


Abstract
Objectives: To evaluated obesity-related morbidity prevalence among overweight/obese children and adolescents in Saudi Arabia, adiposity indicators and insulin resistance as obesity-related morbidity predictors.
Methods: We enrolled 318 overweight/obese children attending a Pediatric Endocrinology Clinic at King Abdulaziz University Hospital, Saudi Arabia, aged 2–20 years in this retrospective cross-sectional study from September 2019 to March 2021. All children had nutritional obesity, and their body mass index (BMI) standard deviation score was higher than one standard deviation score above the mean for their age and gender. Clinical adiposity indices including BMI, waist circumference (WC), waist-hip ratio (WHR), and bioimpedance analysis (BIA) of body composition were assessed. Biochemical testing of insulin resistance through homeostasis model assessment for insulin resistance and fasting insulin was performed, along with receiver operating curve analysis to obtain optimal cut-off points for obesity-related morbidity.
Results: Obesity related morbidity was found in 61.9%, whereas insulin resistance was detected among 64.7% of the patients. Body mass index standard deviation score, WC, BAI of body composition-derived body fat, homeostasis model assessment for insulin resistance, and fasting insulin are significant obesity-related morbidity predictors, and the cut-off points were established.
Conclusion: Obesity-related morbidity is widely prevalent among obese children and insulin resistance is a key factor in its prediction. Clinical adiposity indices, given their accuracy and practicability, are important predictors of obesity-related morbidity.
Childhood overweight/obesity is considered a universal health issue that reached epidemic proportions; also, it can be a predictor of insulin resistance (IR).1 Definition of overweight and obesity by world Health Organization (WHO) is having a body mass index (BMI) higher than 1 and 2 standard score (SDS) above the mean, respectively.2 In Saudi Arabia, the problem is expanding at an alarming rate, and in 2020 the prevalence of overweight among school children was approximately 7.1% and 14.4% prevalence of obesity.3 Obese children may become obese adults with a steadily rising developing risk of obesity-related morbidity (ORM) throughout their lives, like hypertension, type 2 diabetes mellitus (T2DM), hepatic steatosis and dyslipidemia.4 Although determinants of ORM incidence in children are under research, visceral adiposity (VA) contribution to prediabetes and T2DM risk in adolescence has been highlighted.5 Insulin resistance association and prevalence in pediatric obesity has been evaluated.6 Researchers concluded that IR is an important ORM determinant.7
This study aimed to establish ORM prevalence among overweight/obese children and adolescents living in Saudi Arabia, whether clinical and biochemical indicators of adiposity and IR could predict ORM in these patients, and the cut-off points of these indices for ORM prediction.
Methods
A retrospective cross-sectional study was performed on 318 children and adolescents who were overweight or obese at the Pediatric Endocrinology Clinic at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, from September 2019 to March 2021. Following the clinic visit, the patients and their guardian were asked to contribute to this study,and they signed an informed consent form.
Overweight/obese patients whose ages are between 2 and 20 years, (46.9% females and 53.1% males) were enrolled in this study. All of them had a BMI SDS one SD above the mean for their age and gender, according to the WHO definition.2 The calculation of BMI was according to the Quetelet index8 as follows: body weight (kg)/height (m2). All patients had a nutritional type of obesity. Obese children with monogenic obesity, syndromic obesity, endocrinal dysfunction mainly as hypothyroidism, pseudohypoparathyroidism, growth hormone deficiency, or Cushing syndrome; patients on medications including prolonged courses of steroids, antihypertensives, tricyclic antidepressants, sulfonylurea, or those with inadequate data in their electronic medical records were excluded from the study.
Prior to the start of this study, an ethical approval was obtain from the Institutional Review Committee of King Abdulaziz University Hospital under the reference No:184-16, which included permission for reviewing electronic medical files, taking history, and conducting a physical examination. Patients’ confidentiality was protected following the standards of Helsinki’s declaration.
Blood pressure (BP) were measured and plotting of diastolic BP (DBP) and systolic BP (SBP) was carried out on the Centers for Disease Control and Prevention age-gender-specific charts. Patients who have BP greater than or equal the 95th percentile were considered hypertensive, whereas patients whose BP pressure were >90th and <95th percentile were considered as prehypertensive.9 Acanthosis nigricans was also one of the clinical parameters of IR in the participants.
Waist circumference (WC) and waist-hip ratio (WHR) measurements were taken. The lowest circumference between the iliac crest and the lower costal margin was assessed in centimeters with a flexible tape to the nearest 0.1 cm, while standing in light clothes and plotted on the WC percentile. The WHR was computed after estimating the hip circumference at the point of maximal extension.10 Multi-frequency bioimpedance analysis (BIA) technology was used to determine total body fat percentage (TBF%) and visceral fat level (VF),11 using an ‘InBody 270’ device that is capable of abdominal fat direct measurement at the frequencies of 20 and 100 kHz. The curves for TBF% were then used.12
Insulin resistance biochemical indices
Following a 10- to 12-hour overnight fast, the specimens of the blood were taken. The glucose oxidase method was used to assess fasting plasma glucose (FPG) levels by a glucose analyzer (Yellow Springs Instrument Co., Yellow Springs, Ohio, USA). To estimate fasting insulin (FI), the human-specific insulin radioimmunoassay kit (catalogue no. HI-14 K; Linco/Millipore, St. Charles, MO, USA) was utilized. Colorimetry (Hitachi automatic analyzer 7600-210, Hitachi, Ltd., Tokyo, Japan) was used to determine the levels of triglyceride (TG) (mg/dL), and high-density lipoprotein cholesterol (HDL-C) (mg/dL) and total cholesterol (TC) (mg/dl). The Fried Ewald formula: (TC - HDL-C - TG/5 in mg/dL) was used to calculate the level of low-density lipoprotein cholesterol.13 High-performance liquid chromatography (Tosoh Medics, Inc., San Francisco, CA) was used to measure the percent of glycated hemoglobin (HbA1C%).14
Hyperinsulinism was established with an FI level >17 mIU/L (3-17 mIU/L). The calculation of hemostasis model for IR (HOMA-IR) was carried out as follows: FPG (mmol/L) × fasting serum insulin (mU/L) divided by 22.5. Regarding IR diagnosis, a cut-off point of 3.16 was used.15
Biochemical assessment of ORM. Prediabetes/diabetes state
Hemoglobin A1C (HbA1C) and FPG levels were used to diagnose prediabetes and diabetes, prediabetes was recognized when HbA1C was 5.7-6.4% or FPG level was 5.6-6.7 mmol/L, whereas diabetes was diagnosed when HbA1C was 6.5% or FPG level was ≥7 mmol/L.16
The following cut-off points were used to define abnormal lipid profiles (dyslipidemia): TG levels greater than 130 mg/dL, TC concentrations >200 mg/dL, LDL >130 mg/dL, or HDL concentrations <40 mg/d. For children aged 0-9 and 10-20 years, TG levels of 100 and 130 mg/dL were considered above the 95th percentile, respectively.17
Vitamin D level abnormalities
The deficiency of vitamin D was defined as 25-hydroxy vitamin D [25(OH)D] concentration <20 ng/mL, insufficiency was considered at a concentration of 21-29 ng/mL, and sufficiency was regarded at 30-100 ng/mL concentration. An automated chemiluminescence immunoassay was used for evaluating serum concentrations of 25(OH)D (DiaSorin Liaison, Stillwater, MN, USA).18
Statistical analysis
The sample size was estimated using Power Analysis and Sample Size Software, version 15 (NCSS LLC Company, Kaysville, USA), with the type-1 error (α) set to 0.05 and the confidence interval width set to 0.07 (margin of error 3.5%). Type 2DM was found in 9.4% of children with overweight and obesity in a previous report by Al-Agha et al.4 Based on these figures, a minimum sample size of 268 cases was calculated. However, we included 318. Statistical analyses were carried out by SPSS, version 26 (IBM Corp., Armonk, NY, USA). Data with abnormal distributions presented as medians (interquartile range), and data with normal distributions were shown as mean ± SD. Mann-Whitney and non-parametric Kruskal-Wallis tests were utilized to compare the percentage and frequency of categorical data among quantitative variables. The Chi-square test was utilized to compare categorical data. When the expected frequency was <5, the exact test was carried out. Receiver operating characteristic (ROC) analysis and computation of the area under the curve (AUC) were used to identify the cut-off points of adiposity indices and IR for ORM prediction (pre/hypertension, pre/diabetes, dyslipidemia, and vitamin D deficiency). Sensitivity was defined as true positive rate=true positive measurements/all positive cases, representing the ability to diagnose children with ORM and specificity (true negative rate=true negative measurements/all negative cases), reflecting the ability to exclude morbidity. The relationship between the adiposity indices and IR with age, BP, and the results of laboratory tests were analyzed by calculation of Pearson correlation coefficients. All p-values were 2-tailed, and statistical significance was set at p-value of <0.05.
Results
The lists the biochemical and clinical properties of the individuals as shown in Table 1. In population of the study, 37% were overweight while the remaining were obese, and 64.7% exhibited IR, as indicated by high HOMA-IR values. Besides, 180 (61.9%) patients had morbidities distributed as follows: prehypertension (25.8%), hypertension (15.8%), prediabetes (31.1%), T2DM (6.8%), dyslipidemia (32.5%), vitamin D insufficiency (23.2%), and deficiency (31.5%). Children with ORM exhibited significantly higher BMI SDS (p<0.001), WC (p=0.001), WT SDS (p<0.001), VF (p=0.018), TBF% (p=0.004), FI (p=0.001), and HOMA-IR (p<0.001).
- Clinical and biochemical characteristics.
Diagnostic ability of the adiposity indices and IR to predict morbidity
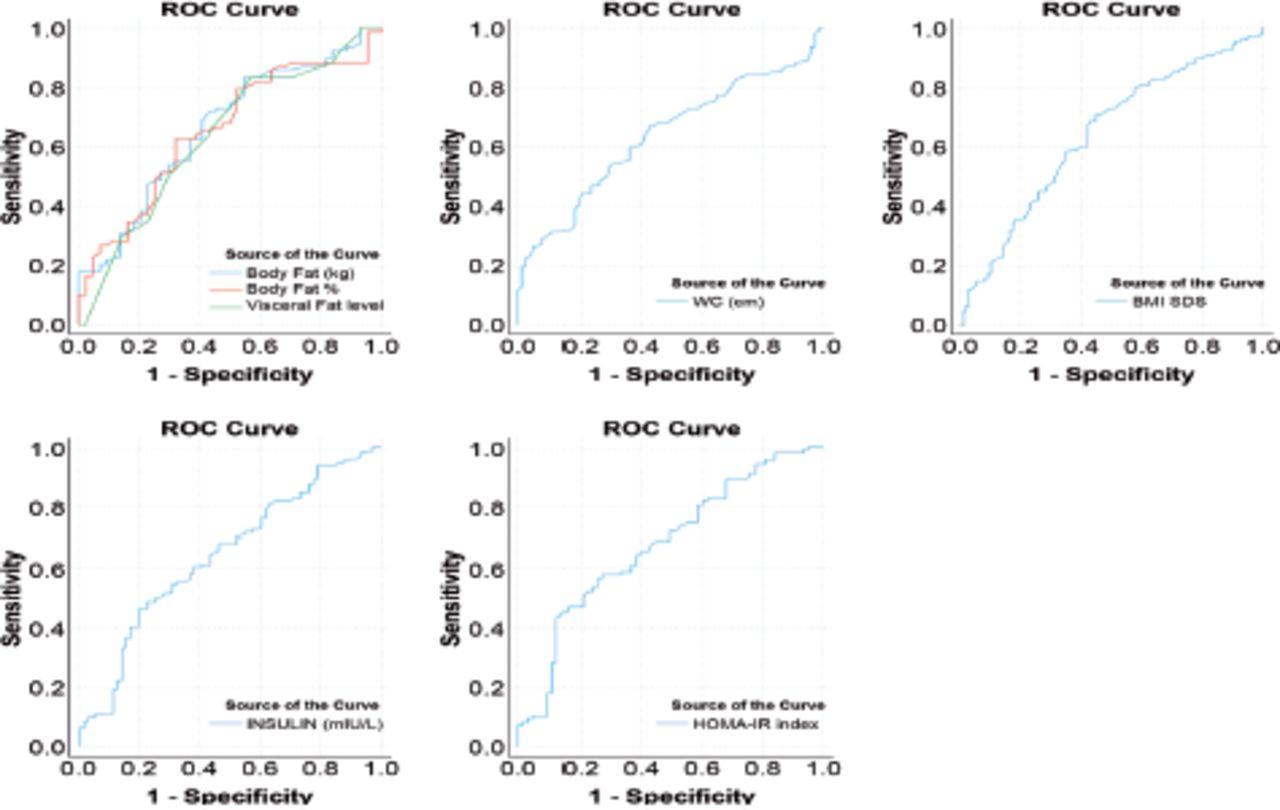
Logistic regression analysis revealed that the adiposity indices (clinical and BIA-derived) and IR (HOMA-IR, FI) had significant AUCs (Table 2). Hemostasis model for IR (cut-off point 4.527) had the top point in the ROC curve (Figure 1), with the highest capability to exclude morbidity (specificity 74%). Body mass index SDS had the highest sensitivity (71%), while WC had higher specificity (71.1) than BMI SDS. All were significant predictors of morbidity (p<0.001), with comparable AUCs. Bioimpedance analysis-derived TBF% (cut-off points 46.15%) and VF (cut-off points 15.2%) also had significant AUCs, but with lower sensitivity and specificity (0.002) in addition to lower significance as morbidity predictors (0.009) than clinical adiposity indices. The mean TBF% was found to be 45.52 ± 5.84 which was higher than 98th percentile for any pediatric age.
- Area under curve and cut-off points of the indices of insulin resistance and adiposity to predict obesity-related morbidity in the studied population.

- Receiver Operating characteristic curves of the adiposity indices. ROC: receiver operating characteristic, BMI SD: body mass index standard deviation, WC: waist circumference, HOMA-IR: homeostatic model assessment for insulin resistance
Associations of the adiposity indices and IR with ORM: simple correlation analysis showed a significant association between SBP in the patients who have WT SDS (r=0.2, p=0.02), BMI (0.29, 0.003), WC (0.2, 0.03), HOMA-IR (0.2, 0.04), and VF (0.2, 0.005). There was also a significant increase in age, WHR, and HOMA-IR across the study population based on their glycemic control as shown in Table 3. Regarding dyslipidemia, around one-third of our patients had dyslipidemia. Those patients had significantly higher BMI SDS (p<0.001), WT SDS (p=0.003), HOMA-IR (p=0.003), and FI (p=0.002) than non-dyslipidemia patients. The 25(OH)D level was positively associated with age (r=0.1, p=0.02) and negatively with WT SDS (-0.2, 0.005) and BMI SDS (-0.2, 0.003).
- Comparing of study population based on their glycemic control.
Associations of indices of IR with adiposity measures
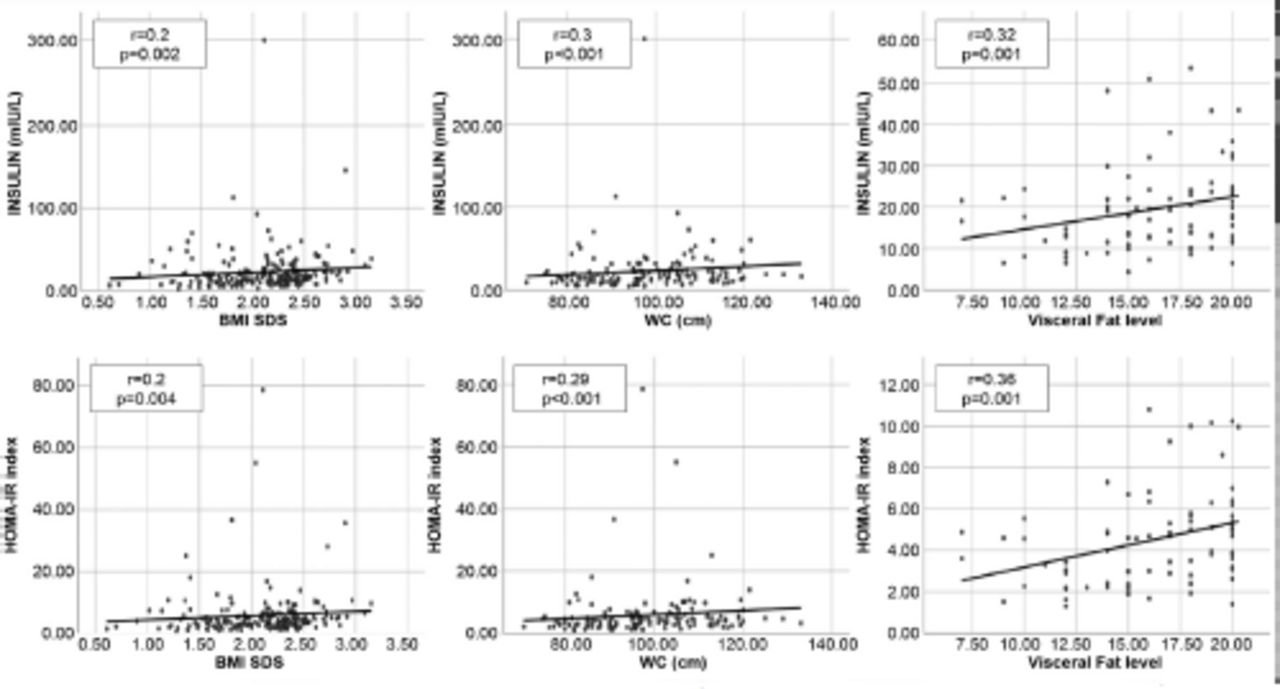
Acanthosis nigricans was found in 64.2% of the patients (n=282), and these children had significantly higher WT SDS (p=0.001), BMI SDS (p<0.001), WC (p=0.02), and VF (p=0.004) than those without acanthosis. As shown in Figure 2, that indices of IR (HOMA-IR, FI) were significantly associated with age (r=0.19, 0.16; p=0.006, 0.06), WT SDS (0.24, 0.25; 0.001, <0.001), BMI SDS (0.2, 0.2; 0.004, 0.002), WC (0.29, 0.3; <0.001, <0.001), WHR (0.18, 0.16; 0.02, 0.04), and VF (0.36, 0.32; 0.001, 0.001) with a comparable strength, additionally HOMA-IR was also correlated with TG levels (r=0.34, p<0.001) and SBP (0.24, 0.04).

- Association between the indices of insulin resistance and adiposity indices. WC: waist circumference, BMI SD: body mass index standard deviation, WC: waist circumference, HOMA-IR: homeostatic model assessment for insulin resistance
Discussion
Comorbidity of pediatric obesity is a disturbing public health problem; the impaired glucose tolerance, increasing BP, and deranged lipid profile can be present since childhood and adolescence with a mounting course through the young adulthood period;. In this study, we found that 37% of the cohort were overweight and 64.7% exhibited IR related comorbidities were the highest in terms of dyslipidemia (32.5%) and prediabetes (31.1%). Hemostasis model for IR (cut-off point 4.527) had the highest ability to exclude morbidity. The ORM prevalence was 61.9%, which is consistent with the results of an American study focusing on the relationship between BMI and morbidity prevalence, and showed that 70% of obese/overweight children had at least one morbidity.19 This work showed that hypertension was detected in 15.8% of obese children and adolescents, while an African meta-analysis reported a lower hypertension prevalence among obese children (5.5%).20 In the same context, Al-Agha et al21 reported hypertension among 6.6%. A recent European study reported prediabetes and T2DM prevalence as 11.9% and 1.4%, respectively, while T2DM was found in 9.04%4 and 5.9% in a German study.22,23 A recent Polish study detected dyslipidemia in 40% of participants, which had the main disorder in the form of low HDL-C level. It was near to the current study percentage, on the other hand, an Emirati study found that 55.3% of children with obesity had dyslipidemia with a higher prevalence of hypertriglyceridemia.24,25 Regarding low vitamin D levels, a Turkish study reported a much greater vitamin D deficiency prevalence (<20 ng/ml; 75%) in children with obesity, whereas a Danish study exhibited a lower vitamin D deficiency (<30 ng/mL levels; 16.5%).26,27
Homostasis model for IR and FI were used to evaluate IR in out patients, and we observed higher values (64.7%, 52.5%) than those decided by Brazilian study (40.5%,39.2).28 Interestingly, in both studies, hyperglycemia was not prevalent among the studied children even with the high prevalence of IR (mean FBS was 5mmol/L in this study, while it was 5.4 mmol/L in the Brazilian study); however, they concluded a similar detection rate of IR between HOMA-IR and FI, while we had a higher detection rate with HOMA-IR. In a nationally representative sample, another group of researchers stated that high HOMA-IR was present in 52.1% of adolescents with obesity,7 with a mean of 4.93 and a median of 4.13.
Comparing 2 groups of the studied patients with and without ORM, the obtained results were agreed with the findings of Asayama et al,29 who concluded that girls with obesity and complications had higher BMI and WC than the girls without complications. This study showed that cases with dyslipidemia had significantly higher BMI SDS, WT SD, HOMA-IR, and FI than non-dyslipidaemic patients, and Brzeziński et al24 reported that childhood obesity and lipid disorders had a significantly higher BMI, WC, and BIA-derived TBF% than those without.
For a closer view of ORM determinants, we established the best cut-off points for both clinical (BMI SDS, WC) and BIA-derived adiposity indices predicting morbidity in obese children, which are outlined in Table 2. The results demonstrated that BMI SDS and WC had a comparable strength as morbidity predictors with a higher sensitivity for BMI SDS (71 vs. 53.9%) and higher specificity for WC (70% vs. 55%). These finding are in line with the results of a meta-analysis conducted by Vazquez et al,30 who concluded that there was no difference between BMI as an indicator of general adiposity, and WC, as an indicator of VA, in predicting diabetes risk in individuals with obesity. In contrast, Hubers et al31 concluded that BMI and WC cut-offs insufficiently describe masses of regional fat depots of varied ages and genders. Researchers reported smaller cut-off points than those identified in this study; a Chinese study found that the optimal cut-off point of BMI SDS to predict dyslipidemia in boys was 1.2.32 In a study of South Asian children carried out in Canada, researchers reported the following optimal cut-off points associated with hypertension risk for girls and boys: BMI SDS (0.9 vs. 1.41) with AUC (0.79 vs. 0.79) and BIA-derived TBF% (29.8% vs. 23.5%) with AUC (0.7 vs. 0.8).33 A lower TBF% cut-off point (19.5% vs. AUC 0.8) was reported by Tompuri et al.34
Our results indicated that BIA-derived adiposity indices were less strong predictors of morbidity than clinical indices, in addition to a lower sensitivity and specificity. These results may add to the results of a German study that compared AUCs of BMI SDS and BIA-derived TBF%, which are comparable significant predictors of ORM, in a sample of more than 3000 children. They found no difference (p>0.05) and concluded that the combined use of these obesity indices did not provide an additive value.35
Insulin resistance is an important therapeutic target in obesity medicine, believing that it is a cardinal link between obesity and impaired glucose metabolism, T2DM, and cardiovascular disease in both adults and children.36 The present study revealed that HOMA-IR is a strong predictor of morbidity (Table 2). A lower cut-off point (2.5) but with similar sensitivity (61%) and specificity (74%) was introduced by Horakova et al.37 In addition, this study presented FI as a comparable predictor of morbidity, such as HOMA-IR.
Study limitation
This study represents a single center in the Saudi Arabia. Involving multiple centers throughout the country would provide more comprehensive ORM data. Further studies including additional morbidities such as sleep apnea, hyperuricemia, and polycystic ovary syndrome, along with more studies of hepatic steatosis, would provide a wider view of ORM.
In conclusion, ORM is widely prevalent in children with obesity. IR is a set for a series of complications, and its targeting would reduce the continuity of ORM. This ORM can be predicted by clinical adiposity indices and IR. The thresholds indicated for the different adiposity and IR indices in identifying ORM suggest that our patients were at risk of ORM at levels of extra adiposity that were higher than those suggested in the literature review. Further research is needed to replicate our findings and confirm the findings prospectively.
Acknowledgment
We would like to thank Rawan Khalid Alsherebi (Clinical Dietician) for her participation in data collection that help to compete the work and all the study participants and their families, who visited the Pediatric Endocrine Outpatient Clinic. We also extend our gratitude to the unit of the Biochemistry Laboratory Department in King Abdul-Aziz University Hospital, Jeddah, Saudi Arabia. We would also like to thank Editage for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 9, 2021.
- Accepted December 7, 2021.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.