that affects more than 264 million people worldwide.1 According to the diagnostic and statistical manual 5th edition, major depressive disorder is characterized by low mood, markedly diminished pleasure, feelings of low self-worth or guilt, insomnia or hypersomnia, psychomotor agitation or retardation, loss of energy or fatigue, significant weight loss or altered appetite, recurrent thoughts of death or suicide, and poor concentration.2 Disability-adjusted life years (DALYs) is an assessment employed to measure the burden of diseases by calculating the years of productive life lost due to disability or premature mortality. Mental and addictive disorders cause a considerable burden of disease. Reports have estimated that approximately 162 million DALYs were lost globally due to these disorders in 2016.3 Moreover, depression has a huge contribution towards global disability; it is listed by the World Health Organization (WHO) as the single largest factor.4 In Saudi Arabia, the lifetime prevalence of major depressive disorders (MDD) 6.0%, and it is the third most common mental disorder.5
Although the etiology of depression has not been fully elucidated, various risk factors, including heritability, chronic diseases, unhealthy lifestyle, low socioeconomic status, a small social network, and widowhood, are linked to depressive disorders development.6 Psychosocial interventions, psychotropic medications, including antidepressants, and noninvasive brain stimulation modalities, such as transcranial magnetic stimulation (TMS) and electroconvulsive therapy (ECT), are effective treatment forms for depressive disorders.7 The lack of appropriate and timely treatment may have devastating consequences on patients’ quality of life. Untreated depression is associated with a higher incidence of comorbidities, poor prognosis, delayed improvement among those with concomitant medical conditions, increased suicidal risk, and increased health care costs.8 Despite the existence of effective treatments, the majority of individuals with mental disorders remain untreated.9 In KSA, the probability of receiving treatment for MDD in the previous 12 months was only 10.6% underscoring the need to improve therapeutic accessibility and deployment.10
Knowledge and beliefs are associated with public attitudes toward mental illness and individuals with psychiatric disorders.11 General population beliefs and attitudes toward psychiatric disorders within the Arab community generally arise from a deep belief system that is supplemented by the present and past experiences of the community. The general population could perceive the treatment of psychiatric patients as ineffective, money and time consuming, and even risky.12
Public awareness data can be used to identify factors associated with the probability of seeking mental health care within targeted community groups. These data can be harnessed by healthcare policy makers to determine appropriate interventions. Hence, it is important to assess any gaps in the general population’s awareness, beliefs, and attitudes toward various mental illnesses, their risk factors, and treatment options.
A study conducted in the Al-Jouf region, Northern KSA, found that 73.6% (n=425) participants had poor awareness regarding depression. In addition, the stigma was the most reported barrier that prevents patients from seeking mental health care.13 Another small audit study conducted in Riyadh, regarding the attitude of the Saudi community toward depression disorder revealed that 57.66% of participants (n=137) attribute depression to supernatural powers, and 45.98% believe that antidepressant medication can cause addiction.14
Despite the high prevalence of depression, there is a paucity of studies on public perception regarding depression in KSA. This study aimed to investigate the degree of public awareness, beliefs, and attitudes regarding major depression and available treatment options in Ha’il region.
Methods
A community-based cross-sectional study was carried out from March to April 2021 among the Ha’il community in Saudi Arabia using an electronic questionnaire, which was distributed online by the researchers. Ethical approval was obtained from the Ha’il University Research Ethics Committee (approval number: 42/5/36836). The study was performed in accordance with the principles of the Declaration of Helsinki for studies involving human participants.
Participants who were younger than 18 years old, did not live in Ha’il, Saudi Arabia, were non-Arabic speakers, or worked as health care workers were excluded from this study. Using a snowball sampling technique, the authors targeted Saudi population living in Ha’il region, using their social media networks (WhatsApp and Telegram users), and encouraged their contacts to forward it to their social networks.
To determine the sample size for this study, we used the single population proportion formula. The analysis indicated that the minimum sample size required for this study was 381, with a confidence level of 95% and a margin of error of 5%. In total, 1,521 participants were initially recruited. After the exclusion criteria were applied, the total number of enrolled participants was 1,188.
The questionnaire consisted of 33 questions and comprised the following 3 parts: i) information on participants’ sociodemographic data, including age, gender, marital status, nationality, level of education, occupation, monthly income, place of residence, and whether the participant was a medical worker; ii) assessed participants’ awareness on the symptoms of major depression, risk factors contributing to the occurrence of depression, and different approaches employed in the management of this disorde; iii) questions regarding depression symptoms were adopted from the patient health questionnaire (PHQ)-9, a valid scale with Arabic translation used to screen for depressive symptoms and their severity.15 Participants were requested to describe their individual attitudes toward patients with depression in the third part of the questionnaire. Each question comprised 2 responses: ‘agree’ or ‘disagree’. The Questionnaire was reviewed and approved by 2 psychiatric consultants and tested for both readability and comprehension by 25 participants who were not included in the study.
Informed consent was obtained from participants via the electronic questionnaire. Agreement to complete the anonymized online questionnaire was accepted as willingness to participate in the study. Confidentiality of participants was maintained, as no addresses or names were required.
The literature search method to find prior related research was conducted throughout January 2021. Medline and Scopus literature searches were conducted using the following keywords (awareness or knowledge), depression, and Saudi. These keywords were appropriate terms pertaining to the topic and area with no time frame limit.
Statistical analysis
Data was extracted, revised, coded, and entered using the Statistical Package for Social Sciences for Windows, version 22 (IBM Corp., Armonk, NY, USA). Statistical analysis was performed using 2-tailed tests. A p-value<0.05 was considered significant. For awareness domains, each correct answer within each domain was provided one point. The total sum of discrete scores for each item was calculated. Patients with scores less than 60% of the total score for each domain and overall score were considered to have poor awareness, whereas good awareness was defined as scores of 60% or higher of the total score. Descriptive analysis was performed for all variables based on frequency and percent distribution. Cross tabulation was used to assess the distribution of awareness according to participants’ personal data. Relationships between variables were assessed using the Pearson’s Chi-square test.
Results
A total of 1,188 respondents were enrolled in this study. The mean age of participant was 27.6±10.3 years. Of participants, 624 (52.5%) were females and 723 (60.9%) were single. The sociodemographic data of the study participants is presented in Table 1.
- Sociodemographic data of study participants, Kingdom of Saudi Arabia.
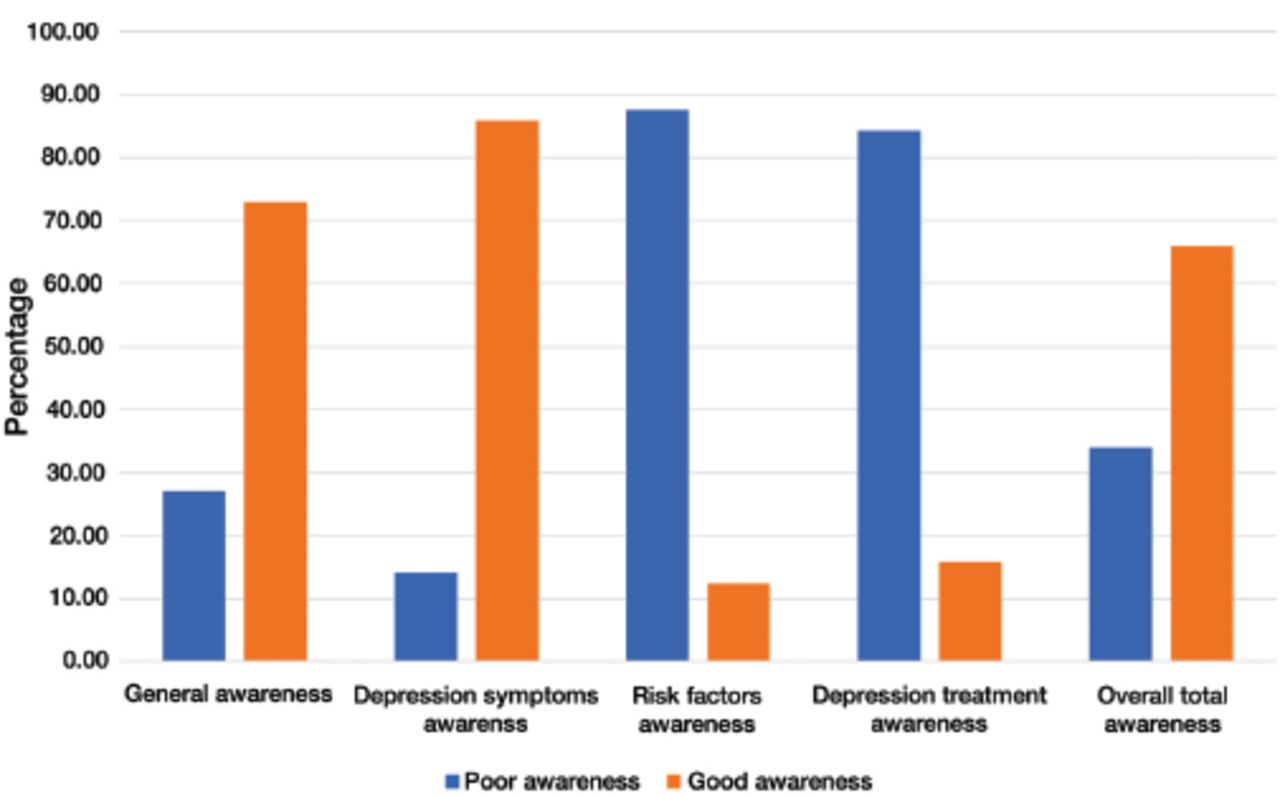
Overall, 65.6% of participants had good awareness regarding depression disorder in total. Of participants, 72.9% had good awareness regarding general awareness, 85.4% regarding depression symptoms, 12.3% of risk factors, and 15.7% regarding treatments (Figure 1).

- Awareness level regarding different aspects of depression among general population in Saudi Arabia.
Of respondents, 96.9% concurred that depression is a treatable illness, 94.3% reported that depressive disorder may affect individuals in different age groups, and 89.4% believed that depression could be regulated by willpower. Regarding awareness of depression symptoms, the most commonly reported symptoms were severe sadness (92.8%), followed by sleep disturbances (insomnia or hypersomnia; 90.2%, Table 2).
- Public awareness regarding depression and depression symptoms in Saudi Arabia.
Concerning risk factors contributing to the development of depression, 67.5% of the participants reported unemployment, followed by lack of faith (67.3%), poverty (57.8%), drug or alcohol abuse (48.7%), and evil eye or black magic (45.5%). Regarding treatments for depression, the most commonly identified approaches were support from family and friends (88.4%), cognitive behavioral therapy (65.0%), faith healers (56.0%), exercise (55.1%), and antidepressants (46.7%) (Table 3).
- Public awareness regarding depression risk factors and treatments in Saudi Arabia.
Attitudes toward depression and individuals with depression among the general population are presented in Table 4. Of participants, 63.9% were willing to work with individuals with depression, 62.7% were willing to form friendships with them, and 27.9% responded that patients with depression had weak personalities. The most reported sources of help for addressing depressive symptoms were self-help (39.6%), followed by family and friends (30.6%), and psychiatrists (24.5%).
- Attitude towards depression and depressed persons among general population in Saudi Arabia.
The distribution of participants’ awareness regarding depression according to demographic data is presented in Table 5. Good awareness was detected in 68.1% of the young age group (<25 years old) and in 53.8% of the old age group (>55 years old), with a significant difference observed between age groups (p=0.049). Further, 68.9% of female participants had good awareness regarding depression, whereas only 62.8% of male participants exhibited good awareness regarding depression, with a significant difference noted between genders (p=0.027). No significant difference in awareness was observed between participants that were university graduates (65.7%) and those with lower educational levels (54.1%; p=0.061).
- Distribution of participants’ awareness regarding depression by their personal data.
Discussion
This study aimed to assess public awareness, beliefs, and attitudes regarding depressive disorder in Ha’il. Limited understanding and erroneous beliefs on mental illness contribute to deep-rooted negative attitudes towards those with mental illness.16,17
The current study demonstrated that 65.6% of participants had good general knowledge regarding depression in total, with the greatest knowledge observed in the area of depression symptoms. In contrast, awareness regarding the risk factors (12.5%) and treatment approaches (15.7%) for depression was low. These findings may be partly underpinned by the relative ease of understanding depression symptoms in contrast to risk factors and treatment modalities that necessitate deeper understanding and changes in cultural beliefs regarding the causes of mental disorders and appropriate treatments. Nevertheless, we identified that general awareness of depression symptoms was higher in the Saudi population than in Nigeria, Bangladesh, Australia, and Canada.18-21 Moreover, the awareness level in our study was higher in the Saudi population living in Al-Jouf region.13 This could be explained by the different methodologies used in our study.
Awareness was significantly higher in young females and those with high educational levels in our study. These results are consistent with previous studies that have assessed the determinants of awareness and attitudes toward mental illnesses.12,22 The significant gender differences may be associated with the lower prevalence of depression in males and consequent lack of exposure to this disorder. A possible factor is also that males may find it more difficult to discuss emotional factors that may limit them opening up on any symptoms they may experience.
Almost half of the respondents in our study believed that “the evil eye” or black magic were causal factors for depression, in accordance with various reports from different Arab countries.13,23,24 These results also agree with the findings from a study of Arab-American muslims that reported that 85.3% of participants believed that depression was a mental disorder, whereas 34.7% of participants reported that “the evil eye” or “black magic” could cause depression.25 Further, a large proportion of Arabs in Australia believe that psychiatric disorders are the result of sin or wrongdoing.26 In contrast, studies in Western societies have indicated that the public generally attributes depression to biological and psychosocial factors.20,21 This illustrates the effect of religion and cultural background on beliefs regarding mental illnesses. Indeed, in non-Western cultures, the causal underpinnings of psychiatric disorders are commonly attributed to the power of supernatural phenomena.27
Majority of the respondents (89%) in this study reported that depression could be controlled by willpower and 67.3% participants believed that lack of faith was a cause for depression. In another study in KSA, 97.8% participants believed that visiting a faith healer was a legitimate treatment option for patients with bipolar disorder.24 A crucial implication of this is that the community members may attribute this mental illness to weakness in personality or religious beliefs. Consequently, this may increase stigma and negatively impact attitudes on seeking mental healthcare. This may at least partly explain the observation that majority of participants (70.6%) stated that they would not seek help from mental health professionals for their depression. In contrast, 82.6% Canadian men reported that they would seek professional help if they developed depression.28
In this study, 88.4% participants reported that family and friends played a key role in the treatment of depression. However, only 30.6% participants stated that they would seek help from loved ones if they were depressed. Indeed, individuals may be more hesitant to discuss mental disorders than physical disorders with relatives and friends.19
An Australian national survey reported that 47.8% of participants regarded taking antidepressants, 50.4% taking vitamins or minerals, 92% performing physical activity, and 44.4% undergoing psychotherapy, as being helpful for treating depression.20 A Canadian survey reported that 62.2% participants regarded taking antidepressants, 60.8% taking vitamins or minerals, 96.5% performing physical activity, and 58.5% undergoing psychotherapy, as being helpful for treating depression.21 Another study carried out in KSA reported that 27% participants regarded taking medications, 4.7% herbal treatments, 33.4% spiritual intervention, and 76% psychotherapy intervention, as being helpful for treating depression.13 In this study, we observed that 46.7% of participants considered taking antidepressants, 35.9% taking vitamins or minerals, 55.1% performing physical activity, and 65% undergoing psychotherapy, as being helpful for treating depression. Our finding shows that the Saudi population has lower awareness of depression treatment modalities (except for psychotherapy) than Australian and Canadian populations.
Only 3.7% of participants believed that ECT could be used to treat depression despite the safety of this approach as a treatment for depression, and it is considered as a gold standard treatment for patients with otherwise treatment-resistant depression.29 These results are similar to those of a study in KSA reporting that only 12.7% of the Saudi population believed that ECT could be used to treat bipolar disorder.24 In this regard, educational interventions have been demonstrated to improve awareness and attitudes toward ECT.29,30 Further, we observed that almost all participants (97.3%) were unaware of TMS. The effect size for TMS is largely beneficial and is recommended for the treatment-resistant or treatment-intolerant patients with depression.31 The poor knowledge of TMS observed in this study may be explained by unfamiliarity to this type of treatment provided the paucity of centers providing such therapy in KSA.
The current study indicated relatively good perception and positive attitudes toward individuals with depression. Of participants, 62.7% reported that they were willing to form friendships and work with individuals with depression, and majority of participants disagreed on the concept of depression being linked to mental retardation. Moreover, approximately a third of participants stated that they would seek help from mental health professionals if they developed depression. In developing countries, mental health services are underutilized due to stigma and beliefs on these conditions as being due to sorcery or spiritual penalty.32 Factors associated with better attitudes toward individuals with psychiatric disorders, mental health services, and improved help-seeking behavior include a weaker effect of traditional beliefs and deeper knowledge on mental disorders.17
Collectively, our findings underscore the need to improve education in the Saudi population regarding depression and increase awareness on the availability and benefits of health services. Our findings emphasize the need for public health initiatives to improve community understanding of depression, especially its causes, treatments, and approaches to care.
Study limitations
This was a cross-sectional study that relied on self-reports. We used the snowball sampling method, which can cause a biased study population. Majority of the study population were young, single, and with higher education. Additionally, respondents may have been more interested in mental health compared to the general population provided that they voluntarily opted to complete the survey. Moreover, the target population included adults living in Ha’il region; therefore, the generalizability of the current findings to the wider Saudi population may be limited. Further studies incorporating larger sample sizes, more variables, and coverage of all regions in Saudi Arabia are warranted to address these limitations.
In conclusion, this study assessed the degree of public perception and attitudes regarding depressive disorders and available treatment options in Ha’il. The general population exhibited positive responses regarding awareness of depression and symptoms; however, awareness of risk factors and treatments was poor. Based on our findings, public educational programs related to depression should focus on increasing public awareness on the risk factors and treatment options for depression. Mental health promotion and educational efforts are warranted to improve mental health literacy and clarify misconceptions regarding depression in the general public. Particularly, these efforts should target older males.
Further studies are required to identify the optimal public interventions to improve knowledge on depression risk factors and treatment.
Acknowledgment
The authors gratefully acknowledge all the individuals who participated in filling the survey of this study. We would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 31, 2021.
- Accepted August 25, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}