


Abstract
Objectives: To determine the prevalence and demographic data regarding incidentally encountered elastofibroma dorsi (EFD) in the Saudi population-based on chest CT (computed tomography) scans.
Methods: This retrospective study was carried out on 4,435 chest CT examinations that were collected between January 2014 and December 2016 in Riyadh, Saudi Arabia. One musculoskeletal radiologist who was unaware of the patients’ clinical presentations or reasons for CT study reviewed the 4,435 chest CTs prospectively, searching for soft tissue tumors in the subscapular region.
Results: Elastofibroma dorsi was incidentally confirmed via CT scan in 36 of the 4,435 patients, including 8 males and 28 females, with a mean age of 76.6 years, yielding a prevalence of 0.8%. Elastofibroma dorsi was more common in females, with a 3.3-fold higher prevalence (77.8%) as compared to males (22.2%); however, this difference was not statistically significant (p>0.05). Twenty-five (69.44%) patients had unilateral EFD and 11 (30.56%) had bilateral EFD. Right-sided EFD was encountered in 60% of females and 50% of males. Furthermore, there was no statistically significant correlation between the size of EFD and the patient’s gender or age (p>0.05).
Conclusion: Elastofibroma dorsi is a rare but uncommon incidental finding on routine chest CT examination encountered in 0.8% of elderly Saudi patients.
Elastofibroma dorsi (EFD) was first described in 1961 by Jarvi et al.1 It is a rare, benign, slow-growing fibrous lesion classically presenting as a painless mass at the inferior pole of the scapula, between the thoracic wall, serratus anterior, and latissimus dorsi muscles. Thus, the term “elastofibroma dorsi” was coined. It is also characterized by spontaneous growth arrest, leading to a prolonged clinical course and frequent asymptomatic cases.1-5 The lesion is usually deep in the serratus anterior and latissimus dorsi muscles. It is often bilateral.2
The exact etiology is unknown, and there is no clear outcome. Thus, ideally, patients usually remain asymptomatic until their EFD reaches a specific size that becomes palpable, visible, and painful. If symptoms are reported, these may include swelling mass, pain, stiffness, scapular snapping, and impingement-like features. According to Brandser et al,4 the prevalence of EFD revealed by computed tomography (CT) is approximately 2%, lower than the 11-24% found in autopsy. There is a female gender predilection (age >50 years), and EFD is infrequent in children.3 The female-to-male ratio is 5:1. The age at diagnosis ranges from 48 to 82 years old, with a mean of 65 years.5 Imaging modalities that used to evaluate the EFD are ultrasound, MRI, and CT scans. Computed tomography is considered the first line investigation and one of the most useful imaging techniques to provide better EFD appearance characterisation and volume measurements.6
There is an information deficit concerning elastofibroma, and most published articles contain limited case reports and case series worldwide. No prior publications were found in the literature discussing the prevalence of EFD in Saudi Arabia generally. This study aims to determine the prevalence of and demographic data regarding asymptomatic patients with EFD in the Saudi population based on CT scan findings.
Methods
This monocentric, retrospective, cross-sectional data collection was carried out at King Fahad Medical City (KFMC), Riyadh, Saudi Arabia. The study approval was obtained Institutional Review Board (IRB H-01-R-012,18-525), and Patients’ data, including gender, age, and images, were retrieved from the standard picture archiving and communication system (PACS). Patients ≥50 years who had had chest CTs between January 2014 and December 2016 were included. Patients <50 years of age, patients complaining of posterolateral chest pain or mass, and patients with a history of chest wall surgeries or previous scapular or chest wall fractures were excluded.
The indications of the obtained chest CT scans were variable, including part of an oncologic staging workup, pulmonary embolism, chest infection, and interstitial lung disease. All patients were scanned with either a GE (64 slices LightSpeed HD), Philips (64 slices Brilliance), or Siemens (128 slices Somatom Definition Flash) CT scanner. The slice thickness varied from 1.5 to 2.5 mm depending on the protocol advised by the assigned radiologist.
A total of 4,435 chest CT scans in ≥50 years were collected. Two thousand eight-hundred thirty-five patients (78%) were scanned post intravenous contrast administration. Nine-hundred seventy-eight (22.1%) scans were performed without contrast administration. Patients were scanned in the supine position with their arms above their heads, except for 47 (1.7%) patients who were unable to place both hands over their heads and were scanned with one or both arms at their sides.
The scans were reviewed by a single musculoskeletal radiologist with more than 8 years of experience in the Musculoskeletal radiology speciality who was unaware of the patients’ clinical presentations and the reasons for scan referral. All studies were reviewed for the presence of a soft-tissue mass in the subscapular region, as well as for the analysis of the mass density as compared to the adjacent muscles; the convexity of the posterolateral margin; and the mass’s depth with regard to the tip of the scapula, serratus anterior, latissimus dorsi, and levator scapulae muscles superficial to the ribs (Figure 1). These CT imaging characteristics were used to diagnose EFD. Furthermore, additional parameters were obtained, such as lesion side, total volume, and contrast enhancement (Figure 2). Information on the patient’s occupation, lifestyle, socioeconomic status, and right or left handedness were not available upon reviewing the patients’ charts.

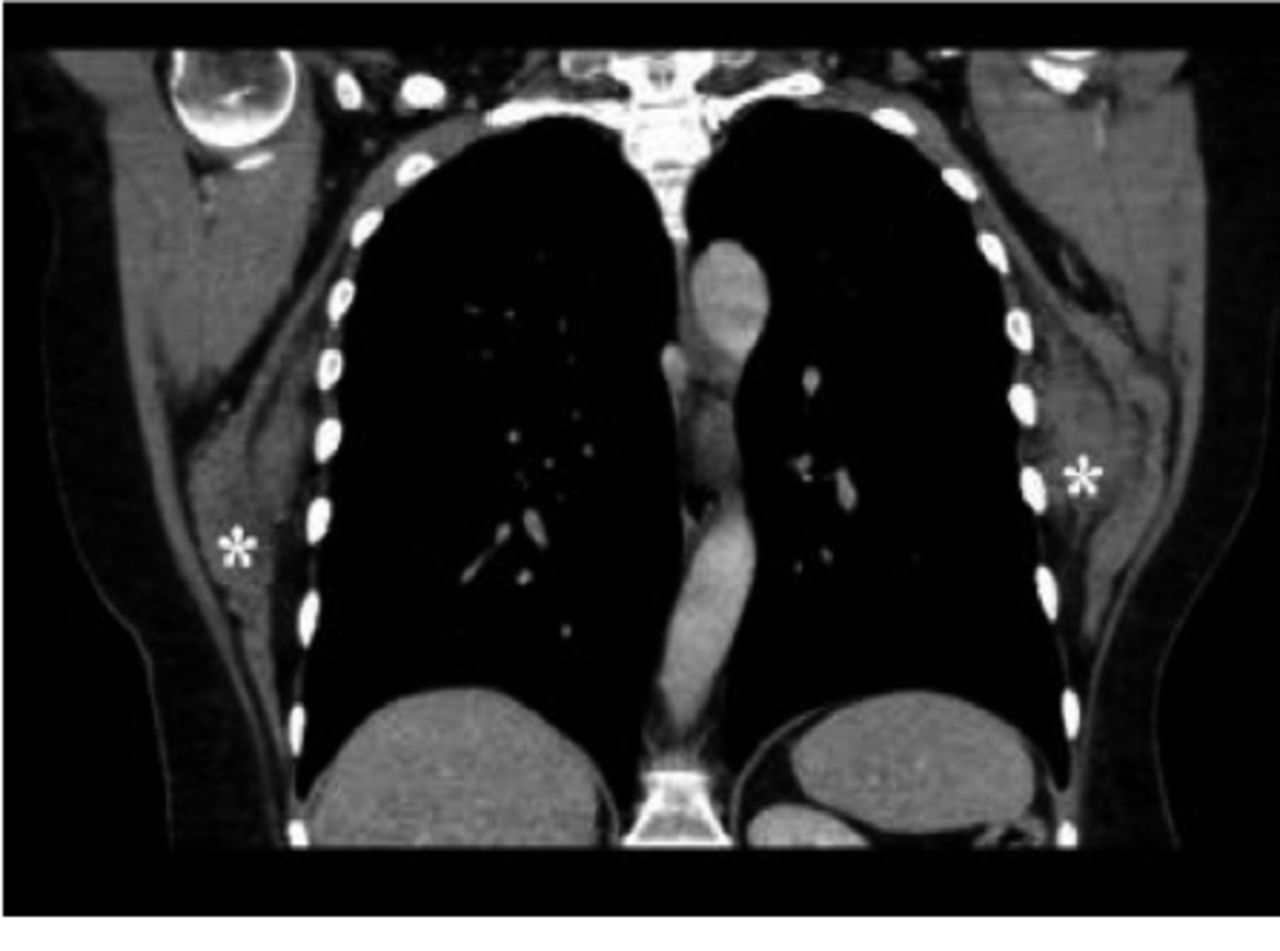
- Coronal contrast-enhanced CT scan of the same patient, demonstrating bilateral EFD (asterisks).

- Axial contrast-enhanced computed tomography scan of the chest of one 69-year-old woman with colon cancer for staging, demonstrating bilateral elastofibroma dorsi. Lesion thickness was taken using the maximum axial dimension (bold white line).
Statistical analysis
All statistical analyses were performed using SPSS Version 27 (Armonk, NY: IBM Corp). Descriptive and inferential statistical analyses were carried out to assess the study variables. Categorical variables were expressed as percentages. Numerical variables were evaluated to ensure the normality of the data distribution using the Kolmogorov-Smirnova and Shapiro Wilk tests. Pearson’s Chi-squared test was performed to assess the relationship between gender and EFD occurrence site. A correlation coefficient was used to determine the linear relationship between the two variables. Pearson’s chi-squared statistic was used for group-to-group comparisons. A p-value of <0.05 indicated a statistically significant difference.
Results
A total of 4,435 chest CT scans were identified in our PACS system during the selected period. The prospective analysis found 36 patients with incidentally encountered EFD, yielding a prevalence of 0.8% (Table 1). Among the patients with EFD, there were eight males and 28 females, with a mean age of 76.6 years. Twenty-five (69.4%) had unilateral EFD, and 11 (30.6%) had bilateral EFD (Table 2). Elastofibroma dorsi on the right side was encountered in 60% of females and 50% of males (Table 2). It appears that EFD was more frequently seen on the right side in most of the positive cases. Elastofibroma dorsi was present more in patients above 60 (Table 3). Statistically, this was significant, with a p=0.002 (Table 4). Our analysis revealed that EFD was more common in females, who had a 3.3-fold higher prevalence (0.6%) as compared to males, which was not statistically significant (p>0.05) (Table 1).
- Descriptive statistics.
- Correlation between elastofibroma dorsi site and gender.
- Relationship between age and side of occurrence.
Values are presented as number and percentage (%).
- Relationship between elastofibroma dorsi (EFD) volume and other characteristics.
Concerning total EFD volume, there was no statistically significant correlation between the size of EFD and the patient’s gender or age (p>0.05) (Table 4). Elastofibroma dorsi had characteristic imaging appearance and location on CT scan, demonstrating homogenous attenuation, similarity to the adjacent muscles, a convex posterolateral margin, and a deep relationship with the tip of the scapula.
Discussion
Elastofibroma dorsi is a benign pseudotumor and non-neoplastic proliferative lesion that is commonly seen incidentally in elderly people.7,8 Several studies have reported that EFD is mostly found in the posterolateral chest wall, in relation to the inferior scapular tip, between the serratus anterior and latissimus dorsi muscle.7-9 It has also been reported that EFD can be seen in other parts of the body, such as the elbow, hand, foot, ischial tuberosity, and olecranon.10,12
This study was conducted in Saudi Arabia, enrolling 4,435 patients above the age of 50, which is considered a large series case in the literature. The calculated prevalence of EFD was 0.8%, with female predominance, and around 70% of the cases were located unilaterally.
Most of the cases reported in the literature were single cases or small case series.13-15 Tepe et al16 published a study including the largest population series in the literature, which was undertaken in Turkey on 4,074 patients, with a prevalence of 2.73% and a female predilection; of these, 54 (48.6%) patients had unilateral lesions, and 57 (51.4%) patients had bilateral lesions.
In our study, the prevalence of asymptomatic EFD among the Saudi population older than 50 years was found to be lower than that reported in the literature. The overall prevalence of radiologically encountered EFD in the literature was around 2%.4-7,17 Hence, genetic and constitutional factors may also contribute to a high prevalence of elastofibroma. Elastofibroma dorsi have been reported in certain populations or families, therefore genetics may play a role in its pathogenesis and etiology. Nagamine et al17 mentioned that 55 out of 170 clinicopathologically proven EFD cases had been found in the same family lines, suggesting a positive family history (16). However, in autopsies, classical elastofibroma dorsi were found in 11.2% of men and 24.4% of women according to Järvi et al.1
The location of EFD and their predominance among older age groups are unlikely to be related to a neoplastic process, as previously thought; rather, a reactive process secondary to the friction of the scapula against the underlying ribs is likely involved.1,12
The reactive process combines hyperplasia and the degeneration of collagen fibers, followed by the overproduction of immature elastic tissue by the fibroblasts.18,19
Unilateral EFD is reportedly more common than bilateral disease and is predominately on the right side.5,20-22 This is compatible with the results of our study, in which EFD was encountered unilaterally and more frequently on the right side.
In the current study, the largest volume size for EFD was located on the right side among females, and this was statistically significant. Elastofibroma dorsi was thought to be the result of a reactive process due to the repetitive mechanical friction of the soft tissue between the scapula and the ribs on the patient’s dominant side.5 However, the relationships between patients’ right or left-handedness, occupation, lifestyle, and disease location and side were not well understood in the literature.23 Therefore, further prospective studies are required to prove or dispute this hypothesis. The current study could not find any significant statistical correlation between the size of the lesion and the age or gender of the patient.
On CT scan, EFD appears as homogenous masses, demonstrating a similar density to that of the adjacent muscles, with interspersed fat streaks that are seated in the subscapular region of the posterolateral chest wall.20,22 The lesion does not demonstrate enhancement upon enhanced CT studies.22
Study limitations
Its retrospective design hampered us in requesting additional and detailed information regarding the patients’ dominant handedness, occupation, or lifestyle for further analysis in relation to the EFD side. Another limitation is the lack of pathological confirmation of the diagnosis due to the study’s retrospective nature. However, such benign lesions do not necessitate systematic biopsy. Lastly, our data collection was based on a single tertiary care center in one region of Saudi Arabia. Thus, to generalize the result of this study, collecting more data from different centers is recommended.
In conclusion, in this largest series of EFD in the literature among the Saudi population, we revealed the prevalence of EFD, along with a literature review. Elastofibroma dorsi is a rarely reported yet not uncommon incidental finding upon routine chest CT examinations, being encountered in 0.8% of elderly Saudi patients. Our calculated prevalence of incidentally detected EFD via CT scan was lower than that reported in the literature, as well as the autopsy series. This will contribute to the improved detection and characterization of posterolateral chest wall masses in patients and the avoidance of unnecessary interventions.
Acknowledgment
The authors gratefully acknowledge Scribendi (www.scribendi.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 1, 2021.
- Accepted December 26, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.