


Abstract
Objectives: To correlate demographics, blood groupings, and laboratory characteristics of hospitalized COVID-19 patients with disease severity and outcomes.
Methods: This study included 294 COVID-19 patients. Data on patient age, gender, laboratory results, clinical severity, mortality, comorbidities, and blood group were obtained from medical records retrospectively.
Results: High levels of ferritin (p<0.01), urea (p<0.0001), and creatinine (p<0.05) were detected in intensive care unit (ICU)-admitted patients. Ferritin (p<0.05), glucose (p<0.0001), urea (p<0.0001), and creatinine (p<0.0001) were significantly higher in non-survivor compared to survivor COVID-19 patients. Predictors for ICU admission among patients were ferritin (odd ratio [OR]=0.999, p=0.0055) and urea (OR=0.991, p=0.0001). Predictors for mortality were: age (OR=0.963, p=0.0001), ferritin (OR=0.999, p=0.0149), glucose (OR=0.993, p=0.0001), urea (OR=0.976, p=0.0001), and creatinine (OR=0.556, p=0.0001). The most reliable laboratory parameters in predicting mortality were: age (area under the curve [AUC]=0.685, p<0.0001), ferritin (AUC=0.610, p<0.05), glucose (AUC=0.681, p<0.0001), urea (AUC=0.856, p<0.0001), and creatinine (AUC=0.823, p<0.0001).
Conclusion: High ferritin, glucose, urea, and creatinine levels may predict poor outcomes in COVID-19 patients. These findings could help predict admissions to the ICU and mortality among such patients.
Coronavirus disease 2019 (COVID-19) is a new pandemic disease caused by an emerging strain of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus.1 This new coronavirus was discovered for the first time in China in December 2019 and spread rapidly throughout the world. Thus, a worldwide health emergency was declared by the World Health Organization (WHO) in January 2020.2 The disease’s initial symptoms spanned from mild and non-specific (primarily fever, coughing, and muscle pain) to severe acute respiratory distress and, in some cases, death. As of May 2023, more than 750 million verified COVID-19 cases have been reported to the WHO, including more than 6.5 million deaths worldwide. It is estimated that over 13 billion vaccine doses have been administered.3 In Saudi Arabia, there were more than 800,000 confirmed cases of COVID-19 by that time, with more than 9,000 deaths, of which approximately 54,000 confirmed cases and more than 800 deaths were in the Asir Region, Saudi Arabia.4 According to a recent statement issued by the WHO, COVID-19 has been declared to no longer be an international health emergency, but rather has become an established health issue in need of long-term management.3
Following the outbreak of COVID-19, investigators studied the possible connection between ABO blood group and susceptibility to COVID-19 and its reported associations.5,6 It is well-known that several risk factors contribute to severe infections such as age, gender, and comorbid conditions (such as hypertension, diabetes, respiratory and cardiovascular diseases).7-9 Researchers have also found correlations between laboratory findings and severity in COVID-19 patients, specifically elevated total leukocyte count, D-dimer test, C-reactive protein, alanine transaminase, and serum ferritin.10,11 The severity of COVID-19 disease is also linked to inflammation.11
It is essential to identify factors that are associated with severe infection or that predict disease progression. In identifying markers associated with COVID-19 disease severity, we may be able to improve our understanding and provide better guidance on identifying patients with high risk at an earlier stage and on developing better disease prevention strategies for reducing mortality and disease severity. Also, markers associated with severe COVID-19 infections could lead to optimizing the selection of effective therapies or the development of new targeted therapies, thereby reducing treatment costs and side effects.
The clinical characteristics of COVID-19 patients in Saudi Arabia have been documented in several studies, but there is only limited information regarding the severity of COVID-19 in the Asir province.12,13 Considering these previously published studies, the aim of the present study was to correlate demographics, blood groupings, and laboratory characteristics of hospitalized COVID-19 patients in Abha, Asir Region, Saudi Arabia, with disease severity and outcomes. The rates of mortality and admission to the intensive care unit (ICU) caused by COVID-19 were collected to evaluate the tendency of the relation.
Methods
This single-center retrospective study was carried out on 294 COVID-19-positive individuals hospitalized at Asir Central Hospital, Asir Region, Saudi Arabia, between January and September 2020. Asir Central Hospital is a tertiary hospital located in Abha with more than 500 beds that offers healthcare for patients in the southern region. All patients diagnosed positive for COVID-19 with registered ABO and Rh-D blood groups were included in this study. Patients were excluded if they did not have a positive result for SARS-CoV-2 detection in respiratory specimens and sufficient laboratory data for analysis. Patient data such as gender, age, ICU admission, mortality, ABO type, Rh group, glucose, urea, creatinine, and ferritin were obtained from the Laboratory Information System (LIS) and patients’ medical records. Ethical approval (ECM#2022-2806) for this study was obtained from the Ethics Committee of King Khalid University, Abha, Saudi Arabia.
Statistical analysis
Microsoft Excel 16.67 (22111300) and GraphPad Prism (Version 9.00 for Mac, GraphPad Software, San Diego CA) were employed for statistical analysis and graph preparation. Chi-squared tests were used to determine the strength of relationships between 2 non-parametric data. Student’s unpaired T-test was applied for group comparison. Logistic regression analysis was carried out to detect factors associated with COVID-19 disease severity and outcome, and logistic regression models were used to assess odds ratios (OR) with 95% confidence intervals (CI) for all blood types. Receiver operating characteristic (ROC) curves and area under the curve (AUC) were used to determine the biomarkers associated with COVID-19 severity and mortality. The laboratory finding data are presented as mean ± standard deviation (SD). A p-value of <0.05 was considered significant. Qualitative data were expressed as numbers and percentages.
Results
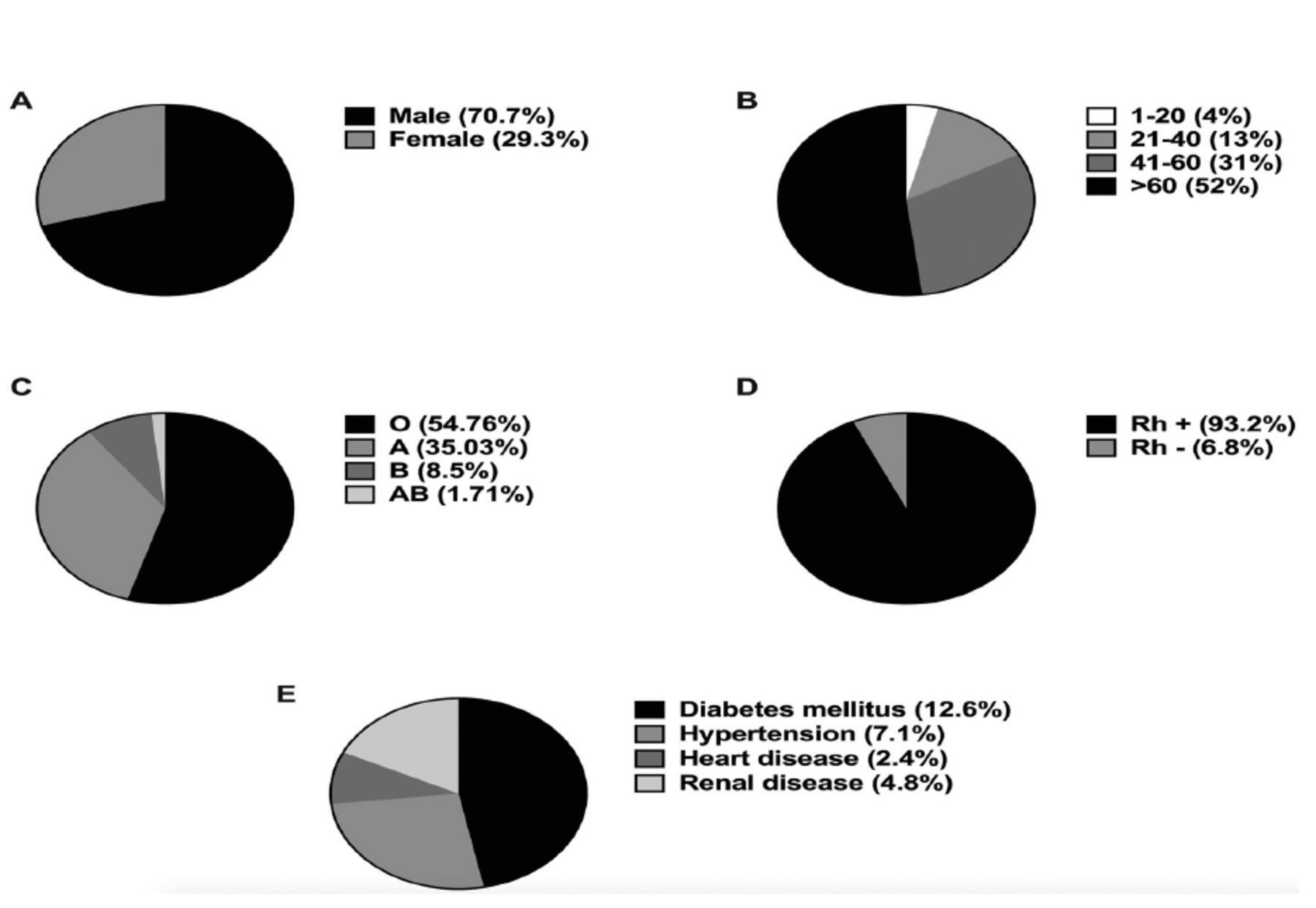
A total of 294 COVID-19 patients were enrolled for this study. Figure 1 presents their demographic and clinical characteristics. Of the 294 participants, 208 (70.7%) were male and 86 (29.3%) were female (Figure 1A). The average age of the patients in this study was 59.4±18.6 years, with an overall range of 1-102 years. A total of 153 (52%) patients were over 60 years old (Figure 1B). The patients were grouped based on their ABO and Rh-D blood types. The distribution of AB blood type was 5 (1.71%), B blood type was 25 (8.5%), A blood type was 103 (35.03%), and O blood type was 161 (54.67%) (Figure 1C). A total of 274 (93.2%) patients were Rh-D positive, and 20 (6.8%) were Rh-D negative (Figure 1D). Based on the information available concerning comorbidities, 27 (12.6%) patients had diabetes, 21 (7.1%) were hypertensive, 7 (2.4%) had heart disease, and 14 (4.8%) had kidney disease (Figure 1E).

- Demographic and clinical characteristics of coronavirus disease-19 (COVID-19) patients. A) Pie chart showing gender distribution of COVID-19 patients. B) Pie chart showing age distribution of COVID-19 patients. C) Pie chart showing ABO blood group distribution of COVID-19 patients. D) Pie chart showing Rh blood group distribution of COVID-19 patients. E) Pie chart showing distribution of comorbidities among COVID-19 patients.
We then divided participants into those admitted to ICU versus those who were not. Of the 294 total patients, 157 (53.40%) cases recovered without requiring admission to the ICU, while 137 (46.6%) required ICU admission. With regard to gender and ICU admission, 100 (73%) male and 37 (27%) female patients were referred to the ICU, whereas 108 (68.8%) male and 49 (31.2%) female patients were not. The mean age of the non-ICU-admitted was 58.24±19.37 years, and that in the ICU-admitted group was 60.51±17.44 years. A total of 75 (54.7%) of the 137 COVID-19 cases admitted to the ICU were over 60 years of age. ABO blood group analysis revealed that >50% of ICU- and non-ICU-admitted patients were type O. Analysis of the Rh-D blood group among patients revealed that 149 (94.3%) of non-ICU-admitted patients and 126 (92%) of ICU-admitted patients were Rh-D positive. Neither ABO (p=0.89) nor Rh (p=0.43) blood group differed significantly between ICU- and non-ICU-admitted patients (Table 1).
- Comparison of demographics, clinical characteristics, and blood group between non-intensive care unit-admitted and intensive care unit-admitted coronavirus disease-19 patients.
We also assessed the incidence of comorbidities relative to ICU admission and found no significant differences (p>0.05; Table 1). However, some laboratory analyses revealed substantial variation among ICU and non-ICU patients. Specifically, high levels of ferritin (1165±636.9 ng/ml, p<0.004), urea (119.3±92.07 mg/dl, p<0.0001), and creatinine (2.020±18.12 mg/dl, p<0.05) were detected in patients admitted to the ICU (Figure 2A).

- Column bar graphs comparing ferritin, glucose, urea, and creatinine among COVID-19 positive patients. A) Column bar graph comparing ferritin, glucose, urea, and creatinine among non-intensive care unit (ICU)- and ICU-admitted coronavirus disease-19 (COVID-19)-positive patients. The mean ferritin was 1165±636.9 vs. 867.7±642.4 (p=0.004), glucose was 192.5±81.27 vs. 178.2±95.05 (p=0.17), urea was 119.3±92.07 vs. 67.75±66.77 (p=0.0001), and creatinine was 2.020±18.12 vs. 1.560±2.021 (p=0.042) in ICU-admitted versus non-ICU patients. B) Column bar graph comparing ferritin, glucose, urea, and creatinine among non-survivor and survivor COVID-19-positive patients. The mean values of these markers in non-survivors and survivors were: 1141±673.2 vs. 897.6±619.1 (p=0.021) for ferritin, 211.9±86.21 vs. 162.5±85.29 (p=0.0001) for glucose, 141.7±92.20 vs. 50.51±44.35 (p=0.0001) for urea, and 2.502±1.994 vs. 1.174±1.669 (p=0.0001) for creatinine. P-values were calculated with the unpaired Student’s T-test. *P<0.05, **p<0.01, ***p<0.001, ****p<0.0001, ns: non-significant
We further categorized patients as survivor and non-survivor patients. Age (65.77±15.77, p<0.0001), ferritin (1141±673.2, p<0.021), glucose (211.9±86.21, p<0.0001), urea (141.7±92.20, p<0.0001), and creatinine (2.502±1.994, p<0.0001) were significantly elevated in non-survivor compared to survivor patients. We found no significant relationship between the study groups in regard to gender, blood group, or comorbidities (p>0.05; Table 2 and Figure 2B).
- Comparison of demographics, clinical characteristics, and blood group between non-survivor and survivor coronavirus disease-19 patients.
A detailed analysis of the relationship between gender, age, ferritin, glucose, urea, and creatinine of COVID-19 patients is provided in Table 3. Risk factors for admission to the ICU patients were ferritin (OR=0.999, 95% CI: [0.998-0.999], p=0.0055), urea (OR=0.991, 95% CI: [0.987-0.994], p=0.0001), and creatinine (OR=0.877, 95% CI: [0.763-0.993], p=0.0502). Additionally, we carried out logistic regression analysis to estimate the risk of mortality from COVID-19 associated with the various laboratory parameters. Risk factors for mortality were age (OR=0.963, 95% CI: [0.948-0.976], p=0.0001), ferritin (OR=0.999, 95% CI: [0.998-0.999], p=0.0149), glucose (OR=0.993, 95% CI: [0.990-0.996], p=0.0001), urea (OR=0.976, 95% CI: [0.970-0.982], p=0.0001), and creatinine (OR=0.556, 95% CI: [0.442-0.682], p=0.0001). In short, logistic regression analysis revealed age, ferritin, glucose, urea, and creatinine to each be an effective indicator of COVID-19 severity (Table 3). This analysis found no significant association between blood group and COVID-19 mortality (p>0.05).
- Association of gender, age, ferritin, glucose, urea, and creatinine with intensive care unit admission and mortality among coronavirus disease-19 patients.
The capacity of age, ferritin, glucose, urea, and creatinine to predict COVID-19 ICU admission and mortality was evaluated using the ROC curve, specifically AUC. In predicting ICU admission, the AUC for ferritin was 0.637 (p=0.003), AUC for glucose was 0.573 (p=0.029), AUC for urea was 0.703 (p<0.0001), and AUC for creatinine was 0.657 (p<0.0001). These parameters were significantly able to discriminate between non-ICU admitted and ICU admitted patients (Figure 3A). In predicting mortality, the AUC for age was 0.685 (p<0.0001), 0.610 (p=0.0187) for ferritin, 0.681 (p<0.0001) for glucose, 0.856 (p<0.0001) for urea, and 0.823 (p<0.0001) for creatinine, indicating that these markers are sensitive predictors of COVID-19 mortality (Figure 3B).

- Receiver operating characteristic (ROC) curve analysis of age, ferritin, glucose, urea, and creatinine across coronavirus disease-19 (COVID-19)-positive patients. A) Intensive care unit (ICU) admission is considered a positive actual state. Receiver operating characteristic curve analysis in non-ICU-admitted vs. ICU-admitted gave the area under the curve (AUC) values of 0.536 for age (p=0.283), 0.637 for ferritin (p=0.003), 0.573 for glucose (p=0.029), 0.703 for urea (p<0.0001), and 0.657 for creatinine (p<0.0001). B) Non-survivor is considered a positive actual state. Receiver operating characteristic curve analysis in survivors vs. non-survivors gave AUC values of 0.685 for age (p<0.0001), 0.610 for ferritin (p=0.0187), 0.681 for glucose (p<0.0001), 0.856 for urea (p<0.0001), and 0.823 for creatine (p<0.0001).
Discussion
This retrospective study aimed to determine the factors that predict ICU admissions and outcome within COVID-19 patients at Asir Central Hospital, Asir Region, Saudi Arabia. Patients with COVID-19 were found to have significant associations of biomarkers such as ferritin, glucose, urea, and creatinine with admission to the ICU and mortality.
Previous reports indicate high mortality in COVID-19 patients according to their age, with increased age being correlated with high risk of COVID-19 illness, ICU hospitalization, and death.7,8,14 In mechanistic terms, COVID-19 severity is increased among older patients due to decreased immunity, increased oxidation activity of the body, a decline in overall body function, and an inefficient defense system.15 In our study, the vast majority of COVID-19 patients were in their 50s and 60s, and most were men, which is consistent with other findings; for example, patients suffering from COVID-19 in Wuhan (China) had a median age of 56.7 years.6-8 The occurrence of severe illness was higher in elderly patients.16 We also found an association between mortality and age comparable to previous studies, with patients who died being mostly elderly.17 Furthermore, we found age to be highly correlated with mortality due to COVID-19, which finding agrees with a previous study.18 Finally, the ICU admission rate for hospitalized patients in our study was 46.4%. This is in agreement with a prior report, which stated that nearly half of COVID-19 patients who are hospitalized in Saudi Arabia are admitted to the ICU.19
Previous studies have reported mixed results concerning ABO blood group, with some showing no relation between ABO blood group and hospital admissions and mortality, while others have demonstrated that the O group in particular is protected.20-23 In our blood group analysis of COVID-19 patients, we found the most common blood group to be O (54.7%). Neither ABO nor Rh blood groups were significantly associated with COVID-19 mortality or ICU admissions. These findings are in line with a study from the United States, which found O to be the most predominant blood group in patients suffering from COVID-19. However, it observed no relation between blood type and COVID-19 severity or hospital admission.24 Other studies have shown that COVID-19 has become more common among the younger generation and people with blood type O.25
Our results regarding blood type are also consistent with other studies in Saudi Arabia; blood group O was likewise reported to be of higher prevalence among COVID-19 patients from Makkah, Saudi Arabia.26 Badedi et al13 concluded that a large percentage of COVID-19 patients from Jazan, Saudi Arabia, were of type O with no connection between COVID-19 severity and blood group. The increased frequency of COVID-19 in Saudis with the O blood group may be because it is the major ABO blood group among Saudis living in Asir.27 The distribution of blood types among participants in this study reflects the local population.
As a point of contrast, other reports have found that the A blood group is most common among COVID-19 patients.28 Both Ad’hiah et al6 and Zheo et al5 demonstrated that group A patients have heightened risk of infection and death from COVID-19. Several factors might account for these conflicting results, including differences in populations and geographical locations; in addition, confounders such as comorbidities that may not have been taken into account in some studies. Finally, the controls selected for comparison may also contribute to inconsistency of findings, particularly taking randomly selected blood donors as controls. The majority of blood banks recruit O-type donors, which may explain why epidemiological studies tend to focus on this group.29 Accordingly, we feel that ABO blood grouping should never be used as the sole determinant for projecting the expected intensity and outcome of COVID-19 disease.
We additionally carried out regression analysis and used ROC curves to assess the diagnostic accuracy of ferritin, glucose, urea, and creatinine levels in relation to risk of ICU admission and mortality. This analysis indicated that laboratory findings could distinguish ICU patients from non-ICU patients. Prior studies have shown that ferritin, urea, and creatinine are significant risk factors for ICU admission.30,31 In the present study, levels of urea, creatinine, ferritin, and glucose were elevated in ICU-admitted patients, and AUC values indicate that these markers could accurately anticipate ICU admission in Saudi patients with COVID-19. This finding is consistent with previously published data, and thus these markers could help to identify severe patients early and inform decisions on immediate ICU admission.
Similarly, previous reports have highlighted several laboratory parameters as predictive factors for mortality in COVID-19 cases, including ferritin, glucose, urea, and creatinine.32-35 These findings align with our results. In our study, mortality rate was significantly correlated with high levels of ferritin, glucose, urea, and creatinine.
Ferritin is a protein in the blood that stores iron. The presence of hyperferritinaemia is observed in many inflammation-driven disorders. There is considerable evidence that it is a valuable biomarker across a wide variety of diseases, including cancer, rheumatologic disorders, and inflammatory disorders. In a recent meta-analysis, high serum ferritin was found to be associated with more severe disease and negative outcomes from COVID-19.36 It is unclear exactly why high ferritin levels correlate with the severity of COVID-19. Nevertheless, there are several possible causes for this phenomenon, including the secretion of proinflammatory cytokines (namely, TNF-α) and cellular damage, which might promote ferritin synthesis in patients suffering from severe COVID-19.36
Additionally, both the progression and outcome of COVID-19 are significantly correlated with blood glucose level. According to Wang et al,34 patients with increased blood glucose levels have a 58% increase in the probability of progressing and a >3-fold increase in the probability of dying from COVID-19. Other studies have reported COVID-19 patients with high glucose levels to develop acute respiratory distress syndrome.37 The mechanism for the detrimental effect of high blood glucose on COVID-19 patients remains unclear at the moment. According to earlier research, diabetes patients are more likely to suffer from impaired innate immunity due to malfunctioning macrophages and lymphocytes.34 It is therefore possible that diabetes patients are more likely to contract SARS-CoV-2.
Moreover, ICU admissions and mortality are increased in COVID-19 patients with high urea and creatinine levels.31 There is still a lack of understanding of the mechanisms underlying acute kidney injury in COVID-19 patients. One of the proposed mechanisms of severe renal impairment in COVID-19 patients is overexpression of angiotensin-converting enzyme 2, a receptor for SARS-CoV-2; however, it is still debatable. Also, there has been evidence that SARS-CoV-2 infects human kidney tubules directly and induces severe tubular damage.38 Accordingly, our findings are consistent with previous research.
Study limitations
We acknowledge some predictable limitations of this work inherent to the nature of retrospective studies. The small sample size is the first constraint. A larger cohort of patients is required to validate the associations of blood groups and laboratory findings with COVID-19 severity and outcome. This study was carried out at only one center, so further multi-center surveys are also necessary. Furthermore, some patients in this study lacked a medical history and laboratory values. In addition, differences in treatment protocols between patients could be contributory factors; however, we could not carry out correlative analysis since treatment data was unavailable.
In conclusion, this single-center observational study aimed to examine predictors of ICU admission and mortality among COVID-19 patients in Asir, Saudi Arabia. The identification of potential risk factors for COVID-19 severity may assist clinicians in identifying patients who require priority treatment to prevent progression of the disease. We observed that the elderly patients had the highest rates of ICU admission and mortality. Other significant risk factors for ICU admission were ferritin, urea, and creatinine. We also found that high levels of ferritin, glucose, urea, and creatinine can predict poor outcomes. Thus, stratifying patients based on biomarkers could be an effective strategy for assessing risk. While COVID-19 is more common among patients with blood group O than among those with types A, B, and AB, illness severity and outcomes were not significantly different in any blood group.
Acknowledgment.
The authors gratefully acknowledge the Department of Laboratory, Asir Central Hospital, Abha, Asir Region, Saudi Arabia, for their cooperation in this study. The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University, Asir, Saudi Arabia, for funding this work through General Research Project under grant number (GRP/126/43). The authors also would like to thank SERVICESCAPE (www.servicescape.com) for English language editing.
Footnotes
Disclosure. This study was funded by the Deanship of Scientific Research at King Khalid University, Abha, Saudi Arabia, through General Research Project under grant number (GRP/126/43).
- Received March 4, 2023.
- Accepted July 11, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
{kind=link}
{kind=link}