


Abstract
Objectives: To investigate the usability of neopterin in demonstrating the progression of COVID-19. As a result of uncontrolled activation of COVID-19 monocytes and macrophages, IFN gamma increases and the resulting inflammatory response causes organ damage. IFN released from T cells causes an increase in gamma neopterin levels. Therefore, measurement of neopterin levels can be used to indicate immune system activation and disease progression.
Methods: The study was carried out prospectively in two different centers. The patients were divided into two groups (mild-moderate and severe) and clinical, laboratory, imaging findings and neopterin levels at hospitalization were compared.
Results: 100 patients were included in our study, 41 of these patients were male. Forty-six patients were identified as severe COVID-19. C-reactive protein, lymphocyte count, fibrinogen, D dimers, lactate dehydrogenase, procalcitonin, troponin and neopterin levels were significant in indicating disease severity. (p<0.05). In ROC analysis, 0.642 for neopterin, 0.698 C-reactive protein, 0.331 lymphocyte count, 0.679 procalcitonin, 0.633 fibrinogen, 0.667 D dimers, 0.655 troponin and 0.706 lactate dehydrogenase were detected and these values were significant.
Conclusion: In our study, neopterin was detected as an important indicator in determining the course of COVID-19.
The coronavirus disease (COVID-19) has led to a pandemic all over the world. Excessive inflammatory response and coagulopathy are held responsible in the pathogenesis of the disease, and increased inflammatory markers and chemokines have been detected in the course of the disease.1-3 Excessive inflammatory response causes an uncontrolled increase of monocytes and macrophages mediated by Interferon gamma (IFN-y) and triggers organ damage. Interferon gamma released from T cells causes an increase in neopterin levels. Because of this relationship between IFN-γ and neopterin, neopterin may be a marker of the cell-mediated immune system. Therefore, measurement of neopterin level may play a role in the early diagnosis and management of the disease.3-6
There are studies showing that neopterin plays a role in the course of viral infections such as human immunodeficiency virus (HIV), hepatitis C virus (HCV), dengue fever, and influenza.7,8 It has been reported that neopterin is useful in demonstrating the severity of the disease in severe acute respiratory syndrome (SARS).1,4
High serum neopterin levels were detected at symptom onset in SARS patients and it was reported that it reached the highest level on the 3rd day. It has been shown that the disease progresses more severely in patients with high neopterin levels in the early stages of the disease.9 Due to the similarities between coronaviruses in the current findings, neopterin may play a role in the timely prediction of disease progression and management of patients in patients with SARS-CoV-2 infection. Limited studies have addressed this issue in relation to COVID-19.7,10-12 Therefore, in our study, we aimed to explorate the role of serum neopterin levels in predicting the course of COVID-19.
Methods
Patients who were hospitalized with the diagnosis of COVID-19 and evaluated in the pandemic service between May 2022 and July 2022 were included. Oropharyngeal or nasal swab samples were evaluated and polymerase chain reaction (PCR)-positive patients were included. Patients’ complaints at the time of admission, demographic data, physical examination, and laboratory results were recorded in the forms. Serum obtained from patients for neopterin measurement was stored at -80°C after centrifugation.
Thoracic computed tomography (CT) was performed on patients with suspected pneumonia due to their complaints and physical examinations, and the findings obtained with CT were recorded. Radiological evaluations were made with low-dose non-contrast computed tomography of the thorax (16-slice multidetector Aquilion-Toshiba-Medical Systems-Otawara-Japan). All images are taken in the supine position with full inspiration. Bilateral and unilateral involvement and presence of ground glass appearance and consolidation with the affected areas were noted. Approval was obtained from the local ethics committee for the study (2022/05-15, 20.04.2022). The patients were informed regarding the study and their consent was obtained. Patients who were pregnant, had malignancies, had end-stage renal disease or had chronic infectious processes were excluded from the study.
Disease severity classification
Disease severity classification and antiviral treatment were made according to the COVID-19 guidelines of the Turkish Ministry of Health. Patients with respiratory rate <30 per minutes, room air SpO2 level >90%, mild to moderate pneumonia are mild to moderate. Severe cases were defined as respiratory rate ≥30 in room air, SpO2 ≤90%, and bilateral diffuse (>50%) involvement of the lung.
Measurement of neopterin
Neopterin measurement in serum was performed with BT LAB brand Human Neopterin ELISA measurement kit (Catalog No: E3155Hu) (Bioassay Technology Laboratory, Birmingham, UK). An absorbance reading was performed using a Chromate 4300 ELISA reader device (Awareness Technology, Inc. Martin Hwy. Palm City, USA). The measurement was made at 450nm. Data were calculated using a 4-parameter logistic regression analysis. Results are expressed in nmol/L.
Statistical analysis
Histogram plots and Kolmogorov Smirnov test were used to show the distribution of continuous data. Those with normal distribution were expressed as mean ± standard deviation, and those with non-normal distribution were expressed as median (minimum-maximum). The independent samples T test was used to compare normally distributed groups, and the Mann-Whitney U test was used for those that did not show normal distribution. Categorical data were given as numbers (%) and Chi-square test was used for comparison. SPSS for Windows, version 1725.0 (SPSS Inc., Chicago, USA) was used, p<0.05 was considered significant.
Results
A total of 41 male and 59 female patients were included in our study. Forty-four (20 males, 24 females) patients were considered mild to moderate disease. There was no significant difference between the demographic data according to the severity of the disease. The complaints of dyspnea at admission were significantly higher in the group with severe disease (p=0.032), and there was no significant difference in terms of other complaints. In the group with severe disease, lung involvement was bilateral on CT and tended to involve all zones (p=0.042, p<0.001) (Table 1).
- Demographic and baseline characteristics of patients with mild to moderate and severe COVID-19.
When antibiotic use was evaluated, there was no significant difference between the groups (p=0.152). Although follow-up in the intensive care unit was higher in the severe group, it was not statistically significant (p=0.075). Oxygen requirement, reservoir mask requirement and MINIPULS steroid therapy (prednol-L 250 mg ıv 3 days) requirement were also significantly higher in the severe disease group (p<0.001, p<0.001, p=0.005). Death occurred in 5 patients (Table 1).
According to laboratory findings, lymphocyte count and hemoglobin were significantly lower in the severe group (p=0.006, p=0.043). C-reactive protein (CRP), fibrinogen, lactate dehydrogenase (LDH), procalcitonin, troponin, neopterin, D-dimer levels were significantly higher in the severe group (p<0.001, p=0.030, p<0.001, p=0.003, p=0.011, p=0.021). =0.006). Laboratory findings are shown in Table 2.
-laboratory test results of patients with mild to moderate and severe COVID-19.
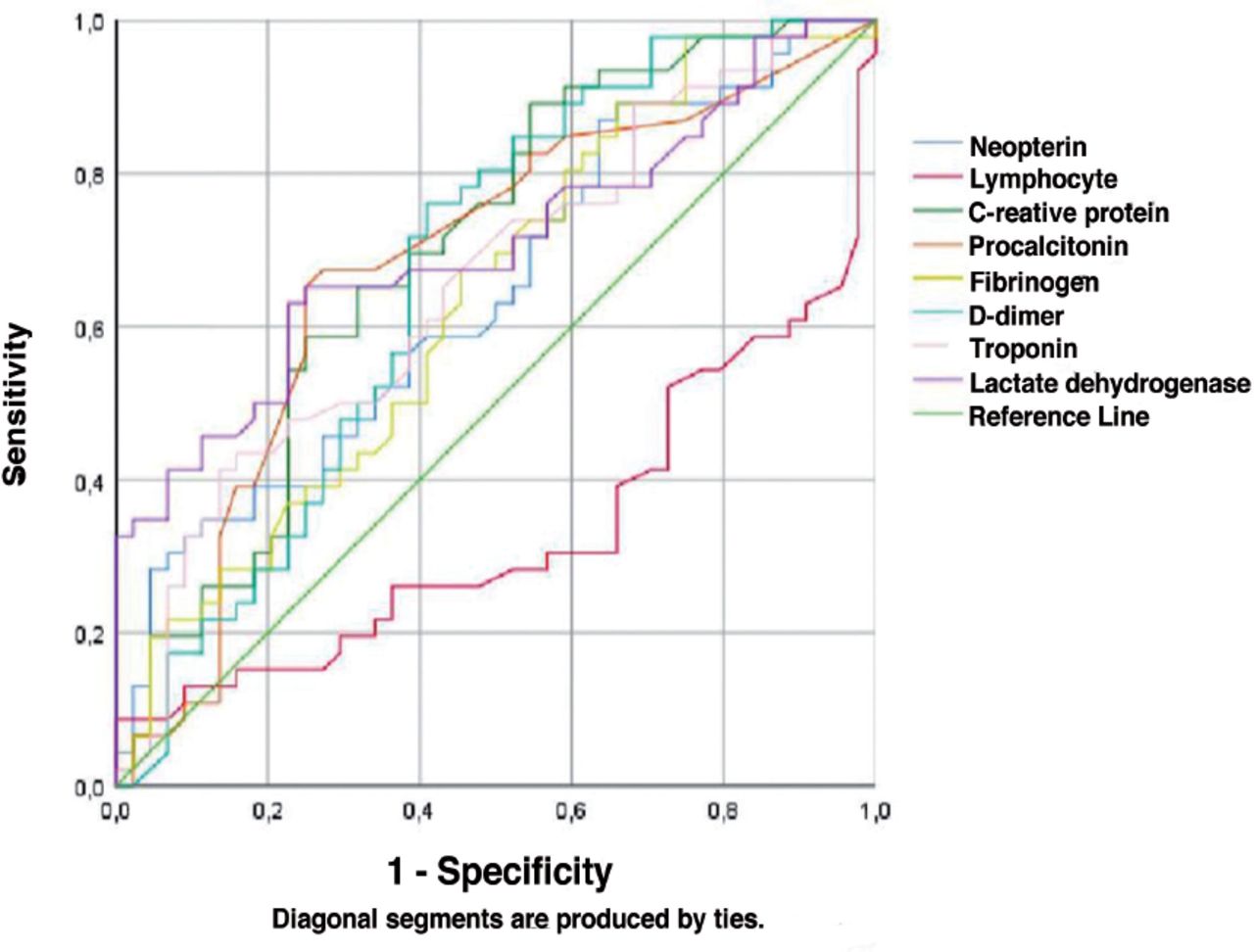
Area under the curve (AUC) values in receiver operating characteristic (ROC) analysis for severe disease neopterin 0.642 (p=0.021), lymphocytes 0.331 (p=0.006), CRP 0.698 (p=0.001), procalcitonin 0.679 (p=0.003), fibrinogen 0.633 (p=0.030), D-dimer 0.667 (p=0.006), 0.655 (p=0.011) for troponin, and 0.706 (p=0.001) for LDH. Area under the curve values and ROC curves for variables that are significant in predicting severe disease are presented in Table 3 and Figure 1.
- Area Under the Curve values of neopterin, lymphocytes count, C-reactive protein, procalcitonin, fibrinogen, D dimers, troponin, and lactate dehydrogenase for severe disease.

- Receiver operating curves of neopterin, lymphocytes count, C-reactive protein, procalcitonin, fibrinogen, D dimers, troponin, and lactate dehydrogenase for severe disease.
Discussion
During viral infections, an increase in interferon gamma causes an increase in mononuclear cells and consequently an increase in neopterin levels. Neopterin shows concentration changes in the blood, urine in the early stages of viral infections; however, this increase can also be seen in other diseases in which the cellular immune system is activated. Neopterin levels can be increased in autoimmune diseases and cancer as well as viral infections.1,14,15
Macrophage activation in the course of COVID-19 causes an increase in neopterin produced by these defense cells, which leads to the use of neopterin in the early diagnosis of the disease.16 Neopterin can be detected in the blood before the clinical picture begins.1,17
Neopterin level is also compatible with other parameters such as CRP, procalcitonin, and interleukin-6, which increase during the disease.4 In our study, neopterin, CRP, lymphocyte count, procalcitonin, fibrinogen, troponin, D-dimer and LDH measured at the time of admission show the severity of the disease. In addition to these parameters in our study, neopterin is a biomarker that can be used in the early period to predict the course of the disease. Similarly, in a study carried out by Chauvin et al,12 when neopterin levels measured at the time of admission to the hospital were used to evaluate the severity of the disease, length of hospital stay and duration of illness; It was found to be higher in patients with long both parameters and in patients who died, regardless of the comorbidity.
In another study, Robertson et al7 investigated the role of neopterin. When mild and severe patients were compared, the neopterin levels in the severely diseased group were found to be twice as high as in the mild group. In this study, repetitive measurements were also made, and it was proven that neopterin levels remained high for a lengthy period and did not return to normal levels in patients with severe disease, whereas neopterin levels decreased more rapidly in patients with mild disease and returned to normal levels in the last measurement.7 Similarly, in a study by Weiler et al,10 neopterin levels measured at admission were found to be associated with disease severity, the need for intensive care and mechanical ventilators, and death. In this study, a 4-fold increase in the risk of death, a 14-fold increase in the need for intensive care, and a 16-fold increase in the need for mechanical ventilation were found in patients with neopterin levels >45 nmol/L at admission compared to patients with neopterin levels <45 nmol/L, and it was proven to be an independent variable in the multivariate analysis.10
In a study by Özger et al,9 neopterin, CRP, procalcitonin, D-dimer, and ferritin were significantly higher in the group with severe disease compared to the mild group. In this study, the AUC values in the ROC curve for neopterin, CRP, D-dimer, procalcitonin, and ferritin to predict disease severity were 0.914, 0.943, 0.870, 0.92 and 0.813 respectively. Similarly, in our study, the AUC values in the ROC curve for estimating disease severity were found to be 0.642 for neopterin, 0.698 for procalcitonin, 0.679 for procalcitonin, 0.633 for fibrinogen, 0.667 for D-dimer, 0.665 for troponin, and 0.706 for LDH. In a contrasting study, neopterin was not found to be significant in predicting disease severity and mortality.11
Study limitations
Firstly, that it was carried out with a small number of patients, and secondly, the measurement of serum neopterin follow-up values was not performed.
In conclusion, our study neopterin, CRP, lymphocyte count, procalcitonin, fibrinogen, troponin, D-dimer, and LDH were determined as independent variables to demonstrate the severity of disease. Among all these variables, neopterin appears to be a new prognostic biomarker in indicating the severity of COVID-19. Neopterin is a specific biomarker for viral infections. Neopterin can be used in the diagnosis of the disease, can predict which patients may have a severe course, and can ultimately help reduce mortality.
Acknowledgment
The authors gratefully acknowledge Scribendi for the English language editing
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 23, 2023.
- Accepted July 11, 2023.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.