


Abstract
Objectives: To translate the topical corticosteroid phobia (TOPICOP) scale into Arabic and assess its validity, reliability, and feasibility.
Methods: A cross-sectional study was carried out at Jordan University Hospital, Amman, Jordan, in 2 phases. Phase one involved translation of the TOPICOP scale into Arabic using a 2-step process, followed by pilot testing and content validation by 6 bilingual dermatologists. Phase 2 involved subsequent validation and feasibility testing on a larger sample of 145 participants. To assess reliability, the scale was administered twice for test-retest analysis.
Results: Calculated content validity indices revealed satisfactory values, establishing content validation of the Arabic version. Cronbach’s alpha coefficient indicated reliable internal consistency (0.757). Test-retest reliability yielded a Pearson’s correlation coefficient of 0.775 (p<0.001). The mean global TOPICOP score was 56.4%. The scale was clear, feasible, and completed in under 5 minutes without difficulty.
Conclusion: The Arabic TOPICOP scale is a valid, reliable, and effective tool for assessing corticosteroid phobia in Arabic-speaking populations. Its implementation can enhance understanding of patient adherence and improve eczema treatment outcomes, benefiting healthcare providers, including dermatologists, general practitioners, and family physicians.
Atopic dermatitis (AD) is a chronic inflammatory skin disorder that is linked to other atopic conditions such as asthma, allergic rhinitis, and food allergies.1 It imposes a multidimensional disease burden and significantly impacts the quality of life of both patients and their caregivers, especially in developing countries.2
Atopic dermatitis is a growing public health concern in Arabic-speaking regions, with studies in the Middle East and North Africa (MENA) estimating a prevalence of AD ranging from 3.6-19.8% in large population studies, mirroring global trends.3 Treatment of AD varies depending on disease severity, but topical corticosteroids (TCS) remain the cornerstone of therapy for managing AD flares and are also employed prophylactically to prevent exacerbations.4
Topical corticosteroids phobia is a widely recognized phenomenon, with a prevalence ranging from 31-95.7% in Asia, Europe, and North America.5 It is also prevalent in Arabic-speaking countries as a study in Saudi Arabia revealed that 66.6% of caregivers of pediatric AD patients exhibited TCS phobia, which is higher than the 40.3% reported in a similar Japanese study.6,7
The main reasons for TCS phobia include improper use, fear of side effects, negative experiences with TCS, lack of education from healthcare providers, and disruption of consistent clinic care.5 Unique cultural factors, such as a preference for traditional medicine and skepticism toward pharmaceuticals may also influence the worldwide disparity in the prevalence of TCS phobia. Moreover, socioeconomic status, the disparities in access to specialized dermatological care, and the reliance on less reliable sources of information on TCS can lead to inconsistent education regarding TCS safety and ultimately increasing the likelihood of fear-driven nonadherence.5,8
Topical corticosteroid phobia negatively impacts treatment adherence, which can lead to poor disease control.9 In Japan, 57.7% of caregivers with TCS phobia reported a history of non-adherence to TCS.10 Poor disease control, as seen in a Saudi study, also compromises quality of life through chronic itching, low mood, and sleep disturbances.11 Patient education can play an important role to address the factors leading to TCS phobia and ultimately improve treatment adherence.12 However, to tackle these factors, an assessment of the extent of TCS phobia in Arabic-speaking populations is needed first.
The topical corticosteroid phobia (TOPICOP) scale, a 12-item questionnaire, was designed to measure TCS phobia among adults and parents of children with AD.13 It is recognized as a valid and reliable tool and has been used globally to evaluate the prevalence of TCS phobia, potentially contributing to improving patient adherence and treatment outcomes.14,15
The TOPICOP scale has been validated in French, English, Japanese, and Thai, but an Arabic version is not yet available.13,16,17 However, adapting such scales for use in different languages and cultural contexts requires translation, cross-cultural adaptation, and validation.18
Adapting the TOPICOP scale into Arabic will help assess the scale of TCS phobia prevalence in Arabic-speaking populations, enabling targeted interventions and tailored education with resultant improved outcomes. This study aims to translate and adapt the TOPICOP scale into Arabic and assess its validity, reliability, and feasibility for use in Arabic speaking populations.
Methods
This study was carried out in 2 main phases. The first phase focused on translating the questionnaire into Arabic, followed by pilot testing and content validation to ensure linguistic and cultural appropriateness. The second phase involved assessing the validity, reliability, and feasibility of the Arabic version on a larger sample of participants through a cross-sectional observational design. Statistical analyses were used to evaluate content validity, internal consistency, and test-retest reliability, with ethical considerations upheld throughout the study.
This study complied with the principles of the Declaration of Helsinki. Written informed consent was collected from all individuals participating in the study, and personal identifiers were removed to maintain confidentiality. Ethical approval was granted by the institutional review board of Jordan University Hospital, University of Jordan, Amman, Jordan (certification No.: 10/2023/584).
Phase 2 involved subsequent validation and feasibility testing of the Arabic TOPICOP on a larger sample of participants. Data collection for this cross-sectional study design was carried out between October and December 2023. Eligible participants for inclusion included adult AD patients and parents of children under 15 years diagnosed with AD. Exclusion criteria were incomplete responses, inability to read Arabic, or cognitive/communication impairments. Following guidelines recommending a minimum respondent-to-item ratio of 5:1, a minimum of 60 participants was required for validation of the 12-item questionnaire.18
Medical records from the Dermatology Outpatient Clinic at Jordan University Hospital, Amman, Jordan (2017-2023) identified 440 eligible participants. These individuals were contacted via phone and invited to participate. A total of 145 participants consented to participate and completed a self-administered online questionnaire (via Google Forms).
Permission to translate the TOPICOP scale into Arabic was obtained from Professor Stalder, one of the original authors of the TOPICOP study.14 Phase one started with the translation process which was carried out by a professional translation center and involved 2 steps: initial translation of the English version by a bilingual translator and subsequent validation by an Arabic-speaking clinician to produce a preliminary Arabic version of the TOPICOP scale.
The questionnaire was composed of 5 main parts: I) an electronic informed consent form; II) general sociodemographic data; III) specific data regarding the disease and TCS; IV) the Arabic version of the TOPICOP scale; and V) clarity and feasibility of the questionnaire. To assess test-retest reliability of the TOPICOP scale, 96 of the participants completed part 4 of the questionnaire again after 2 weeks.
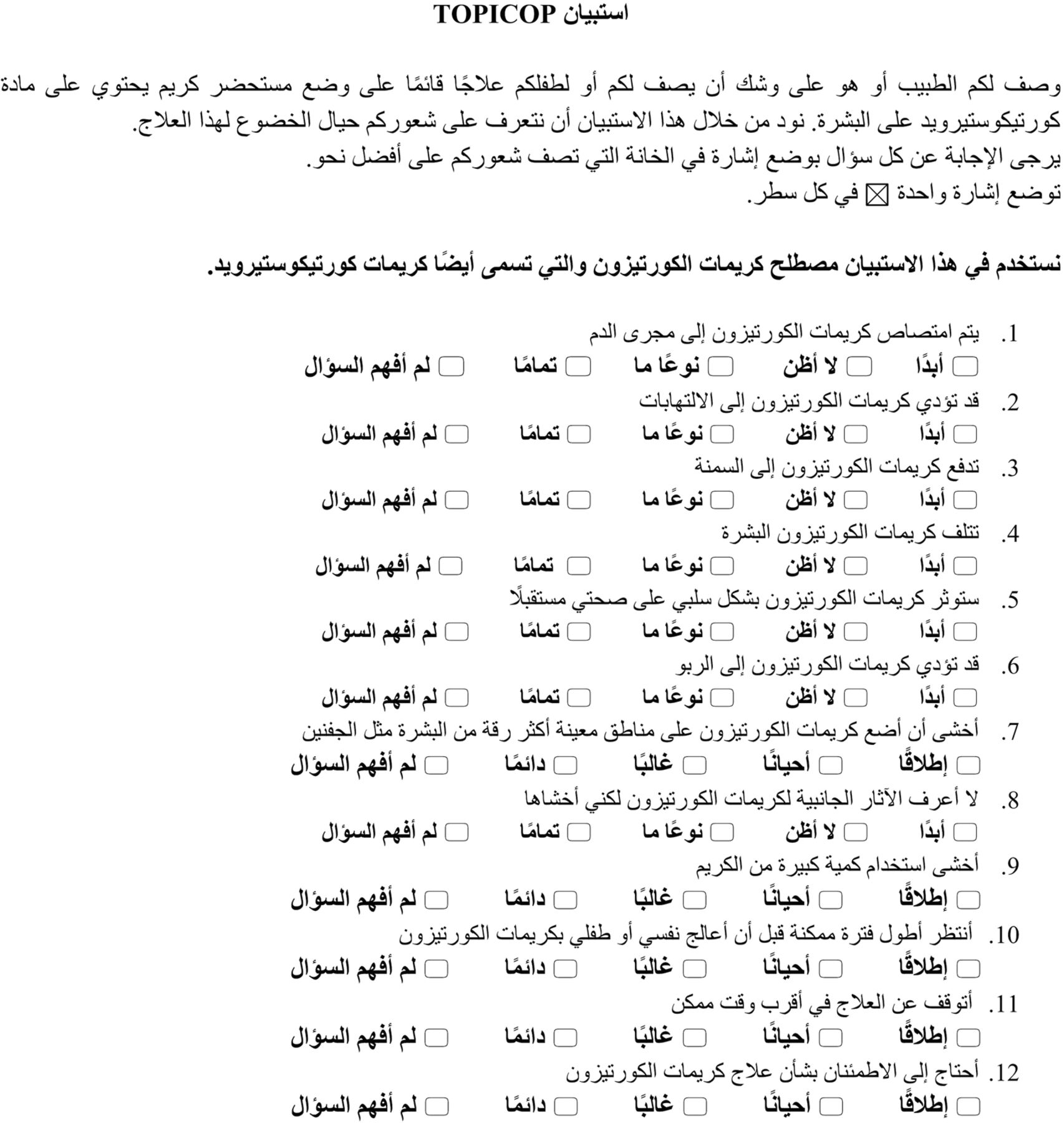
Regarding the study tool, The TOPICOP scale consists of 12 items grouped into 3 domains: knowledge and beliefs (items 1-6), fears (items 7-9), and behavior (items 10-12). Each item is rated on a 4-point Likert scale, with responses ranging from “totally disagree” to “totally agree” or “never” to “always,” corresponding to scores of 0-3. Higher scores indicate greater corticosteroid phobia.13
The TOPICOP score was calculated by summing all item scores, with a maximum of 36, expressed as a percentage for easier interpretation. Responses were included if participants answered at least half the items plus one within a domain. The mean score for a domain was the sum of the individual scores for that domain divided by the number of respondents. The TOPICOP scores range from 0-100.13
To ensure conceptual equivalence, a backward translation of the Arabic version was carried out by a bilingual translator unfamiliar with the questionnaire’s objectives. The original and back-translated versions were compared by the primary investigators for discrepancies. Adjustments were carried out based on pilot testing feedback, and the final version was approved by Professor Stalder.
Pilot testing was carried out to ensure participants comprehended the Arabic questionnaire. A total of 2 rounds of pilot testing were completed, each involving 20 participants (adult AD patients or parents of pediatric AD patients). Participants were asked open-ended questions to identify comprehension issues and were probed to assess their interpretation of the items, as suggested by published guidelines.18
In the first round, participants reported difficulties understanding items 1, 10, and 11. Item 1 (TCS absorption into bloodstream) was unclear, item 10 (waiting as long as possible before using TCS for myself or my child), and 11 (stopping the treatment as soon as possible) were confusing. Item 10 was misinterpreted as “I prefer to take corticosteroid treatment for the longest duration possible” instead of the intended meaning “waiting as long as I can before treating myself or my child.” Additionally, participants recommended replacing the abbreviation “TCS” with “cortisone creams” for clarity.
Following these recommendations, the questionnaire was revised and retested in a second pilot sample of 20 participants. No further difficulties were reported, confirming the clarity and comprehensibility of the final Arabic version of the TOPICOP scale (Figure 1).

- Arabic version of the topical corticosteroid phobia (TOPICOP©) questionnaire.
The Arabic TOPICOP scale then underwent content validation by 6 bilingual dermatologists using the content validation index (CVI) form. Items were scored on a 4-point scale, where 1 indicated irrelevance and 4 indicated high relevance. Scores of 3 or 4 were regrouped as 1, and scores of 1 or 2 were regrouped as 0. The CVI included item-level CVI (I-CVI), scale-level CVI using the average method (S-CVI/Ave), and scale-level CVI using the universal agreement method (S-CVI/UA). An acceptable CVI threshold of ≥0.83 was used for 6 evaluators.19 All I-CVI values met this benchmark, with S-CVI/Ave value of 0.97 and S-CVI/UA value of 0.83.
Statistical analysis
Microsoft Excel was used to enter the data and then analyzed using the statistical Package for the Social Sciences statistics for Windows, version 21.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were reported as frequencies and percentages. Content validity was assessed using CVI calculations. Reliability was assessed using internal consistency (Cronbach’s α). Test-retest reliability was evaluated by calculating the Pearson correlation coefficient (r) based on responses after a 2-week interval. A p-value of <0.05 was considered significant.
Results
The study included 145 participants, of whom 99 were parents of children with AD and 46 were adult patients with AD. The sociodemographic data of the participants are shown in Table 1. The mean age across all participants was 35.6±12.0 years, with parents averaging 40.4±7.5 years, children with AD averaging 8.2±3.8 years, and adult patients with AD averaging 25.2±13.3 years. Males comprised 54.5% of participants, the majority (64.8%) resided in the capital Amman, Jordan, held a bachelor’s degree or higher (57.9%), and reported a family income between 200-2,000 Jordanian dinar (89.7%).
- Socio-demographic data.
Specific data regarding AD and disease characteristics are shown in Table 2. More than a third (37.9%) of the patients had a family history of AD, and nearly half (43.5%) had other atopic disorders. More than four-fifths (83.4%) of the patients had used TCS recently or in the past. The duration of TCS use varied among the patients. Approximately 55% of participants reported having TCS phobia when asked a yes or no question, and 83.7% of those reported concerns regarding side effects as the main reason for such fears. Dermatologists were the main source of knowledge regarding TCS in 55.9% of participants (followed by social media, with 15.2%, and then family and friends, with 13.1%).
- Specific data regarding atopic dermatitis and disease characteristics (N=145).
The reliability of the Arabic version of the TOPICOP© questionnaire was assessed using internal consistency and test-retest methods. For internal consistency, Cronbach’s alpha coefficient was 0.757. Cronbach’s alpha did not increase if any of the 12 items were deleted. Test-retest methods showed a Pearson correlation coefficient of 0.775 (p<0.001) between the 2 scores obtained at a 2-week interval.
The global TOPICOP score, subscores for the domains, and detailed responses for the Arabic version of the TOPICOP© questionnaire are presented in Table 3. The mean global TOPICOP score was 56.4±16.5. The mean global TOPICOP score for parents of pediatric patients with AD was 59.1±16.1 and adult patients score was 50.4±16.1. The participants who reported no TCS phobia had a mean global TOPICOP score of 46.0±14.6. Regarding domain subscores, the fears domain was the most dominant (63.4%), followed by behavior (62.6%), and knowledge (49.4%) domains.
- Responses and scores for the Arabic version of topical corticosteroid phobia (TOPICOP©) scale items.
The most common concerns regarding TCS were related to areas of application, such as the eyelids (73.8% often/always), and too much application of TCS (67.6% often/always). The majority of the participants were fearful of using TCS while not knowing the side effects (67.6% almost/totally agreed), and most needed reassurance regarding TCS (73.8% often/always). A total of 33 (22.8%) participants did not understand some of the items given, with the highest percentage (13.8%) found for item 1 (TCS can be absorbed into the bloodstream).
The difficulty in answering each item on the Arabic version of the TOPICOP© scale was evaluated with a 4-point Likert scale, ranging from “not at all difficult” to “extremely difficult” (Table 4). Most participants found the items easy to answer, with 48-77% considering them “not at all difficult.” Notably, 14-34% found the knowledge/belief domain items quite or extremely difficult. The top 3 difficult-to-answer items were item 1 (TCS absorption into bloodstream) accounting for 33.8%, item 2 (TCS causing infections) accounting for 26.2%, and item 6 (TCS leading to asthma) accounting for 24.2% of the participants. Conversely, behavior-domain items were the easiest, with 73-77% reporting them as “not at all difficult” and only 6-12% finding them quite or extremely difficult. Overall, only 18% found all 12 items combined quite or extremely difficult.
- Difficulty in answering each item of the Arabic version of topical corticosteroid phobia (TOPICOP©) questionnaire.
The clarity and feasibility of the Arabic version of the TOPICOP© questionnaire was assessed using 5 questions, which are presented in Table 5. Most of the participants (96.5%) reported that the TOPICOP questionnaire was clear or extremely clear, and 73.1% completed it in less than 5 minutes. The majority (82.1%) encountered no difficulty in completion. Additionally, 88.3% agreed that the questionnaire covered all aspects that might deter them from using TCS, while 85.5% expressed a willingness to use it for future follow-ups.
- Clarity and feasibility of the Arabic version of topical corticosteroid phobia (TOPICOP©) questionnaire (N=145).
Discussion
This study translated and cross-culturally adapted the TOPICOP scale into Arabic, along with an assessment of content validity, reliability, and feasibility.
The Arabic TOPICOP scale achieved high content validity meeting the minimum CVIs threshold of 0.83 needed to establish content validation (I-CVI; 0.83-1, S-CVI/Ave; 0.97, and S-CVI/UA; 0.83), confirming the appropriateness of its translation and adaptation.19 Reliability metrics (Cronbach’s alpha = 0.757, Pearson correlation coefficient = 0.775) demonstrated consistency and stability, aligning with previous studies.13,17,18 These findings affirm the scale’s robustness in evaluating TCS phobia in Arabic-speaking populations.
Stalder et al14 carried out an international feasibility study that reported a mean global TOPICOP score of 44.7% across 17 countries. The mean global TOPICOP score (56.4%) in Jordan was comparable to countries like Poland, Ukraine, and Thailand (ranging from 52.9-58.6%), indicating a shared degree of TCS phobia.14,17 However, it was higher than the international average reported by Stalder et al (44.7%).14 This suggests that Jordanians may have heightened apprehensions regarding TCS use, possibly due to cultural beliefs, misinformation or inadequate patient education.
Although the mean global TOPICOP score can be similar among different countries, the domain subscores may differ. For instance, both mean global TOPICOP scores in our study (56.4%) and in Poland (58.4%) were comparable.14 However, The fears domain emerged as the most dominant in Jordan, suggesting heightened anxiety around corticosteroid safety compared to the behavior-focused concerns in Poland. This could reflect cultural variations in trust toward medications or health literacy levels regarding TCS.
In our study, the mean global TOPICOP scores in parents of pediatric patients were higher (59.1%) than adult patients (50.4%), likely due to heightened concerns for children’s safety. Parents may overestimate risks associated with TCS use for their children, leading to higher phobia levels. The mean global scores for parents of pediatric patients in our study (59.1%) were higher than those reported in a Japanese study for caregivers of pediatric patients (40.3%) but lower than those found in a study carried out in Saudi Arabia (66.6%).6,7
Notably, 16.6% of participants reported no explicit fears regarding TCS yet had elevated mean global TOPICOP scores (46%). This discrepancy highlights latent TCS phobia in patients or caretakers that may not be immediately evident but could still impair adherence. The TOPICOP scale thus proves valuable in identifying subtle forms of phobia requiring intervention.
Regarding difficulty in answering the TOPICOP scale questions, the knowledge and beliefs domain posed the most difficulty, particularly items related to systemic absorption, infection risks, and links to asthma; item 1 (TCS absorption into bloodstream), item 2 (TCS causing infections), and item 6 (TCS leading to asthma). These misconceptions were also observed in other studies and among healthcare providers, indicating widespread misinformation regarding TCS.14,20,21 This domain’s complexity underlines the importance for targeted educational efforts to resolve specific misunderstandings and improve treatment adherence.
The scale was perceived as clear and easy to complete, with 96.5% of participants expressing satisfaction and most completing it within 5 minutes. This is similar to the other translated versions of the TOPICOP scale.14,16,17 Its ease of use makes it a practical tool for routine clinical assessment, enabling healthcare providers to identify and address TCS phobia effectively.
Study limitations
While the study successfully validated the Arabic TOPICOP scale, limitations include its single-center design and limited sample size restricting generalizability. The absence of a comparable scale precluded construct validity assessment, though this may not be critical given the thorough translation and adaptation process.22,23 Furthermore, carrying out factor analysis is recommended to ascertain the suitability of the scale’s 3-factor model.
Future studies with larger, multi-center samples are needed to: I) explore the prevalence of TCS phobia in Arabic-speaking populations. II) Investigate the influence of demographic and psychosocial factors on domain scores. III) Develop interventions addressing specific educational needs identified through TOPICOP scores.
In conclusion, corticosteroid phobia remains a significant barrier to optimal AD management, with tangible consequences for both patients and healthcare systems. By incorporating validated tools like the TOPICOP scale and investing in patient education, healthcare providers such as dermatologists and general practitioners can address these fears, improve treatment adherence, and ultimately enhance patient outcomes. Efforts to culturally adapt and validate the scale, such as translating it into Arabic, are essential for expanding its utility across diverse populations.
Acknowledgment
The authors gratefully acknowledge Prof. Jean-François Stalder, Prof. Emeritus, and Mr. David Troya, SCORAD/TOPICOP Licensing Manager, from the Department of Dermatology at Nantes University Hospital, France, for granting permission to translate TOPICOP© into the Arabic language. The authors also would like to thank Dr. Salah A. Abdallat, Dr. Rand Murshidi, Dr. Mai Albsoul, Dr. Salsabiela Bani Hamad, and Dr. Zain Al Ta’ani for the content validation of the Arabic version. Additionally, They would like to thank Scribendi (www.scribendi) for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 28, 2024.
- Accepted February 4, 2025.
- Copyright: © Saudi Medical Journal
This is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.