


Abstract
Objectives: To evaluate whether hypothyroidism is a risk factor for transient ischemic attack (TIA).
Methods: We systematically searched Embase, PubMed, Cochrane, Vipers database, China Biomedical Literature Database, Wanfang Data, and China National Knowledge Infrastructure for studies assessing the association between hypothyroidism and TIA (publication cut-off in May 2024). Two researchers independently extracted the data based on inclusion and exclusion criteria. Meta-analysis was carried out using Review Manager 5.3 software.
Results: A total of 7 studies (combined n=190248) were included. Hypothyroidism showed a significant association with TIA (risk ratio [RR]=1.43 [95% confidence interval [CI]: [1.29-1.57]). The association was significant in clinical hypothyroidism (RR=1.45 [95% CI: [1.31-1.62]) but not evident in subclinical hypothyroidism (RR=1.20 [95% CI: [0.90-1.61]). Sensitivity analysis confirmed the stability and reliability of the results from the 7 studies (Begg’s test z=1.2, p<0.01). No significant publication bias was detected in the meta-analysis.
Conclusion: Hypothyroidism, particularly clinical hypothyroidism, may be an independent risk factor for TIA.
PROSPERO No. ID: CRD42024552608
Stroke ranks as a leading neurological disorder leading to long-term disability and is a major cause of morbidity and mortality worldwide.1 In 2019, there were 101 million cases of stroke and 6.55 million deaths from stroke.2 Ischemic stroke, caused by the obstruction of a blood vessel in the brain, accounts for approximately 62.4% of total stroke incidents.2 The direct and indirect costs of stroke are approximately 73.7 billion US Dollars ($) annually.3 The regions with the most substantial burden of ischemic stroke include Southern Sub-Saharan Africa, Central Asia, Eastern Europe, and the Middle East.3 Therefore, prevention and control of ischemic stroke is imperative. The most important preventive measure is to actively target the risk factors for stroke, which can significantly reduce the incidence and recurrence of ischemic stroke.
Transient ischemic attack (TIA) is a precursor to ischemic stroke characterized by symptoms typically resolving within one hour.4 Frequent episodes of TIA can precipitate ischemic stroke and are a common cause of cerebral small vessel disease.5 The 2021 American Heart Association and American Stroke Association guidelines for stroke prevention and the 2022 Chinese guidelines for secondary prevention of TIA provide a separate analysis of the risk factors for TIA.5,6 Hypothyroidism is a common endocrine and metabolic disorder caused by various factors that lead to insufficient synthesis, secretion, or biological effect of thyroid hormones (THs).7 This condition can be divided into 2 types: clinical hypothyroidism and subclinical hypothyroidism.7 Clinical hypothyroidism is characterized by elevated levels of thyroid-stimulating hormone (TSH) and decreased levels of serum free thyroxine (FT4), whereas subclinical hypothyroidism is characterized by elevated TSH levels with normal FT4 levels.7 Several studies have indicated that hypothyroidism may affect the functional prognosis of patients with ischemic stroke.8,9
However, neither set of the above guidelines elaborates on studies concerning TIA and hypothyroidism. This gap suggests that research exploring the relationship between TIA and hypothyroidism stays in its initial stages. This study aims to investigate the relationship between hypothyroidism and TIA and to determine whether hypothyroidism is a risk factor for TIA.
Methods
A literature search was carried out in PubMed, Cochrane, Embase, Vipers database (VIP), China Biomedical Literature Database (CBM), Wanfang database, and China Knowledge Network (CNKI) before May 2024. The Chinese database search terms included: (transient ischemic attack, cerebral infarction, or ischemic stroke) and (hypothyroidism, clinical hypothyroidism, or subclinical hypothyroidism). The English search terms included (autoimmune thyroiditis OR thyroiditis, autoimmune OR hypothyroidism OR thyroid deficiency OR thyroidectomy) AND (transient ischemic OR ischemic attack transient OR transient ischemic attack OR stroke). The search strategy employed subject terms combined with free words. The inclusion criteria were: i) randomized controlled trials, relevant cross-sectional surveys, or cohort studies; ii) investigating the relationship between hypothyroidism and TIA in adult patients; iii) results reported as odds ratio (OR), relative risk (RR), or comparable incidence or prevalence rates; and iv) English or Chinese publications. The exclusion criteria were: i) conference papers, abstracts, and letters to the editor; ii) data like the exact number of patients with TIA or hypothyroidism cannot be extracted; ii) duplicate publications; and iv) animal studies.
Two researchers independently screened the retrieved articles and carried out quality evaluation using EndNote X9 management software (USA, 1998-2020 Clarivate Analytics). Any disagreement between the 2 researchers was resolved by involving a third researcher. The Newcastle-Ottawa scale was used to assess the quality of cohort studies, whereas the Agency for Healthcare Research and Quality checklist was used to evaluate the quality of cross-sectional studies using reference.10,11 Only high-quality studies with scores more than 6 were included in the meta-analysis.
Statistical analysis
Review Manager 5.3 software (Copenhagen, Denmark) and Stata 17.0 software (Stata Corporation, College Station, Texas, USA) were used for analysis. Relative risk was calculated for categorical variables, and standardized mean difference was computed for continuous variables. A p-value of <0.05 was considered a statistically significant difference. Heterogeneity among the studies was assessed using quantitative methods and a Q-test with a p-value of>0.05, indicating no significant heterogeneity. An I2<50% indicated no significant heterogeneity, and a fixed-effects model was used for meta-analysis. When I2>50%, a random-effects model was used. Publication bias was assessed using funnel plots.
Results
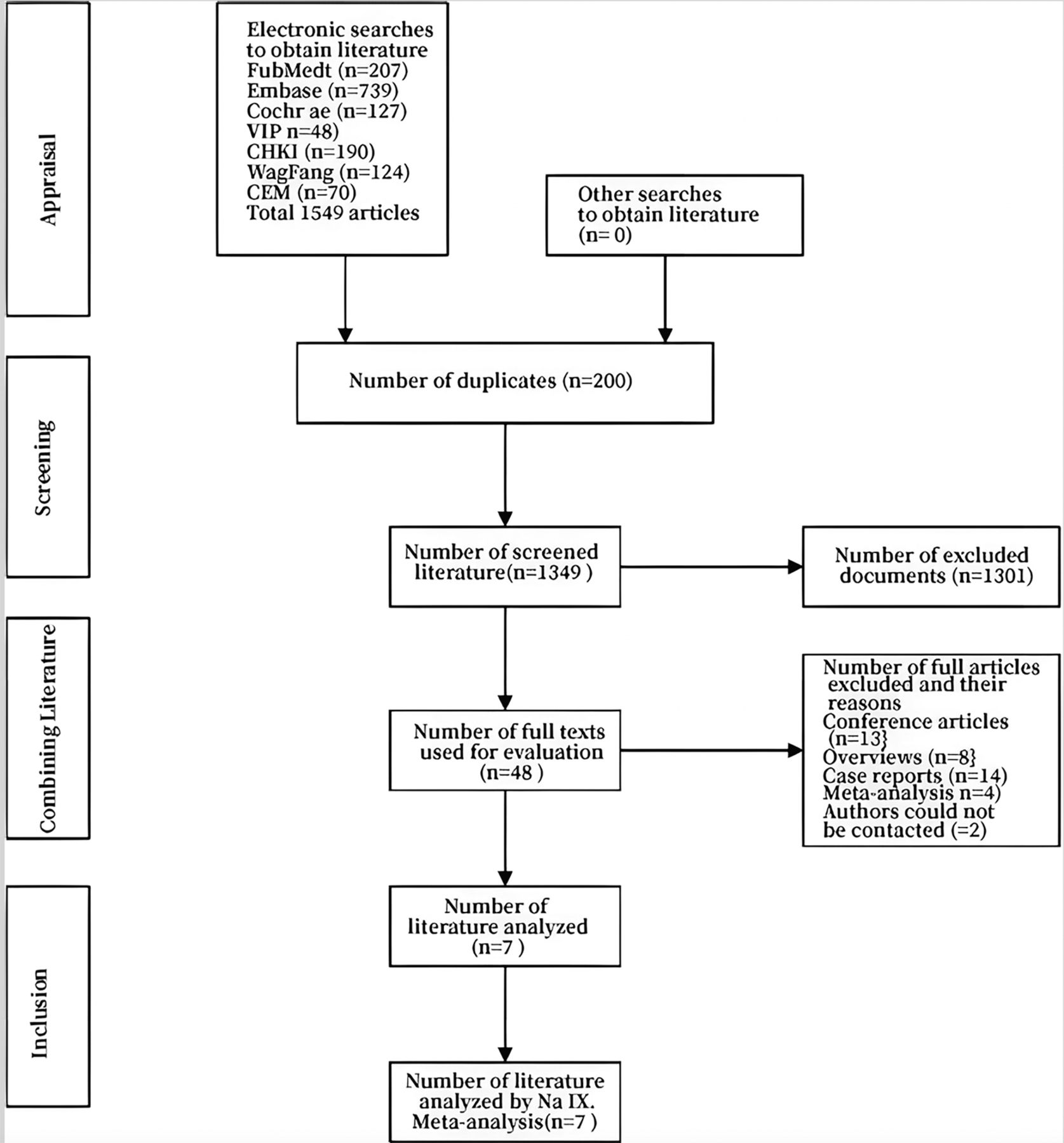
Figure 1 shows the literature search and screening process. Initially, 1549 articles were identified through database searches. Following computerized and manual deduplication, 1349 articles remained. Of these, 1341 were excluded after thoroughly screening titles and abstracts. The remaining 48 articles underwent full-text review. Subsequently, 41 articles were excluded as these were conference papers, reviews, case reports, meta-analyses, or articles with incomplete information for which the authors could not be contacted. Finally, 7 studies were included in the meta-analysis.12-18

- Schematic illustration of literature search and screening process.
Quality evaluation
The primary characteristics of the 7 studies are summarized in Table 1. The studies were carried out in developed countries such as Italy, Germany, Turkey, the United Kingdom, the United States, and Denmark. Two of the studies were cross-sectional surveys with quality scores of 6-9, and the remaining 5 were cohort studies with a total population of 190,248 patients, with quality scores of 6-9.
- Basic characteristics of the included studies.
Meta-analysis of clinical hypothyroidism and TIA
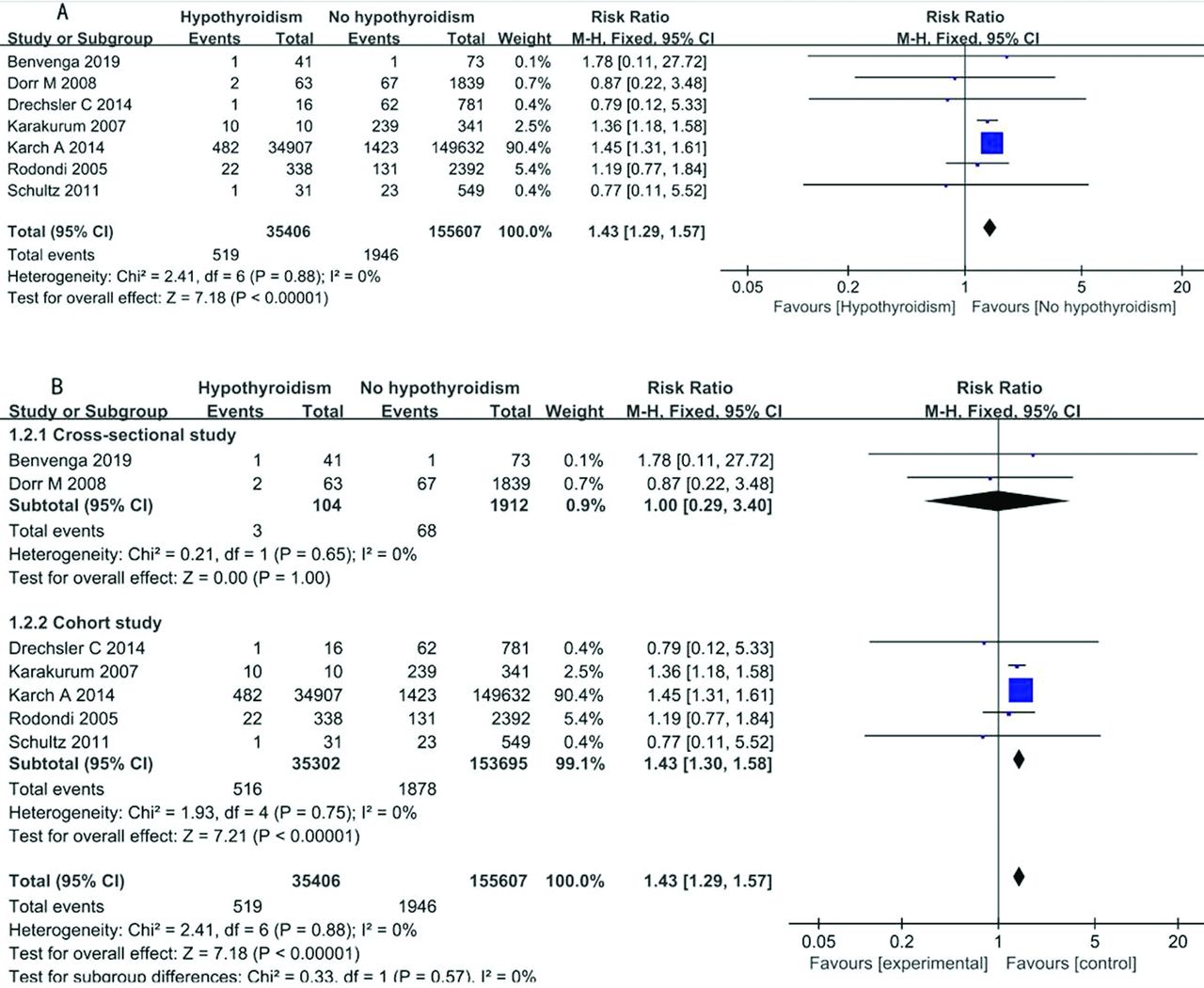
Seven studies were finally included, combined, and analyzed separately according to the study design using a fixed-effects model (Figure 2). The exposure factor was 35,406 patients with hypothyroidism, including 519 (1.47%) patients with concomitant TIA, and 155,607 patients in the control group, including 1,946 (1.25%) patients with concomitant TIA, with a combined RR value of 1.43 (95% CI: [1.29-1.57], I2=0%, p<0.01; Figure 2A). When the studies were divided by study types, the combined RR value was 1.00 (95% CI: [0.29-3.40], I2=0%, p=1.00) in cross-sectional study subgroup with 2 studies and the combined RR value was 1.43 (95% CI: [1.30-1.58], I2=0%, p<0.01) in cohort study subgroup with 5 studies (Figure 2B).

Meta-analysis of clinical or subclinical hypothyroidism and TIA
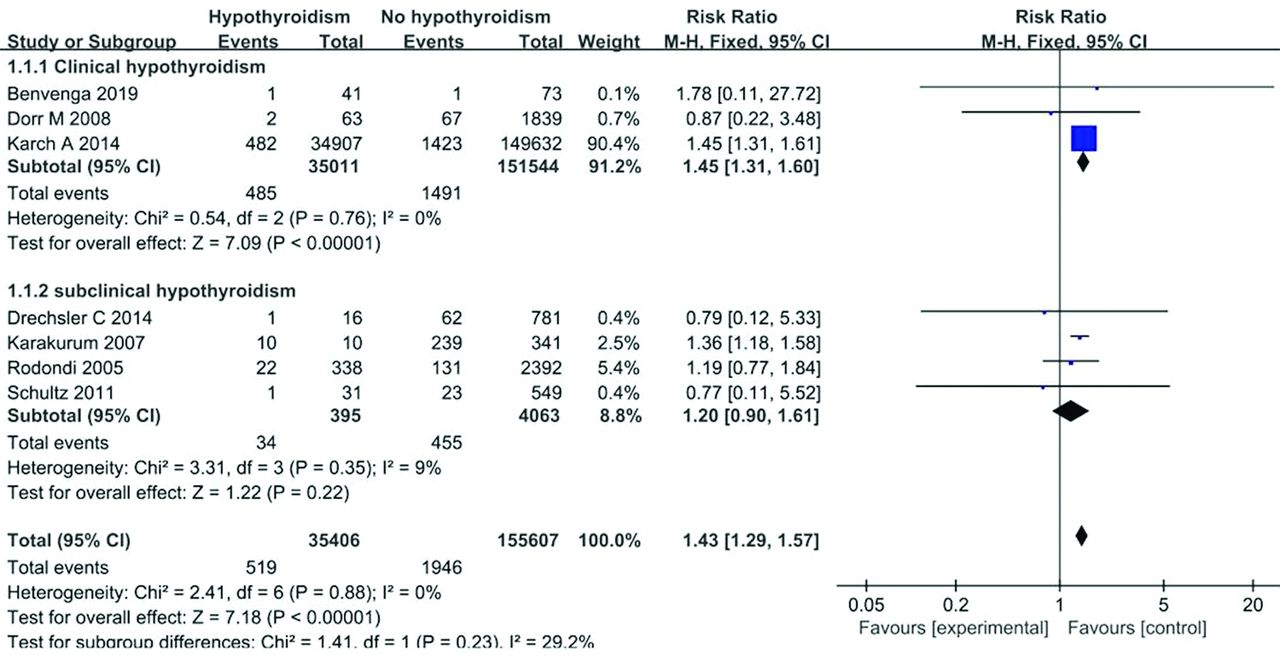
Hypothyroidism is categorized into 2 types: clinical hypothyroidism and subclinical hypothyroidism. Therefore, the studies were further divided into clinical hypothyroidism and subclinical hypothyroidism subgroups by disease type. A total of 4 studies were in the subclinical hypothyroidism group, and 3 were in the hypothyroidism group. The exposure factor was clinical hypothyroidism in 35,011 patients, of which 499 (1.43%) developed TIA, and 151,544 patients in the control group, of which 1,491 (1%) experienced TIA, with a combined RR value of 1.45 (95% CI: [1.31-1.62], I2=0%, p<0.01; Figure 3). The exposure factor was subclinical hypothyroidism in 395 patients, of which 34 (8.61%) developed TIA, and 4063 patients in the control group, of which 455 (11.2%) experienced TIA, with a combined RR value of 1.20 (95% CI: [0.90-1.61], I2=0%, p=0.22; Figure 3).

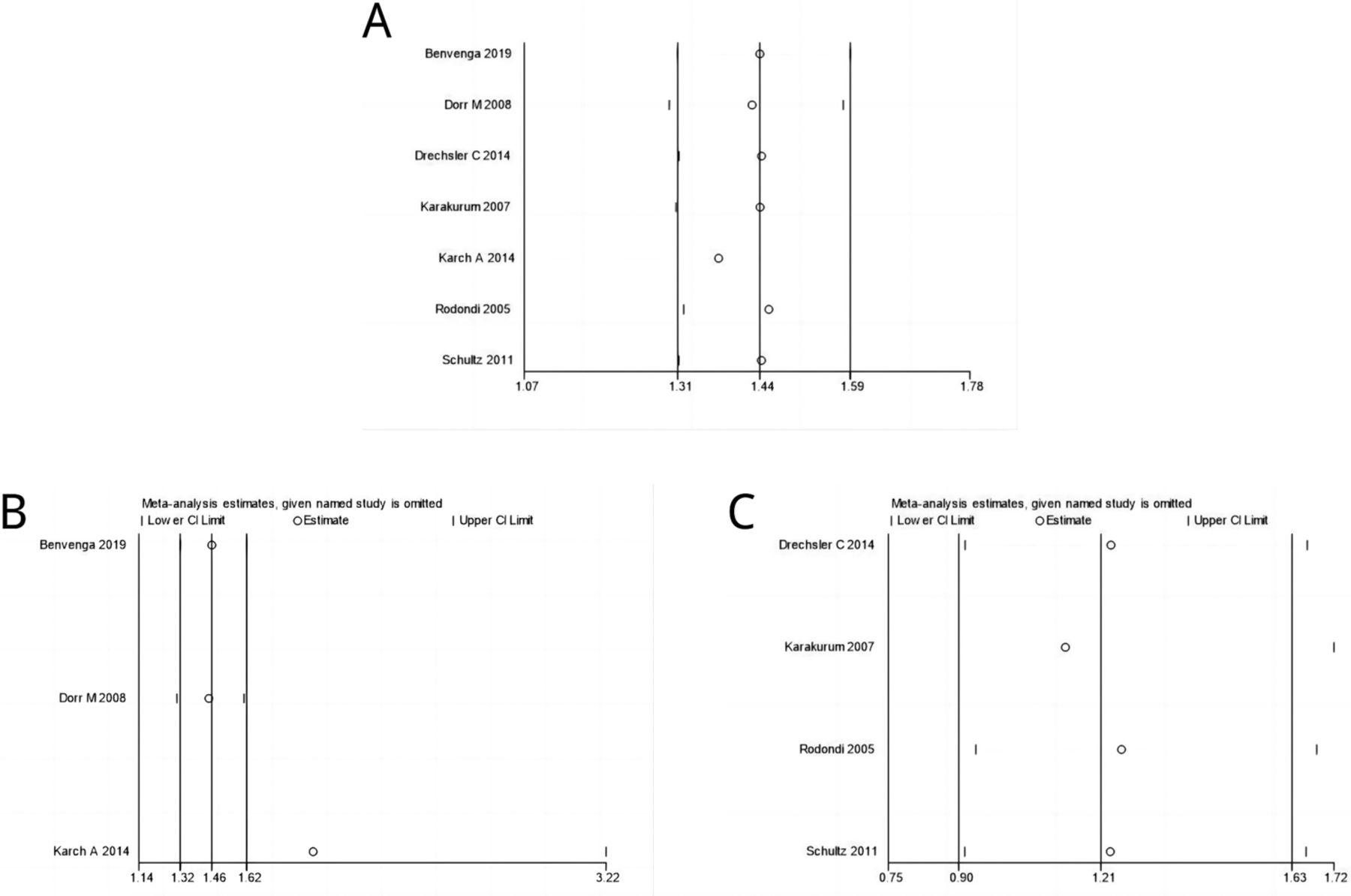
Sensitivity analysis and assessment of publication bias
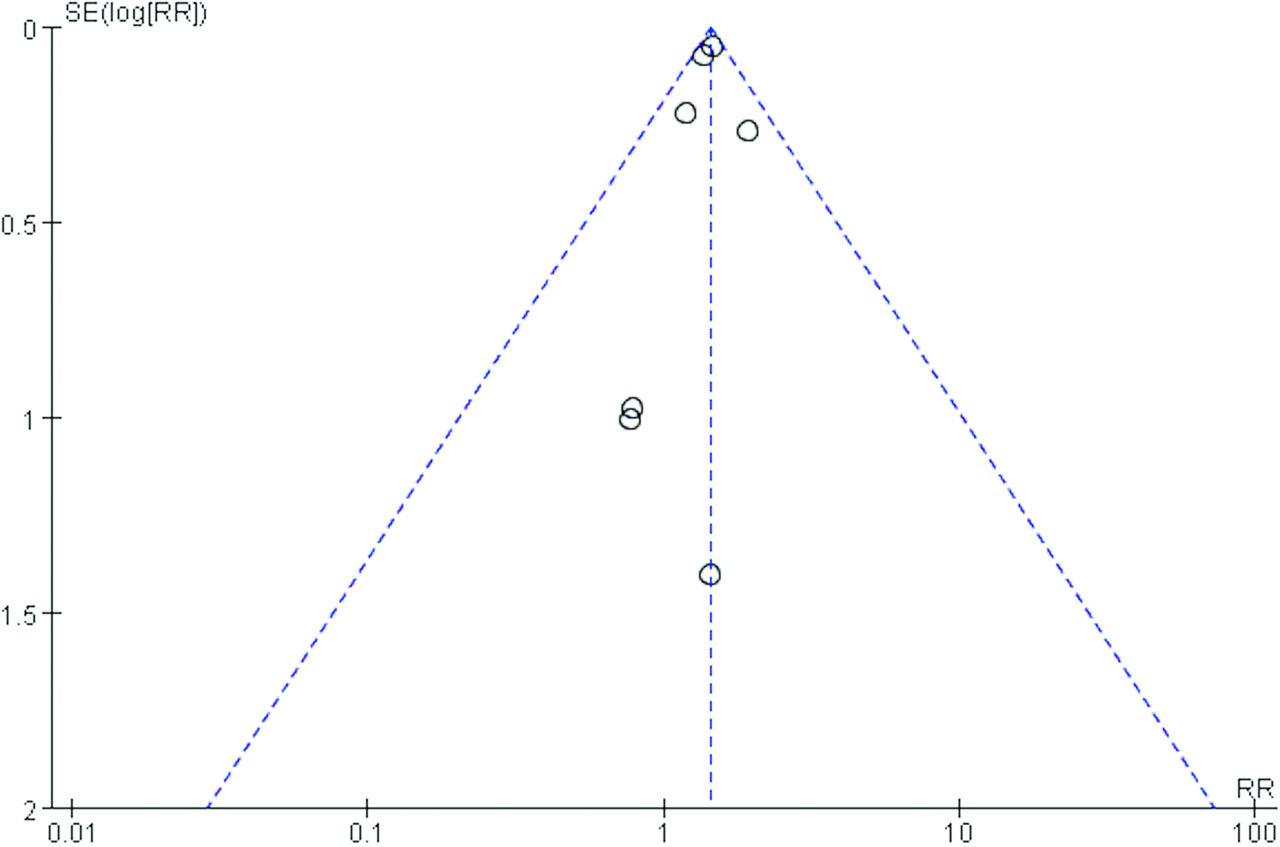
Sensitivity analysis was carried out by repeating the meta-analysis after the sequential exclusion of one study at a time. The results showed no significant change in the combined effect size after excluding any individual study (Figure 4). The funnel plot suggested a minimal effect of potential publication bias on the meta-analysis results (Figure 5).


- Publication bias funnel plot.
Discussion
In this meta-analysis, hypothyroidism was a risk for TIA, with a combined RR value of 1.43. It showed an association in cohort studies but not in cross-sectional studies. Moreover, further subgroup analysis revealed that clinical hypothyroidism was a risk for TIA, but subclinical hypothyroidism was not a risk for TIA. All meta-analyses showed an I2-value of 0%, indicating the low heterogeneity among the included studies.
Several studies have demonstrated that TIA is an independent risk factor for ischemic stroke.19-22 Interventions to alleviate the risk factors for TIA can help reduce the incidence of ischemic stroke. There is a partial overlap between the risk factors for TIA and ischemic stroke.23,24 For example, hypertension, diabetes mellitus, and smoking are risk factors for both conditions. However, there is a paucity of studies investigating risk factors specifically for TIA. Hypothyroidism is a common endocrine disorder that refers to insufficient production of THs. Evidence has shown that THs are pivotal in developing the nervous system and the physiological brain maturation.1 Studies have linked hypothyroidism to an elevated risk of stroke-related conditions. Remmel et al25 found that in patients diagnosed with AIS or TIA, the prevalence of hyperhomocysteinemia was significantly higher in patients with hypothyroidism (45.4%) compared to those with normal thyroid function (27.8%). In the present study, despite the large cohort, a small number of TIA cases were observed in centers with large and moderate sample sizes. Notably, even with this limited number of TIA cases, a significant proportion was associated with hypothyroidism, underscoring its substantial influence on TIA occurrence. The study revealed a higher incidence of TIA in patients with hypothyroidism compared to those without it. We hypothesize that the mechanism by which hypothyroidism affects TIA may parallel its impact on ischemic stroke. We found this association in 5 cohort studies but not in 2 cross-sectional studies, potentially because of the infrequent occurrence of hypothyroidism among the TIA population of the included cross-sectional studies. In fact, there were only 3 events in the TIA population of included cross-sectional studies. Future cross-sectional studies investigating this project should be carried out with more events.
Our study found that clinical hypothyroidism, but not subclinical hypothyroidism, was a risk for TIA. Studies have shown that clinical hypothyroidism can affect the central nervous system’s regulation of blood pressure, blood glucose, blood lipids, and other related physical functions, which exacerbates the risk of hypertension, hyperglycemia, and hyperlipidemia in clinical hypothyroidism patients.26 Moreover, hypothyroidism increases the occurrence of ischemic stroke and aggravates oxidative stress damage and calcium overload after cerebral ischemia, triggering inflammatory cascades and adversely affecting the prognosis of ischemic stroke.27 The main difference in THs between hypothyroidism and subclinical hypothyroidism is the levels of FT4, which are normal in subclinical hypothyroidism but reduced in hypothyroidism.7 Evidence has demonstrated the beneficial effects of T4 in mitigating neuronal injury, reducing the volume of cerebral infarction post-stroke, and dampening the expression of inflammatory genes. Furthermore, it also seems to enhance neuronal survival and neurogenesis.1 Our data showed that subclinical hypothyroidism was not a risk for TIA, partially because of the normal FT4 levels in subclinical hypothyroidism. Notably, this result was drawn from only 3 studies with a smaller sample size (only 34 events compared to 485 events in the hypothyroidism subgroup). Further studies are needed to confirm this.
Study limitations
First, this was a study-level meta-analysis with a greater risk of bias. Second, one study included 34907 individuals in the experimental group and 149632 individuals in the control group, whereas other studies only included individuals less than 500 individuals in the experimental groups.16 The Karch’s study contributed 90.4% to the total results. Therefore, more studies with large samples are required to validate our conclusions. Moreover, there is a need to carry out similar studies in China, which has the highest stroke burden in the world. Finally, research on the underlying mechanisms connecting hypothyroidism and TIA is imperative.
In conclusion, hypothyroidism may be an independent risk factor for TIA. Clinical but not subclinical hypothyroidism is a significant risk factor for TIA, possibly due to the combined effect of elevated TSH and decreased FT4 levels. Thyroid hormones should be monitored for subclinical hypothyroidism patients.
Acknowledgment
The authors gratefully acknowledge Medlive Inc. (www.medlive.cn) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 12, 2024.
- Accepted December 18, 2024.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.