


Abstract
Objectives: To systematically review evidence on the prevalence of the JAK2V617F (JAK2) mutation and polycythemia vera (PV) among all blood donors, focusing on those with elevated hematocrit. Although blood donors are generally healthy, considering a preclinical stage of myeloproliferative neoplasm, especially in those with polycythemia, is crucial. Evidence on managing these donors is limited.
Methods: We performed a literature search using EMBASE and MEDLINE from inception until August 2023, including studies on the prevalence of JAK2 mutation or PV among blood donors. Eligible studies examined blood donors in hospital or community settings, had a sample size of at least 20 donors, and reported the prevalence of the JAK2 mutation or PV. We assessed bias, extracted data, and used a random effects model meta-analysis to estimate pooled prevalence and 95% confidence intervals. Subgroup analysis differentiated donors with normal hematocrit from those with polycythemia. Heterogeneity was assessed using I2 statistics.
Results: Our review included eleven studies in total. Of those, ten studies examined the presence of a JAK-2 mutation in 1,999 blood donors. The overall proportion of JAK2 mutations was 3% (95% CI 0.60 – 6.9, I2 90.21%). Subgroup analysis revealed a prevalence of 4.7% (95% CI 2.1 – 8.0, I2 0.00%) among repeat donors with polycythemia and 2.3% (95% CI 0.0 – 7.7, I2 0.00%) among healthy ones. Only 3 (309 donors) studies reported PV prevalence, precluding a meta-analysis.
Conclusion: The prevalence of the JAK2 mutation among blood donors is similar to the general population’s but slightly higher among repeat donors with elevated hematocrit. Further research is necessary to establish definitive upper hemoglobin limits for donor deferral.
PROSPERO No.: CRD42023456878
The Janus kinase 2 gene encodes a tyrosine kinase essential for cellular growth and proliferation.1 The JAK2V617F (JAK2) mutation, a somatic gain of function mutation within this gene, leads to the unchecked proliferation of hematopoietic progenitor cells.2 This mutation is linked with various myeloproliferative neoplasms (MPNs), including polycythemia vera (PV), and is present in over 95% of PV cases alone.2
Blood transfusions are vital for saving lives, yet the safety of blood components during donation and transfusion must be a top priority. Although blood donors are typically healthy, the potential presence of an undetected preclinical stage of MPN, especially in individuals with high hematocrit levels, cannot be overlooked.3 Extensive guidelines exist for managing donors with low hemoglobin and hematocrit levels. Regulatory and accreditation bodies like the United States Food and Drug Administration (US FDA) and the Association for the Advancement of Blood & Biotherapies (AABB) specify the minimum hemoglobin thresholds required for donor eligibility.4 However, information on the appropriate upper hemoglobin cutoffs is scarce, and these thresholds vary among different centers. For instance, in the United Kingdom, the upper hemoglobin limit for blood donors is set at 18 g/dL for men and 16.5 g/dL for women; in Australia, it is 18.5 g/dL for men and 16.5 g/dL for women, and at the American Red Cross, the limit is 20 g/dL for both genders.5-7
Identifying blood donors with PV is critical for two reasons. Firstly, the safety of blood donations from patients with MPNs has not been established, and the presence of a hematological malignancy is generally considered a reason for deferral.8 Secondly, detecting these individuals allows for their referral to specialists for further evaluation and appropriate management.
Numerous studies have attempted to determine the presence of the JAK2 mutation among blood donors, particularly those with normal or elevated hematocrit levels.9-11 Results varied across different studies and populations.12-15 These findings are crucial for transfusion medicine professionals striving to implement best practices for donors with elevated hemoglobin and may help establish evidence-informed criteria for donor eligibility.
This study aims to systematically review the existing evidence regarding the prevalence of the JAK2 mutation and PV among all blood donors and those with elevated hemoglobin or hematocrit. It seeks to provide a comprehensive summary of the pooled prevalence of these conditions in blood donors, which could significantly inform the management of donors with high hematocrit and influence health policies concerning donor selection in these cases.
Methods
This systematic review was conducted according to the protocols recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
All studies published up until August 2023 were considered for inclusion. Eligible studies examined blood donors in hospital or community settings, had a sample size of at least 20 donors, and reported the prevalence of the JAK2 mutation and/or polycythemia vera (PV). Studies were excluded if they were irretrievable, if there was no response from the primary authors within one month of contact, or if the methods were poorly reported or unclear. Abstracts were included if they provided sufficient data to assess the prevalence of JAK2 mutation or PV. No studies were excluded based on the language of publication.
Two independent reviewers (MA and AA) screened titles and abstracts, selected studies based on eligibility criteria, reviewed full articles, and extracted data. A consensus or a third reviewer (EM) resolved any discrepancies. Two votes were required to advance a record from the title/abstract screen to the full-text review. The screening process was conducted using Covidence software.16 One study, published in Russian, was translated using Google Translate.
We carried out a literature search in EMBASE and MEDLINE from inception through 2023. Keywords and MeSH terms used in the searches are detailed in Appendix 1 & 2. Additional search strategies included reviewing the reference lists of included articles and searching for “Related Articles” in databases such as PubMed. Searches also extended to conference proceedings for the British Journal of Hematology and the American Society of Hematology (ASH). We included observational studies, both retrospective and prospective cohort studies, as well as case-control and cross-sectional studies. Abstracts were included due to the scarcity of evidence, provided they contained adequate data. Efforts were made to contact the corresponding authors of abstracts to obtain full articles when necessary.
A standardized and piloted Excel spreadsheet was used to extract quantitative and qualitative data. One author extracted all relevant data from each study, while another independently verified them. Discrepancies were resolved by consensus and, if necessary, by a third author.
Extracted variables included year of publication, study design, location, sample size, mean age, smoking status, blood counts, type of hemoglobin test, method of polycythemia diagnosis confirmation, type of JAK2 mutation detection test, mutation load, and the count/frequency of cases, as well as the prevalence of JAK2 mutations and PV. A positive JAK2 mutation was defined as any positive result reported by the study, with a sensitivity analysis conducted to exclude patients with a JAK2 mutation load of less than 1%. The diagnosis of PV was defined by the criteria set by the WHO at the time of the study, as interpreted by the authors of the published studies.
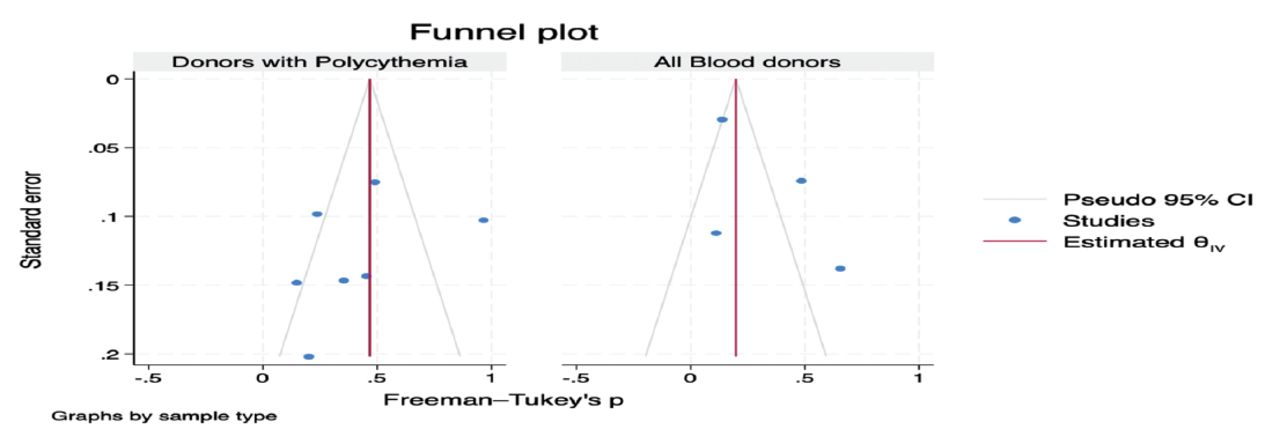
The Newcastle-Ottawa Scale (NOS) for evaluating the quality of observational studies was utilized to assess the risk of bias in individual studies. This scale assesses studies based on the selection of study groups, the comparability of these groups, and the ascertainment of outcomes. Small study bias was evaluated by generating funnel plots and conducting Egger’s test.
The random-effects model, specifically the DerSimonian-Laird method, was utilized to estimate the pooled prevalence and 95% confidence interval (CI). Heterogeneity was assessed using I2 statistics, which measure the degree of inconsistency between studies. Due to anticipated high heterogeneity stemming from differences in background populations among the studies, a random-effects model was favored over a fixed-effects model. Subgroup analyses were conducted for studies that included any blood donors, repeat donors with polycythemia, and donors diagnosed with polycythemia. Post-hoc analyses were performed to exclude patients with a very low JAK2 allele load (<1%) and to remove results derived solely from abstracts. All statistical analyses were conducted using Stata (version 18.0).
Results
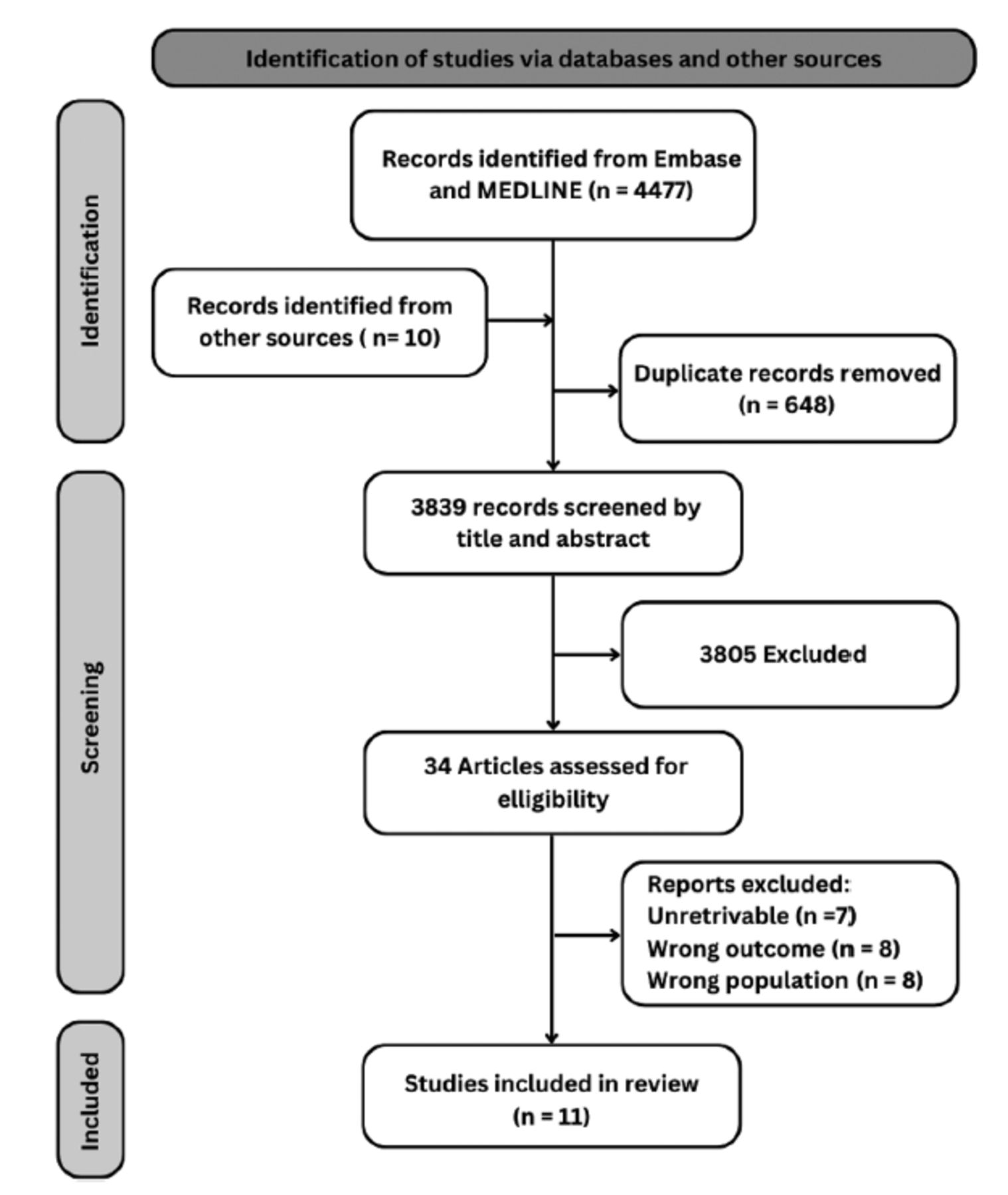
A total of 4,477 studies were initially screened for this systematic review. After title and abstract screening, 3,809 studies were deemed ineligible, leaving 20 studies selected for full-text review. Additional research yielded 14 more studies. Out of these 34 studies, 7 were unretrievable due to a lack of access to abstracts, reports, full texts, responses after contact attempts, or missing contact information. Upon reviewing the full texts of the remaining 27 studies, 16 were excluded. The reasons for exclusion are summarized in Figure 1. Ultimately, 11 studies were included in the systematic review and meta-analysis.9,11-13,15,17-22

- Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart for study selection.
Of the 11 studies included in the analysis, 81% were designed as prospective cohort studies, one followed a case-control design, and one was cross-sectional. These studies were conducted in various countries: 3 in Italy, 2 in India, and one each in Belgium, Iraq, Russia, Malaysia, Denmark, and the USA. The sample sizes ranged from 46 to 1,150 participants. Five studies did not specify their durations, while the others ranged from one month to 2 years. The participants primarily consisted of blood donors with high hematocrit (polycythemia) in 7 studies, while 3 studies included all blood donors, and one study compared cases of donors with polycythemia to controls from the general blood donor pool. Ten studies reported on JAK2 positivity, with participants’ ages ranging from 17 to 77 years. Only 3 studies reported on the proportion of patients eventually diagnosed with PV. The mean hematocrit levels across the studies varied from 44.2% to 58%. Additionally, the mean hemoglobin levels ranged from 14.5 to 19.1 g/dL, red blood cell (RBC) counts from 4.3 to 8.43 million/µL, white blood cell counts from 3.2 to 16.3 × 10^3/µL, and platelet counts from 94 to 527 × 10^9/L. Details of the characteristics of the included studies are found in Table 1 & Appendix 3.
- Characteristics of studies included in the meta-analysis to assess prevalence of JAK2 mutation among blood donors.
Of the patients tested for the JAK2 mutation, approximately 68.1% were male. Smoking status was reported in 5 studies, all involving blood donors with polycythemia. The prevalence of smoking among these donors varied widely, ranging from 84% to 24%14, indicating a notably high prevalence of smoking, particularly among male donors.19,20
The JAK2 detection assays differed across the studies, as detailed in Table 1. The allele load of JAK2-positive patients was not reported in most studies. However, the few studies that did report allele loads noted ranges from 0.07 to 2.58%,<1%, <10 copies, and 37% .9,12,17,19
When assessed for the risk of bias, the scores of the included studies ranged from 5 to 9. This range suggests a generally accepted quality of the studies, with clear criteria for patient selection and outcome reporting. However, most studies did not report the sensitivity and specific cutoffs. Appendix 4 provides a detailed scoring for each study.
Prevalence of JAK2 mutation among blood donors
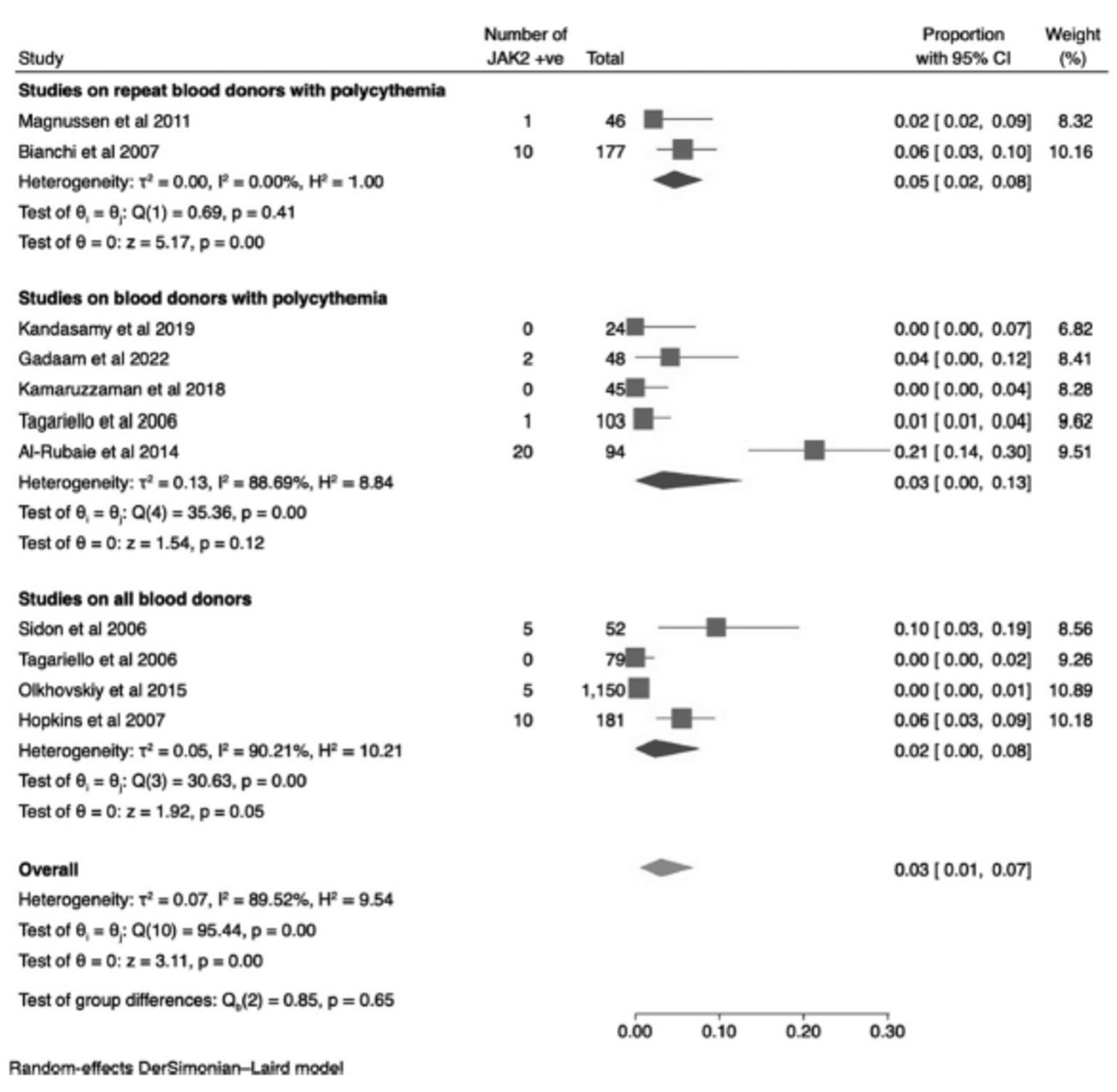
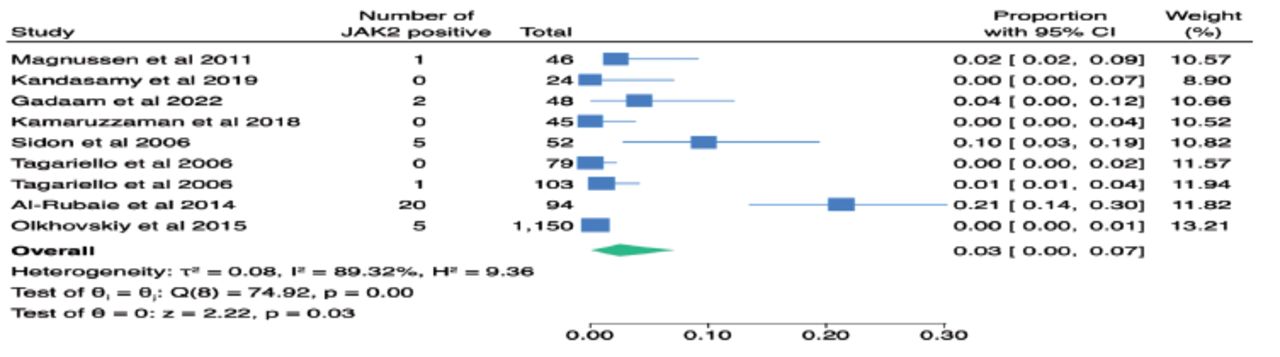
Ten studies involving 1,999 individuals reported the prevalence of the JAK2 mutation among blood donors, ranging from 0.0% to 21.3%. The overall proportion of the JAK2 mutation among donors was estimated to be 3% (95% CI 0.60 – 6.9, I2 90.21%). Subgroup analysis was conducted based on the sample type: i) repeat blood donors with polycythemia, ii) blood donors with polycythemia, and iii) healthy blood donors (with normal hematocrit). The prevalence of the JAK2 mutation among repeat donors with polycythemia was 4.7% (95% CI 2.1 – 8.0, I2 0.00%); among blood donors with polycythemia it was 3.3% (95% CI 3.3–12.8, I2 88.69%), and among general blood donors, it was 2.3% (95% CI 0.0 – 7.7, I2 0.00%). Notably, tests for differences between groups were not statistically significant, as shown in Figure 2.

- Forest plot of the prevalence of JAK2V617F mutation among blood donors (overall, and subgroups).
Significant heterogeneity between studies was observed, which could be attributed to varying cutoff points in the definition of polycythemia across studies, with some using hematocrit and others using hemoglobin levels to establish cutoffs. Details on the hemoglobin/hematocrit cutoffs used by each study are provided in Table 1. There was no evidence of small study bias (Egger’s test, p=0.9), as indicated in Appendix 5.
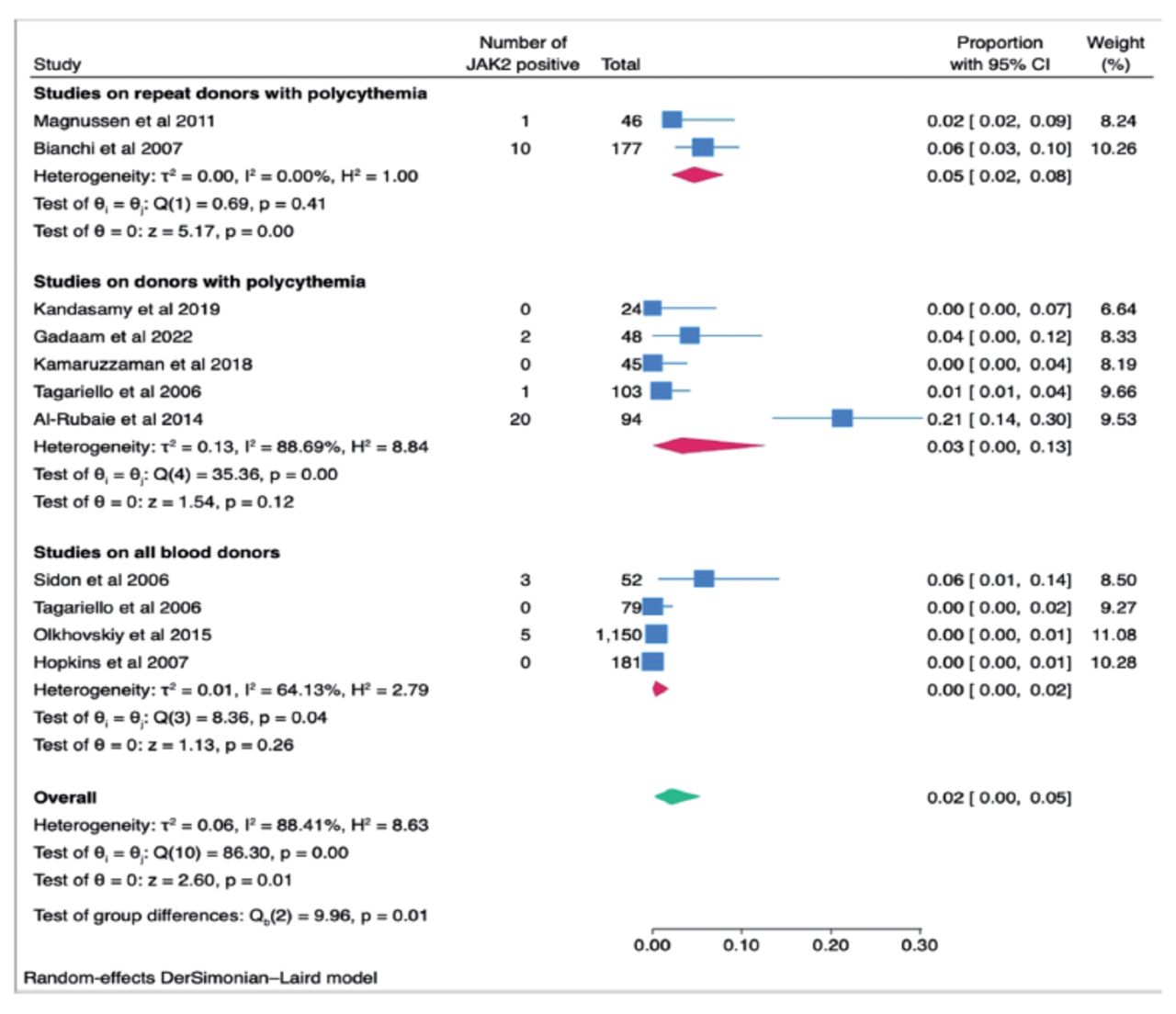
A post-hoc analysis conducted after removing observations reporting very low JAK2 mutation allele levels (<1%) showed a similar result to the primary analysis for donors with polycythemia and a much lower proportion for general blood donors at 0.3% (95% CI 0.0-1.8, I2 64.13%). These details are presented in Appendix 6.
Another post-hoc analysis that excluded abstracts revealed no significant change in the overall proportion of JAK2 mutations among blood donors, as seen in Appendix 7.
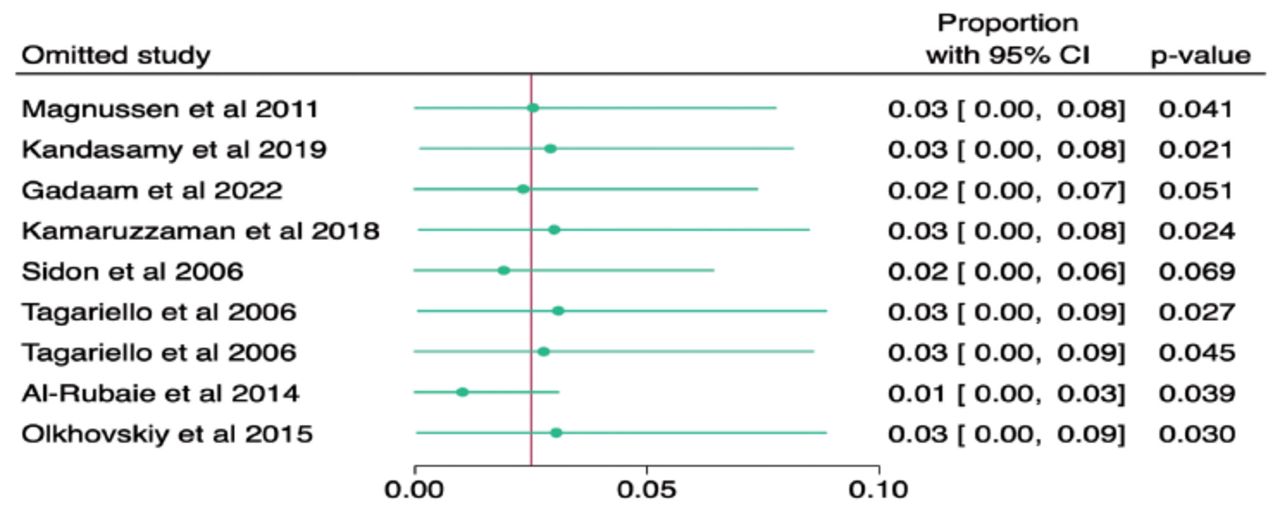
Given the extraordinarily high prevalence of JAK2 mutation detected in one of the studies,20 a meta-analysis excluding this study resulted in an overall JAK2 mutation proportion of 1% (95% CI 0.0-3.1), with the removal of any other study not leading to significant deviations in estimates, as illustrated in Appendix 8.
Prevalence of PV among blood donors
Three studies reported the prevalence of PV among blood donors, ranging from 0.0% to 4.3%.10,13,19 Two of these studies focused on repeat donors with polycythemia, while the other examined all donors with polycythemia. All patients diagnosed with PV were regular blood donors; 2 had donated approximately 100 times. We did not perform a meta-analysis on the prevalence of PV among blood donors due to the very low number of studies, significant heterogeneity between them, and the fact that these studies applied different versions of the PV diagnostic criteria based on the year they were conducted.
We aimed to explore the prevalence of the JAK2 mutation and PV cases among smokers versus non-smokers. However, this was not feasible due to missing information on smoking status in some studies, and those that did report smoking status did not specify whether the donors who were JAK2 positive or diagnosed with PV were smokers.
Discussion
This meta-analysis suggests that the prevalence of the JAK2 mutation among all blood donors, including those with polycythemia and healthy donors, is estimated at 3% (95% CI 0.60 – 6.9). Subgroup analysis reveals a higher proportion, approximately 4.7% (95% CI 2.1 – 8.0), among repeat donors with polycythemia and 3.3% (95% CI 3.3– 12.8) among donors with polycythemia. The lowest proportion, 2.3% (95% CI 0.0-7.7), was observed among studies that included any blood donors. Notably, the estimate among healthy donors significantly dropped to 0.3% when removing very low JAK2 mutation allele levels (<1%). However, data on the prevalence of PV among blood donors was limited, preventing a comprehensive meta-analysis. Nevertheless, it was observed that donors diagnosed with PV were all frequent blood donors with polycythemia.
JAK2V617F mutations have been detected in the general population with varying prevalence reported by different studies.23 For example, a study from China involving 3,935 random samples reported a JAK2 prevalence of 0.9%.24 A study from Denmark25 reported a lower prevalence of 0.1%, while another report from a Danish suburban population found a prevalence of 3.1%, though 42% of those positive had an allele load of <0.1%, with a higher allele burden noted as age increased.26 The variability in prevalence between population studies and blood donor studies likely reflects the performance variability among different JAK2 mutation tests and the absence of standardized cutoff values for determining positive results.27
Various tests are used to determine JAK2 mutation status. Direct DNA sequencing is considered less sensitive for diagnostic purposes; it is also time-consuming and expensive.28 Allele-specific PCR (Amplification Refractory Mutation System [ARMS]) or “sequence-specific primer PCR” is highly sensitive. Real-time PCR offers greater sensitivity than sequencing. In contrast, Restriction Fragment Length Polymorphism (RFLP) is less sensitive but effective for screening, similar to Allele-specific PCR and DNA-melting curve analysis.28 Droplet digital PCR is another precise technology when compared with quantitative PCR.29. This variation in assay sensitivity is particularly relevant for screening in apparently healthy individuals as opposed to patients exhibiting clinical features, who likely carry higher JAK2 variant allele frequency (VAF), and is also significant for monitoring minimal residual disease.
The association of low JAK2 VAF with disease is a topic of considerable debate.30 Currently, there is no defined cutoff to establish a positive JAK2 mutation according to the latest WHO criteria.31 Commonly, a threshold of 1-2% is used in practice.32 A study involving 576 patients with PV showed a heterogeneous JAK2 VAF ranging from 0.3 to 100%, with a median of 41.5%.33 This variability was reflected in the heterogeneity of definitions for a positive JAK2 in this review and a reduction in reported JAK2 positivity from 2.3% to 0.3% among all blood donors when excluding patients with very low JAK2 VAF.
The clinical significance of a positive JAK2 mutation in individuals without evidence of a MPN remains uncertain.34 Although up to 97% of patients with PV carry the JAK2 mutation, it is acknowledged that the presence of the JAK2 mutation alone does not sufficiently explain the development of MPNs. For instance, germline polygenic variation involved in basic hematopoiesis has been identified as influencing the risk of JAK2 mutation clonal expansion and the subsequent risk of MPN development.35
Aside from MPNs, there are other potential adverse associations with the JAK2 mutation. Individuals with clonal hematopoiesis, including those with the JAK2 mutation but without abnormalities in blood counts, face an increased risk of atherosclerotic cardiovascular events.36 Simultaneously, a population study revealed that erythrocytosis (hemoglobin [Hb] >18.5 g/dL or hematocrit [Hct]≥52% in males, and Hb > 16.5 g/dL or Hct ≥ 48% in females) is linked to cardiovascular morbidity and mortality, as well as all-cause mortality.37 This study also showed that approximately 2.2% of patients developed hematologic malignancies, including MPNs, with the JAK2 mutation observed in 5.3% of individuals with erythrocytosis.37 These findings suggest that donors with polycythemia would benefit from additional workup to identify those at risk of cardiovascular events and to address other modifiable risk factors.
In this review, a high prevalence of smoking was observed in studies that reported on smoking status. This could be explained by several factors. Primarily, the studies often focused on donors with polycythemia, where smoking is a common etiology.38 Additionally, a study from the 1980s reflects the then-high prevalence of smoking, reported at up to 72% among males.39 Furthermore, some countries have higher smoking rates, which could also contribute to this trend.40 It is now recognized that the JAK2 mutation is more common in smokers; thus, not only does smoking cause secondary polycythemia, but it is also associated with a higher risk of MPN development.41
Another important aspect of this review is that blood banks appear to encounter higher proportions of individuals with polycythemia compared to the general population. Many such individuals, whether identified with secondary polycythemia or not previously evaluated for an underlying diagnosis, seem motivated to donate blood. Some are encouraged by their physicians, while others are self-motivated. This trend is observed in cohorts of donors on testosterone replacement therapy in Canada and the US.42,43 Smokers may also be particularly motivated to become repeat donors. Our experience suggests that many smokers donate blood to reduce their hemoglobin level, under the impression that it might result in improved health outcomes, although this area lacks extensive research.
Despite the high prevalence of polycythemia and the JAK2 mutation among blood donors and in population studies, PV remains a rare disease. The prevalence of PV among blood donors has not been adequately investigated, with only three studies published on the subject. These studies, conducted in 1986, 2006, and 2014, included a total of 309 blood donors and used varying definitions for the diagnosis of PV over the years. A table summarizing the evolution of the diagnostic criteria for PV can be found in the appendix (Appendix 9).44-47 Notably, significant changes in the diagnostic criteria include the lowering of hemoglobin level cut-off points, the integration of the JAK2V617F mutation identified in 2005, and the requirement of a bone marrow biopsy for diagnosis since 2016.48,49
Although JAK2 mutation testing is a reasonable initial step when PV is highly suspected, many patients with polycythemia ultimately test negative, indicating secondary polycythemia. Multiple researchers have attempted to create algorithms to identify individuals for whom JAK2 testing would be most appropriate, thereby reducing costs and minimizing patients’ psychological stress. Models developed to prioritize patients for testing include the JAK2-tree clinical decision tree by Mahe et al,50 the 2-step algorithm by Piris-Villaespesa et al,32 and the JAKPOT prediction rule by Chin-Yee et al.51 Additionally, a machine-learning approach led to the development of JAKCalc, another promising tool that predicts JAK2 positivity based on blood counts.52
While the reviewed studies do not provide strong evidence for optimal management approaches for blood donors with polycythemia, and despite the lack of data on the safety of blood donated by patients with MPNs, it seems prudent for blood banks to continue deferring potential donors with polycythemia. Depending on the blood bank’s policies and available resources, they may refer all donors with polycythemia for further evaluation, typically by their primary care providers. Blood banks could also perform complete blood counts for donors identified with polycythemia during point-of-care testing and utilize available decision tools to determine the next steps.32,50-52 Evaluating these approaches for clinically relevant outcomes and considering the perspectives of referred donors would be beneficial.
There are several additional research opportunities that can further advance our understanding of this issue. Long-term follow-up of patients who received blood from donors found to have the JAK2 mutation in the included studies would provide valuable information on the safety of blood donated by these individuals. Similarly, long-term follow-ups of donors who were identified with the JAK2 mutation would be insightful to determine the risks of MPN diagnosis in this specific group.
Our literature search yielded no other published systematic reviews attempting to estimate the prevalence of JAK2 mutations or PV diagnoses among blood donors. This study highlights the rates of JAK2 mutation among donors compared to the general population, particularly those with polycythemia. It underscores the need for future large-scale studies to address this frequently encountered question in blood banks and to stimulate discussion on the optimal approach to individuals with polycythemia who present for blood donation. The study’s limitations include the rarity of the JAK2 mutation and PV outcomes, the variability between studies, and the small number of studies and sample sizes, which are influenced by the high costs of conducting large-scale testing.
In conclusion, this meta-analysis reveals that the prevalence of the JAK2 mutation among all blood donors—including those with polycythemia and healthy donors—is estimated at 3% (95% CI 0.60 – 6.9). The prevalence is higher among repeat donors with polycythemia. Data on the prevalence of polycythemia vera (PV) among blood donors is very limited. Although data on the outcomes for these individuals are sparse, we recommend the deferral of donors with polycythemia and further evaluation for the potential need for JAK2 mutation testing. More efforts are required to establish a consensus on the upper limit values of hemoglobin for donor deferral and to develop guidelines for blood centers on counseling and referrals for individuals with polycythemia.
Acknowledgment
We would like to acknowledge the guidance of the late Prof. Nahla Khamis from King Abdulaziz University. We would like to thank Editage (www.editage.com) for English language editing.
Appendix
- Ovid MEDLINE(R) and Epub ahead of print, in-process, in-data-review and other non-indexed citations, Daily and Versions 1946 to August 18, 2023
- Database(s): Embase 1974 to 2023 August 18.
- Further details on characteristics of included studies.
- Risk of bias assessment for cohort study using Ottawa-Newcastle score.

- Egger’s funnel plot of JAK2V617F mutation among blood donors

- Results of post-hoc analysis after removing studies that reported very low JAK2V617F mutation allele levels <1% among blood donors (overall, and subgroups).

- Results of post-hoc analysis after removing abstracts.

- Results of the leave one out meta-analysis.
- Diagnostic criteria of polycythemia vera (PV) from 1975 to 2022.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 13, 2024.
- Accepted November 5, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.