


Abstract
Objectives: To analyze the performance of a leading institution in implementing newborn hearing screening and address two key areas: the knowledge gap in screening practice and the prevalence of permanent sensorineural hearing loss in Saudi Arabia.
Methods: We analyzed the prevalence of hearing impairment in all live births at King Fahad Hospital of the University, Al Khobar, Saudi Arabia, from September 2018 to June 2022. Automated auditory brainstem response was used for both initial screening and rescreening. Newborns who failed the rescreening underwent a diagnostic evaluation. We assessed the coverage of initial screening, the rate of lost follow-up, referrals for rescreening and diagnostic evaluation, and the prevalence of hearing impairment.
Results: A total of 5,986 newborns were born. Of these, 96.5% were screened. The passing rate for the initial screening and rescreening was 71.8%. However, 27.5% of newborns were lost to follow-up. Only 0.7% required referral for a diagnostic evaluation. The overall prevalence of hearing impairment was 2.6 per 1,000 newborns.
Conclusion: Early identification of hearing loss through newborn screening improves the lives of affected individuals. Our program currently meets the World Health Organization’s 1-3-6 benchmark goals. However, the underestimation of permanent hearing loss due to the 30% lost-to-follow-up rate is a limitation. Emphasizing the importance of the screening program is crucial to raising awareness and improving the accuracy of prevalence rates.
Hearing loss is a significant clinical condition with a high global prevalence. It affects 0.1% to 0.3% of low-risk newborns, while rates can reach 2% to 4% for newborns in the intensive care unit (ICU).1,2 The World Health Organization estimates that 466 million people have hearing disabilities, including approximately 34 million children. Studies report a global prevalence of permanent hearing loss in newborns of 0.5 to 5.0 per 1,000 infants, potentially increasing in developing countries.3-5 Early detection of hearing impairment is critical to minimize its impact and ensure timely management.4
Delayed detection and management of hearing impairment can have significant negative consequences. Children with undetected hearing loss may experience language development and communication difficulties, leading to poor academic performance. Additionally, these individuals may suffer from social and emotional problems such as loneliness, anxiety, depression, isolation, and frustration due to low self-esteem.6-8 Successful newborn hearing screening programs offer a critical solution. Early detection and intervention through such programs can help ensure speech and language development, leading to positive outcomes in academic, social, and emotional development, ultimately improving the quality of life for individuals with hearing loss.9
The concept of hearing screening emerged in the 19th century. First, the screening was limited to high-risk infants and children. Observational and behavioral testing methods were used, such as observing a child’s response to a ringing bell outside their field of vision.10 In 1969, the Joint Committee on Infant Hearing (JCIH) was formed, bringing together representatives from the American Academy of Ophthalmology and Otolaryngology, the American Speech and Hearing Association, and the American Academy of Pediatrics.11 Their 1970 position statement acknowledged the value of screening but noted the lack of suitable testing procedures, preventing widespread implementation at that time. The discovery of Otoacoustic emission (OAE) in 1988 by David Kemp and the availability of commercial OAE machines paved the way for universal newborn hearing screening. The JCIH endorsed this approach in their 1994 position statement. Joint Committee on Infant Hearing position statements have been updated regularly since then, most recently in 2019.12 The 2000 statement introduced the 1-3-6 principle for early hearing detection and intervention (EHDI) programs: screening by one month, diagnostic audiological and medical evaluation by 3 months, and initiation of early intervention by 6 months. The 2019 statement recommends even earlier intervention, with a revised 1-2-3 principle: screening by one month, diagnostic testing by 2 months, and intervention by 3 months.
Currently, 2 main objective physiological tests are used in newborn hearing screening: (OAEs) and automated auditory brainstem response (AABR).13 Both OAEs and AABR are non-invasive, easy to perform, and can detect hearing loss below 40 dB. The choice of test or combination of tests used in newborn hearing screening programs depends on resource availability. Otoacoustic emission testing measures the emissions of outer hair cells in the cochlea in response to sound. It is faster and cheaper compared to AABR. On the other hand, automated auditory brainstem response testing measures the electrical response of the auditory brainstem to sound at 35 or 40 dB. While more expensive than OAE, AABR is advantageous for identifying auditory neuropathy.13-16 Globally, most newborn hearing screening protocols will implement OAE alone for newborns with low-risk factors. In contrast, protocols that use OAE followed by AABR or AABR alone will be directed to screen newborns with risk factors of hearing loss, including gestational age less than 28 weeks, birth weight less than 1500 g, neonatal ICU (NICU) admission for more than 5 days, hyperbilirubinemia managed by exchange transfusion, TORCH infection, family history of hearing loss, and the use of ototoxic medications.17
Significant progress has been made worldwide in newborn hearing screening since introducing the first universal program in the early 1990s. However, implementation and data collection disparities persist across countries.18 In Saudi Arabia, the newborn hearing screening program became mandatory in 2016. The program was launched at King Fahad Hospital of the University (KFHU) in 2012. The program underwent several refinements, with significant protocol enhancements implemented in 2015 to improve screening accuracy and early intervention. This study aims to evaluate 2 key areas: the effectiveness of the current National Health Service (NHS) program at KFHU and the prevalence of permanent hearing loss in newborns born between September 2018, and June 2022. The study seeks to highlight the strengths and gaps in the current practice. In addition, it will offer insights into the prevalence of hearing loss, contributing valuable data to the global understanding of neonatal hearing health.
Methods
This study was carried out at KFHU in Alkhobar, Saudi Arabia, with approval from the Institutional Review Board. All neonates born at KFHU between September 2018 and June 2022 were included. Newborn hearing screening is a routine medical service offered to all newborns at the hospital, with informed consent typically obtained verbally from parents.
The screening was conducted in a quiet room while the newborns were asleep to ensure optimal conditions for an accurate reading. The screening protocol involved 2 screenings: initial screening and re-screening, followed by diagnostic evaluation for infants who failed both. A GSI Novus AABR machine was used for both stages. The machines automatically interpreted the results as “pass” or “refer” to each tested ear. The first screening was usually performed by a trained nurse as close to discharge as possible, typically within the first 24 hours of life. Newborns who passed the screening in both ears were discharged without further intervention. Newborns who failed the initial screening in one or both ears were referred for re-screening at the outpatient audiology clinic within one month of age. A trained nurse performed the re-screening. Those who passed the re-screening bilaterally were discharged without further intervention. However, newborns who failed re-screening in both or either ear were referred for a diagnostic audiological evaluation by audio-vestibular consultants at 3 months of age. If necessary, a follow-up evaluation at 6 months could occur before starting any management plan.
Data were analyzed descriptively and expressed as percentages. The analysis focused on several outcomes, including coverage of initial screening, rate of loss to follow-up, referral rates for re-screening and diagnostic evaluation, and prevalence of permanent hearing impairment.
Results
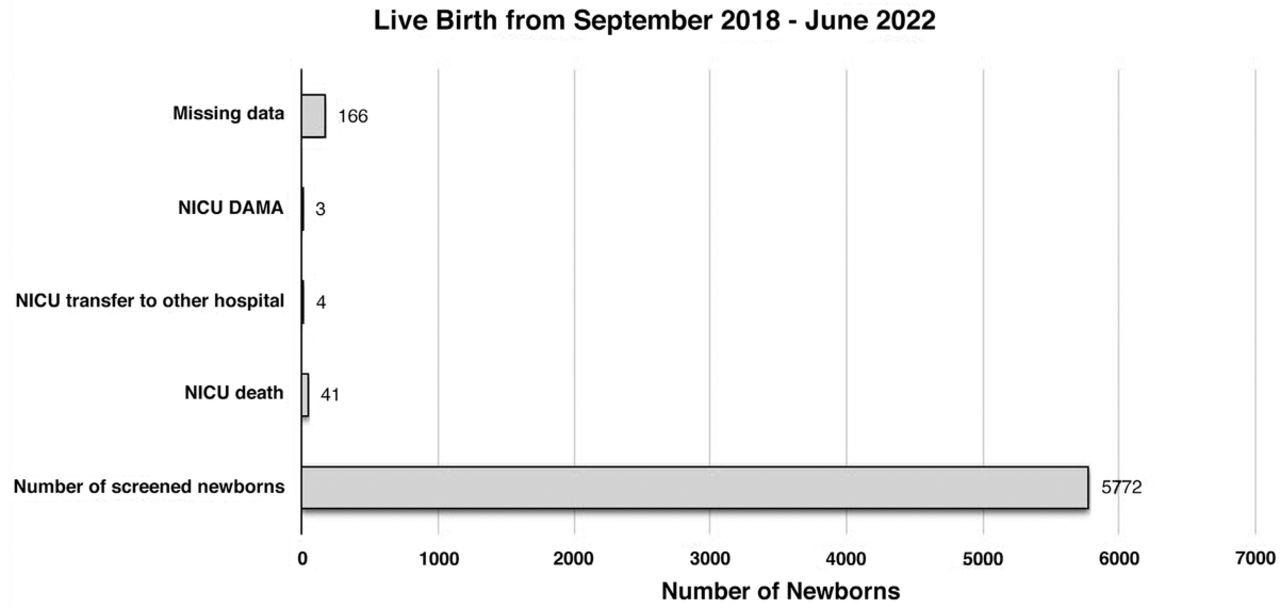
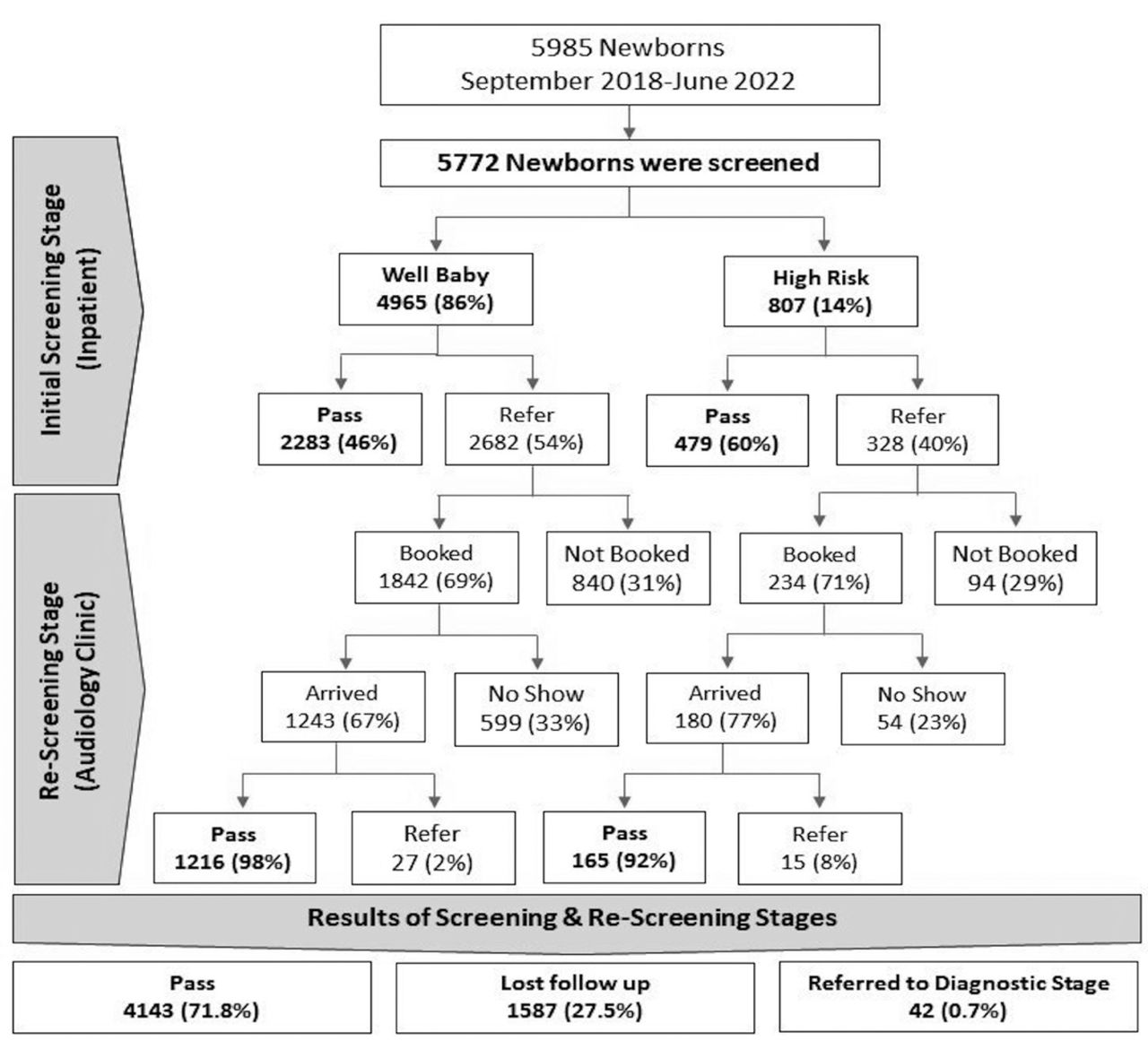
Between September 2018 and June 2022, 5,772 live births were recorded at the hospital. Of these, 51% (2,966) were males and 49% (2,806) were females. A high proportion (96.4%) of targeted newborns underwent newborn hearing screening, while 3.6% were not screened for the reasons shown in Figure 1. The initial screening results are summarized in the flowchart of Figure 2. Only 48% of newborns passed the hearing screening in both ears, while 20% passed in one ear only. The remaining 32% had referred results in both ears. Consequently, around 52% (3010) of newborns were referred for re-screening in the audiology unit, 2682 well-baby and 328 newborns with high-risk factors for hearing loss. Only 70% of newborns who were referred for re-screening booked an appointment. Moreover, analyzing the booked appointments, it was found that only 70% of patients attended and completed the re-screening, and 30% of those needing re-screening did not follow through.

- Newborns hearing screening outcomes (Total: 5986).

- Results of initial and second stages of screening.
Combining the results from both stages, approximately 71.8% of newborns passed the entire screening process. However, 27.5% were lost to follow-up and never completed re-screening, while 0.7 % were referred for diagnostic evaluation.
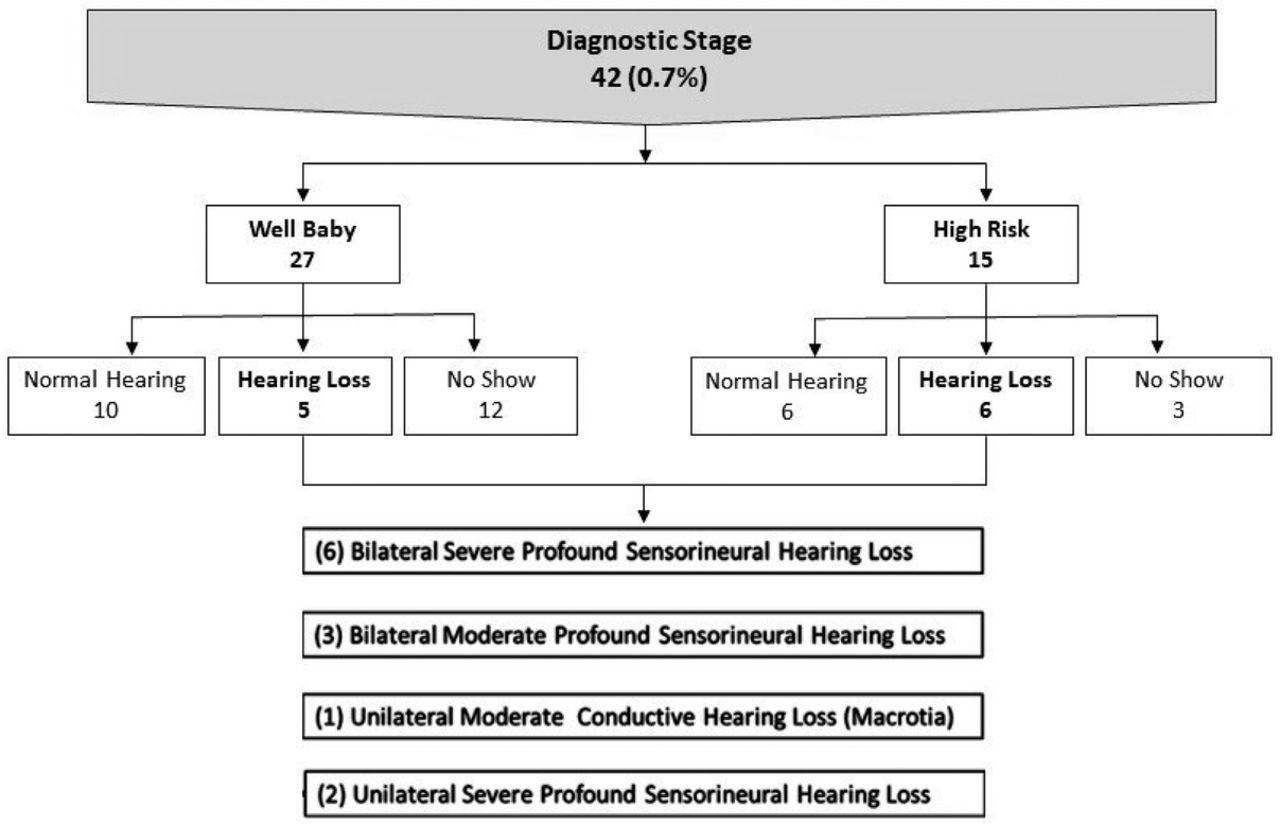
The diagnostic stage results showed 18 cases with normal hearing, 13 who did not show up for follow-up, and 11 diagnosed with hearing loss (Figure 3). Among those diagnosed, 6 had severe bilateral profound sensorineural hearing loss (SNHL), 3 had bilateral moderate SNHL, one had moderate permanent unilateral conductive hearing loss (CHL) due to macrotia, and 2 had unilateral severe to profound SNHL.

- Results of the diagnostic stage.
A total of 4170 newborns completed hearing evaluations by passing through the initial screening, the re-screening, and the diagnostic stages as indicated, and they never missed a follow-up. Among them, 3,514 were well-born babies, while 656 were high-risk newborns. Of the 11 newborns diagnosed with permanent hearing loss exceeding 40 dB HL, 5 were admitted initially to a well-baby nursery and 6 to the NICU. The overall prevalence of permanent hearing loss was 2.6 per 1,000 newborns. In the well-baby group, the prevalence was 1.4 per 1,000, while in high-risk infants, the prevalence was 9.1 per 1000 newborns.
Discussion
Hearing loss is a prevalent health condition worldwide, requiring early detection and intervention. National Health Service programs are crucial in achieving this goal and have been implemented in many countries, including Saudi Arabia.
In Saudi Arabia, the NHS became part of the early detection and intervention system in 2016.19 Our NHS program at KFHU is a pioneer in this initiative. It began in 2012, even before mandatory screening was implemented nationwide. The program has undergone continuous development, with the current protocol established in 2015 and electronic documentation of screening stages introduced in June 2018.
This study aimed to assess 2 critical aspects of the NHS program at KFHU: its effectiveness following the introduction of electronic documentation and the prevalence of permanent hearing loss among newborns born between September 2018 and June 2022. The program achieved a high coverage rate, screening 96.4% of newborns delivered at the hospital, exceeding the JCIH recommendation of at least 95%. However, only 71.8% of newborns passed both the initial screening and re-screening stages. The remaining 27.5% were lost to follow-up and needed to complete re-screening. The proportion of infants referred for formal audiological evaluation after failing both screening stages was 0.7%, which falls within the JCIH guideline of not exceeding 4%.20 Additionally, the program adheres to the recommended EHDI timeline, with screening and re-screening completed by one month of age, diagnostic evaluations performed at 3 months, and intervention initiated by 6 months.
The study found a prevalence of permanent hearing loss exceeding 40 dB HL in 2.6 per 1,000 newborns. This prevalence is higher than reported in other Saudi Arabian studies on similar age groups. Our study utilized AABR testing, known for its higher sensitivity in detecting auditory neuropathy compared to OAE, used in the study by Habib & Abdelgaffar,21 who reported a prevalence of 1.8 per 1,000 newborns. The variations in consanguinity rates between regions may contribute to differences in research findings on hearing loss across Saudi Arabia.22 It is important to note that other studies in Saudi Arabia reported a wide range of hearing loss prevalence. For instance, the King Fahd Military Medical Complex study found a prevalence of 11 per 1,000 newborns.23 This higher number is due to their inclusion of all types and degrees of hearing loss, not just permanent SNHL exceeding 40 dB HL. Earlier studies examining school-aged children reported even wider ranges (13%, 4.4 %, and 1.75%).24-26 Similar to the military complex study, these studies included all types and degrees of hearing loss, potentially including CHL and mild hearing loss not limited to permanent SNHL exceeding 40 dB HL.
Despite the success of the KFHU NHS program in meeting international standards, 2 fundamental limitations still need to be addressed: a high rate of refer results in the initial screening and a significant number of no-shows or lost-to-follow-up cases. One reason for the high referral rate is that KFHU, a government hospital, typically discharges newborns within 24 hours. This short timeframe coincides with factors that can elevate false-positive results, such as vernix in the ear canal and middle ear fluid in newborns. Studies suggest the fourth day of life is ideal for minimizing referrals and false positives.27 However, implementing this delay could lead to even more missed initial screenings. To address this, we provided additional training for screening nurses and prioritized performing the screening as close to discharge as possible. Another area for improvement is the high percentage of no-shows or lost-to-follow-up cases. Despite providing informational leaflets and result cards to parents of infants who fail the initial screening, many still do not book an appointment or do not return for re-screening. This underestimates the true prevalence of hearing loss and delays diagnosis and management, ultimately affecting intervention outcomes. Lost follow-up is a challenge shared by other NHS programs worldwide, where the percentage of lost follow-up varies significantly between countries and within the same country.28,29 At the regional level, in a study by Alanazi, the referral and loss-to-system rates of 2 newborn hearing screening programs in Saudi Arabia were investigated and reported to be 34.92%.30 A similar loss of follow-up rate was found in a study by Alothman,31 with a loss of follow-up reaching 37% after failing the initial screening. Similarly, in a tertiary care hospital in the UAE, a loss to follow-up for a second screening reached 25.49%.32
Various factors contribute to challenges with follow-up appointments, including caregiver unawareness of follow-up importance, forgetfulness, lack of transportation, living far from the hospital, work commitments, responsibilities with other children, or perceiving follow-ups as unnecessary.31 Geographical factors are less impactful in our cohort, as most families of newborns reside in Alkhobar or nearby cities in the eastern province. Notably, our hospital policy sends reminder notifications to patients 48 hours before appointments. Despite this, our outreach efforts found that some families missed audiological diagnostic appointments. Although they knew this, they believed attending was unnecessary because they had no concerns about their child’s hearing. Addressing loss to follow-up challenges by enhancing parental education, strengthening tracking systems, and minimizing false positives are crucial in improving the outcomes of newborn hearing screening programs. Another thing to consider in future protocols is the surveillance program for infants with high-risk factors, even if they pass the initial screening.
Overcoming these challenges can significantly impact the efficiency and effectiveness of our newborn hearing screening program. Early detection ensures timely and appropriate intervention.
In conclusion, hearing loss is one of the most common birth abnormalities. Early identification through NHS programs significantly improves the quality of life for affected individuals. The study at KFHU found a prevalence of hearing loss of 2.6 per 1,000 newborns. Enhancing public awareness about the importance of NHS programs is crucial to increasing participation and reducing the number of lost-to-follow-up cases. This will allow for a more accurate assessment of the true prevalence of hearing loss, facilitate ongoing program evaluation, and ensure optimal management for affected newborns.
Our NHS program meets the EHDI 1-3-6 benchmark goals, emphasizing timely screening, diagnosis, and intervention. However, regular review of the program’s performance remains essential to identify areas for improvement and implement effective solutions.
Acknowledgment
I extend my deepest gratitude to all the nurses in the hospital nursery and the Audiology Unit for conducting the screenings. Mrs.Nadeen Algjryafi, Mrs. Hawraa AlShimer & Mrs. Monirah AlMosabbah. Your dedication and hard work were essential to the success of this study. Additionally, I would like to thank Editage for their assistance with English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 6, 2024.
- Accepted August 13, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.