


Abstract
Intestinal lymphangiectasia (IL) is a rare disease characterized by dilatation of intestinal lymphatics. It can be classified as primary or secondary according to the underlying etiology. The clinical presentations of IL are pitting edema, chylous ascites, pleural effusion, acute appendicitis, diarrhea, lymphocytopenia, malabsorption, and intestinal obstruction. The diagnosis is made by intestinal endoscopy and biopsies. Dietary modification is the mainstay in the management of IL with a variable response. Here we report 2 patients with IL in Bahrain who showed positive response to dietary modification.
Intestinal lymphangiectasia (IL) is a rare1-4 benign disease characterized by focal or diffuse dilation of the mucosal, submucosal, and subserosal lymphatics.2,5 In addition to being an important cause of protein losing enteropathy (PLE),6 IL is frequently associated with extraintestinal lymphatic abnormalities.5 Depending on the underlying pathology IL can be classified as primary or secondary disease.1,2,4,5 Primary IL (PIL) probably represents a congenital disorder of mesenteric lymphatics.1,3 The IL can be secondary to diseases like constrictive pericarditis, lymphoma, sarcoidosis, and scleroderma.1 A secondary disorder should always be ruled out before labeling IL as primary, this is by testing for proteinuria, rheumatic, neoplastic, and parasitic infection.1,3 Recently, a functional form of PIL with typical endoscopic and pathological findings but without clinical symptoms has been reported.3 The clinical presentations of IL are pitting edema, chylous ascites, pleural effusion, acute appendicitis, diarrhea, lymphocytopenia, malabsorption, and intestinal obstruction.1,2,4 Palliative treatment with lifelong dietary modification is the most effective and widely prescribed therapy.6 Limiting the dietary fat intake reduces chyle flow and therefore, protein loss.1 Once protein level is within the normal range, recurrence of enteric protein loss can be prevented by total parenteral nutrition (TPN) and medium chain triglycerides (MCT).1 In cases of secondary IL, treating the underlying primary disorder may be curative.2 Although the therapeutic approach for this disorder have gained a lot of attention lately, few studies have considered the therapeutic effects, nutritional condition, and long-term results in PIL patients.4 Here, we report 2 patients with PIL who were diagnosed by endoscopy and biopsy, and showed positive response to dietary modifications. We present these particular cases to highlight the effect of dietary modifications on the clinical status of patients with IL.
Case Report
Patient 1
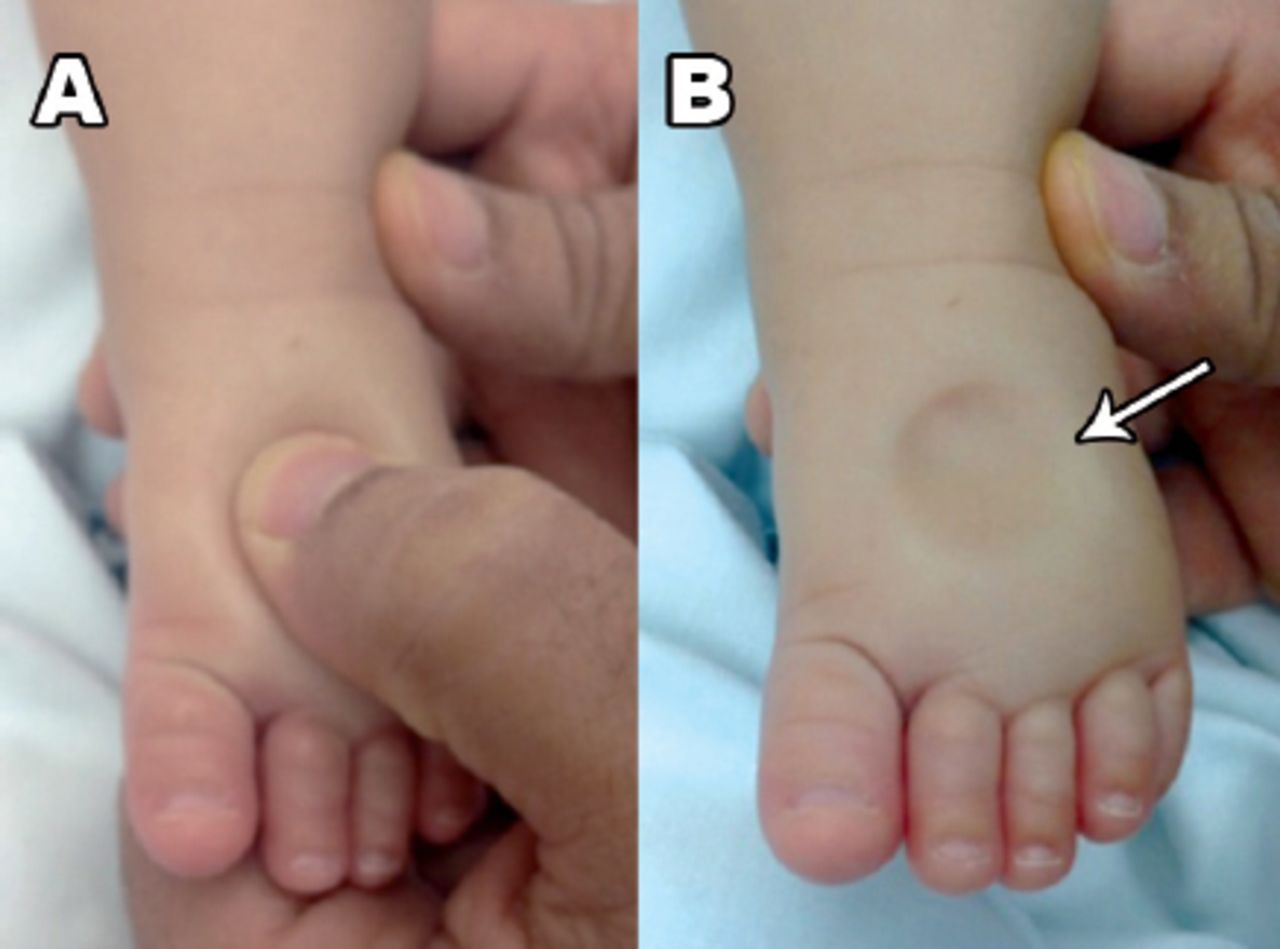
The first case was an 11-week-old male, a product of full term normal vaginal delivery with a birth weight of 3.6 kg. The parents are first-degree relatives. The pregnancy was complicated by gestational diabetes mellitus. He presented at the age of 2 months with a history of right lower limb edema and chronic diarrhea since birth. The right lower limb edema started soon after birth, associated with redness and warmth. Later on, the edema became generalized and noticeable on the face and both lower limbs (Figure 1). The diarrhea was up to 6 times per day, loose, non-greasy with no mucus or blood. There was mild abdominal distention. His feeding and activities were normal. Right lower limb cellulitis was suspected and treated with antibiotics. There was no history of recurrent infections, chronic, or genetic diseases in the family. Physical examination revealed right lower limb pitting edema but no redness or warmth. The abdomen and both testicles were mildly distended. His laboratory tests revealed low total serum protein, low serum albumin, low serum calcium, and high alkaline phosphatase. (Table 1).

A pitting edema (arrow): A) gentile pressure on the foot dorsum; and B) persistent skin depression in a 2-month-old infant with primary intestinal lymphangiectasia.
Laboratory data of 2 patients with primary intestinal lymphangiectasia.
Initial serum immunoglobulin E (IgE) <7.00 IU/ml (normal range: 11-162 IU/ml) and immunoglobulin G (IgG) 0.48 (normal range: 2-6.8 g/l) were low, while immunoglobulin A (IgA) and immunoglobulin M (IgM) levels were normal. Repeated total IgE was high but IgG remained low. Toxoplasma, others, Rubella, cytomegalovirus, and herpes simplex (TORCH) screen, and hepatitis profile were negative. The 24-hour urine for protein was negative. Serum cholesterol was low while serum triglycerides were normal. Allergy tests were negative. Stool microscopy was positive for fat globules but stool alpha 1 anti-trypsin was not performed. Thyroid stimulating hormone level (TSH) was high indicating subclinical hypothyroidism, which normalized on subsequent testing. Ultrasound abdomen was unremarkable. Upper gastrointestinal endoscopy showed normal esophagus mild diffuse gastritis, while first and second part of the duodenum showed prominent submucosal folds with whitish appearing villi throughout. Duodenal biopsies showed hugely dilated lymphatics in the lamina propria indicating intestinal lymphangiectasia. The patient was given albumin infusion with furosemide and started initially on amino-acids based formula (Elecare) followed by MCT based formula (Monogen), fat-soluble vitamins, multivitamins, oral iron, and calcium supplementations. The edema significantly improved and continued after 9 months of follow-up.
Patient 2
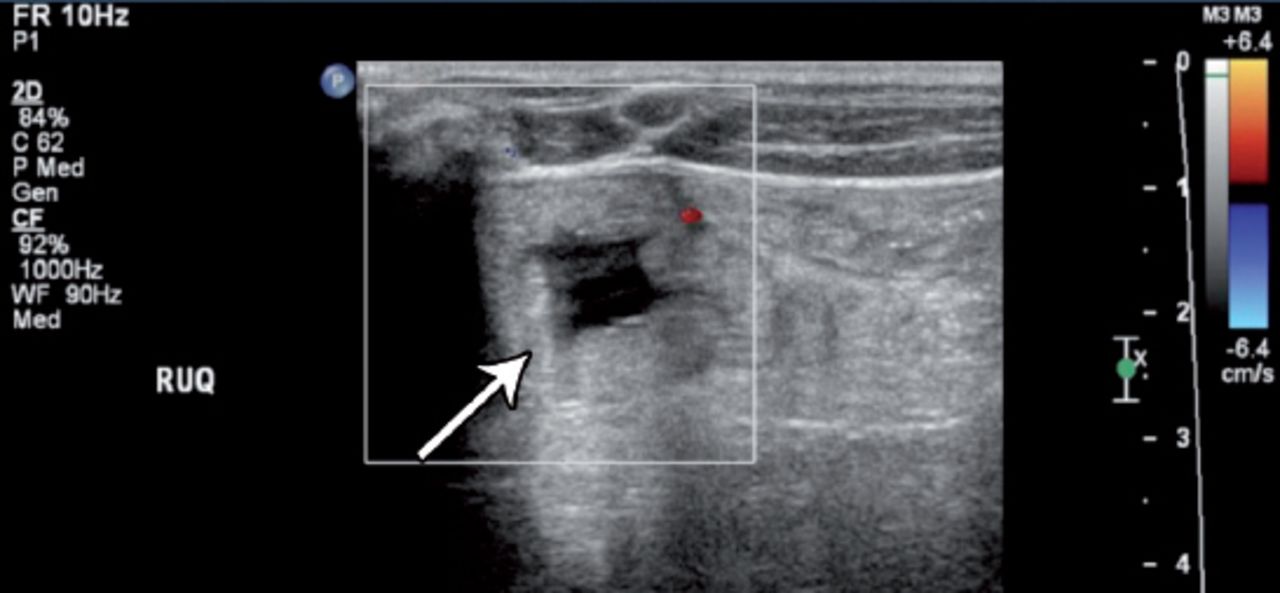
A 12-year-old male who was initially diagnosed as a case of mesenteric lipoma after a history of puffy eyes, scrotal swelling, and recurrent diarrhea of 2 months duration. The diarrhea was 3-4 times per day, loose with no mucous, blood, or steatorrhea. He had occasional mild abdominal pains not associated with vomiting, weight loss, or changes in appetite. He had a history of recurrent attacks of wheezing and shortness of breath, but no history of atopic conditions. He had no history of recent upper respiratory tract infections or urinary complaints. He was a product of a full term normal vaginal delivery with an Apgar score of 9 and 9 at one and 5 minutes. His birth weight was 2.9 kilograms. He had a right foot hypertrophy since birth. He was fully vaccinated. The parents are non-consanguineous, and they have 8 other siblings who are not suffering from any chronic or genetic diseases. At the age of 10 years, an abdominal mass was felt accidently, but he was reassured as his abdominal ultrasound (US) was unremarkable. On physical examination, he had course facial features but no dysmorphism. There was a bilateral pitting pedal edema more prominent on the right lower limb. His weight was 27 Kg and his height was 127 centimeters both on the 25th percentile. Abdominal examination revealed mobile, palpable masses in the left hypochondrial and lumbar region, a scrotal edema, and extensive multiple cutaneous warts on his genitalia. All other systems were normal including fundus examination. The laboratory work up (Table 1) revealed low serum total protein (44 g/L), low albumin (28 g/L), low globulin (17 g/L), and low serum cholesterol. His full blood count showed lymphopenia. Serum thyroid stimulating hormone level was high indicating subclinical hypothyroidism. Serum 25 hydroxycholecalciferol (30 nmol/l, normal >50) and serum calcium were low. Erythrocytes sedimentation rate, C-reactive protein, coagulation profile, liver enzymes, and renal function test were all within normal range. Human immunodeficiency virus (HIV) serology was negative. Urine and stool routine microscopy were normal. His abdominal US was reported as normal, although a retrospective review showed ‘a halo sign’ indicating thickened intestinal wall (Figure 2).

Right upper quadrant (RUQ) abdominal ultrasound of a 12-year-old child showing ‘a halo sign’ (arrow) indicating thickened intestinal wall secondary to primary intestinal lymphangiectasia.
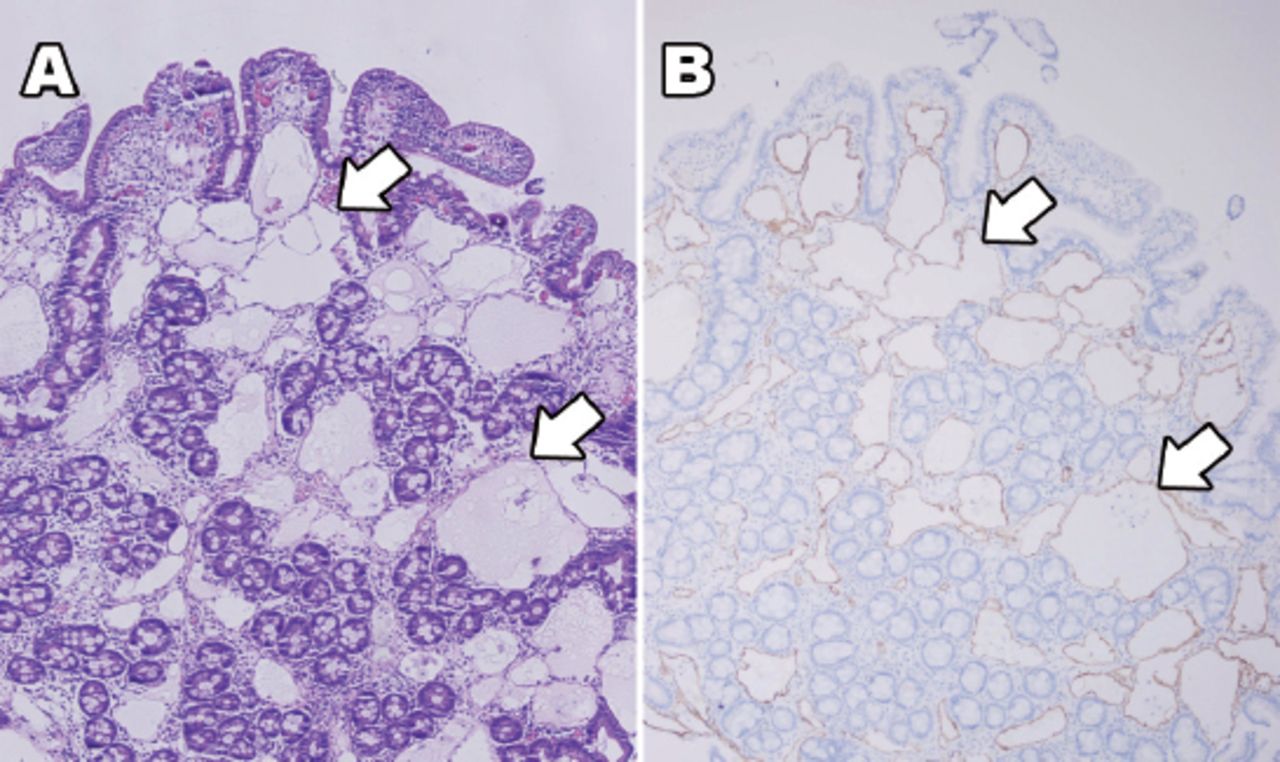
Abdominal CT scan showed a diffuse mass predominantly of fat density infiltrating the mesentery. Ultrasound guided fine needle biopsy of abdominal masses was negative for malignancy, and it revealed mature fibro-adipose tissue and benign peritoneal mesothelial cells. Barium meal and follow through showed thickened bowel wall with nodularity. Low red blood cells indices, low serum iron (5 umol/l, normal range 6-27), and low serum ferritin (36 µg/l, normal range 52-421) were consistent with iron deficiency anemia. While the patient was on his regular diet, stool alpha 1 anti-trypsin was elevated (normal value: 0-0.62 mg/g) indicating PLE. Upper gastrointestinal endoscopy showed creamy white dots covering the second part of duodenal mucosa. Colonoscopy showed nodular rectum, sigmoid, and ascending colon. Microscopic examination revealed hugely dilated lymphatics in the duodenal mucosa and submucosal (Figure 3).

Duodenal biopsy of a 12-year-old child showing hugely dilated lymphatics (arrows) in the lamina propria indicating intestinal lymphangiectasia; A) stained with Hematoxylin and Eosin ×10, and B) stained with D2-40 immunohistochemistry ×10).
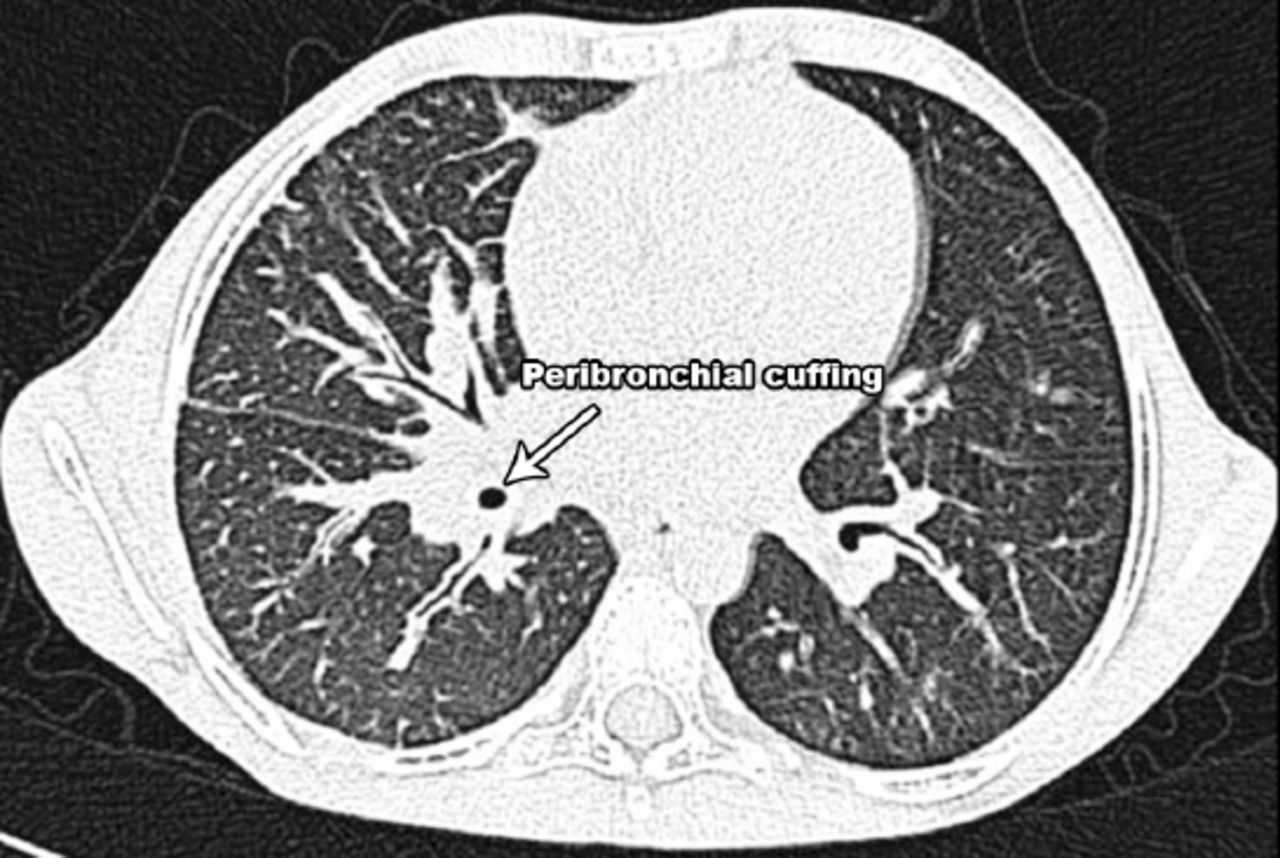
Lower esophagus biopsies showed chronic, non-specific esophagitis with no eosinophils. Gastric and rectal mucosa were normal. Helicobacter pylori test was negative. The patient was diagnosed with PIL. He was kept on low-fat, high protein diet along with MCT oil, fat-soluble vitamins, iron, and calcium supplements. In addition, he received nebulized salbutamol and pulmicort for his chest symptoms. On follow-up, the patient showed improvement. Three years later, the patient presented again with diarrhea, occasional colicky abdominal pain, chronic productive cough, and stammering speech. On examination, he had bilateral lower limb edema more on the right side and bilateral crepitations in his chest. A high-resolution chest CT scan showed thickening of central lung interstitium and interlobar septa, few small nodules with peri-lymphatic distribution, and central peribronchial cuffing. There were no hilar or mediastinal lymphadenopathy, and no pleural or pericardial effusion. These changes are consistent with pulmonary lymphangiectasia (Figure 4). The patient was managed with albumin infusion and diuretics. On follow-up, the patient improved but he was not adherent to the restricted diet.

High-resolution CT scan of the lung of a 12-year-old child with primary intestinal lymphangiectasia showing thickening of central lung interstitium and interlobar septa, and some small nodules with peri-lymphatic distribution. Peribronchial cuffing (arrow) is also seen centrally.
Ethical approval for this study was obtained from the Pediatric Department, Salmaniya Medical Complex, Bahrain.
Discussion
Congenital defects of the lymphatic system lead to a spectrum of disorders with a diversity of clinical presentations like lymphedema, chylous effusions, lymphangiomatous malformations with cystic masses, localized gigantism, and IL.2 Although lymphangiectasia is commonly seen in the head, neck, and axilla, it rarely involves intra-abdominal organs.2 The etiology behind PIL remains unknown.5-7 Hoopes et al7 studied genetic mutations correlated with IL in mice and found that certain gene mutations are associated with lymphatic dysfunction. Several genes are implicated in the development of lymphatic systems, for example VEGFR3 (vascular endothelial growth factor receptor 3), PROX1 (prospero-related homeobox-transcriptional factor) and FOXC2 (forkhead transcriptional factor).7 In this report, genetic testing for mutations was not performed due to the unavailability of the tests in our institute. However, the parents of the first patient are consanguineous and this might support the possibility of a genetic involvement. In contrast, 2 of the 4 cases reported by Suresh et al5 were products of non-consanguineous marriages.
The IL is characterized by obstruction and subsequent dilation of lymph vessels in the submucosa of the small bowel.1,6-8 Dilated vessels may leak chyle into the small bowel lumen, and occasionally into the peritoneal cavity and the pleural space, causing chylous effusions.8 Exudative enteropathy leads to lymphopenia, hypoalbuminemia, and low oncotic pressure, and so the patient may develop pitting edema.3,9 In addition, inability to absorb fat and fat-soluble vitamins results in hypocalcemia.1
The worldwide incidence and prevalence of IL is still unknown.1,8,9 There are inadequate number of cases to make a solid statement.6 Only few cases have been reported.8 Most of the present recommendations are provided from no more than 200 cases of PIL.6 There is no racial predilection.1 The IL can affect both male and female equally.1,2 Variable clinical presentations have been reported with IL. Primary intestinal lymphangiectasia usually presents in childhood and early adolescence.8 However, it can presents by 30 or 40 years of age.2,6 The PIL is usually presented with episodic abdominal pain, steatorrhea, peripheral edema, and ascites.5,6,8 Edema, hypoproteinemia, diarrhea, and lymphocytopenia are the main clinical presentations.2-4 The peripheral edema can be unilateral or bilateral.1 Peripheral edema may initially be intermittent, but eventually becomes constant.8 The edema can affect the macula and cause reversible blindness.1 Lymphedema; although rare and not usually related to other diseases, it may be associated with IL.9 Lymphedema is typically less pitting than edema due to hypoproteinemia limited to the lower limbs (foot, ankle, calf, rarely thigh) and mostly bilateral.9 The edema in both patients of this report was more prominent in the right side.
Suresh et al5 reported 4 pediatric cases from India with IL who presented with anasarca, recurrent diarrhea, and hypoproteinemia. More variable presentations have been reported in adult age group including abdominal pain, vomiting, recurrent peripheral edema, diarrhea, or as post traumatic incidental findings.2,5 Lai et al1 reported a 17-year-old female who presented with diarrhea, edema, and diagnosed with PIL after endoscopy. She improved with TPN and MCT. Intestinal obstruction is a rare presentation of IL.2 Rashmi et al2 reported 2 cases of IL; a 35-year-old female and a 21-year-old male. In the first patient, the presentation was mainly with abdominal pain and vomiting, so intestinal obstruction was suspected, and the diagnosis was made after she has a segment of her bowel resected. The second patient presented with a picture of appendicitis and treated with an appendectomy.
Pleural and pericardial effusions can occasionally develop in patients with PIL.6 Like the second patient in this report, IL might present with respiratory symptoms, such as cough or respiratory distress.10 This can be explained by the development of associated pulmonary lymphangiectasia as a part of generalized lymphangiectasia.10
Radiological imaging, such as US or CT scan can indirectly suggest IL by revealing a halo or target sign indicating thickened intestinal walls and ascetic fluids.8,9 Small bowel barium study shows nodular mucosa and mild to moderate loops dilatation in more than 75% of IL patients.8 Similar to our patients, Hashemi et al8 reported the use of various radiological studies in diagnosing IL, including sonography, CT scan, barium studies, and laparoscopy in a 42-year-old male who presented with weakness, abdominal discomfort, and swelling of the legs. Low serum Ig is also an indirect biological abnormality that suggest IL.9 High fecal a1-anti-trypsin clearance can confirm protein loss in IL patients.9 The diagnosis of PIL is confirmed by endoscopic and histological findings.5,9 Endoscopic examination usually reveal a multiple whitish mucosal spots, or a creamy yellow jejunal villi corresponding to markedly dilated lymphatics.9 The definitive diagnosis of PIL is difficult to be settled using only serological tests, endoscopy, colonoscopy, and normal image check, but it can be proven by double balloon enteroscopy, multi-dot biopsy, and particularly by the pathological examination of small intestinal tissue showing dilated mucosal and submucosal lymphatic chanels.1,5 Histopathology is the hallmark of the diagnosis of IL and it is identical in both primary and secondary forms.2 The dilated intestinal lymphatics might be seen in many villi or only few.6,9
Most of the therapeutic approaches in treating IL focus on dietary modifications. Lifelong dietary modification with low-fat, MCT oil, vitamin supplements, and high protein remains the cornerstone in the PIL management.5,6 Enteral nutrition and TPN may be a useful treatment in IL patients.1,5,8 Lai et al1 reported one case of PIL who responded to TPN and MCTs therapy. Once serum protein level normalized, enteral nutrition seems to be useful to prevent relapses but non-compliance leads to relapse of symptoms.1 Upon relaxation of dietary regimen, frequent relapses of clinical symptoms can occur.4 Based on these findings they recommend lifelong continuation of the regimen.1,4,6 Desai et al3 studied the effects of dietary modifications on 55 cases with IL and compared patients receiving MCT therapy (28 patients) with those who did not, and found that 63% of patients who received MCT showed improvement. Tang et al4 reported 4 inpatients with IL from China. The TPN was used as an initial in hospital management. After discharge, intermittent TPN was maintained with gradually tapering, accompanied by long-term dietary control and regular monitoring. They found that great improvement was seen both clinically and in laboratory parameters. However, there are problems related to use of MCT oil as it has a strong odor, expensive, extremely flammable, and has a tendency to smoke.3 In addition, it is clear that not all patients respond equally well to a low-fat, MCT-supplemented diet.3 If the patient did not respond to low-fat and MCT diet, medical therapy, such as antiplasmin therapy and octreotide, a somatostatin analog, should be considered.1,6 Octreotide is the treatment of choice in patients in which dietary modifications failed.6 Long-term therapy of PIL patients with octreotide showed improvement in histological and endoscopic findings.6 However, its effect on IL still remains to be clarified,4 in addition to being an expensive therapy and necessities parenteral administration.6 Patients with PIL are prone to fat-soluble vitamin deficiencies and oral fat-soluble vitamin supplementations are important in the management.6 Surgery is a fairly useful for segmental lesions of IL and local bowel resection has been reported as a successful treatment.4 Treatment of underlying condition is useful in cases with secondary type of IL.2
Intestinal lymphangiectasia is considered a form of a secondary immune deficiency and gamma globulin infusions should be considered in case of recurrent infections.6 Similar to the second patient, patients with IL can develop widespread cutaneous viral warts, which might be related to immune deficiency or lymphoma.9 It is still not clear whether IL can lead to occurrence of malignancy, especially lymphoma.9 If lymphoma or pleural or cardiac effusion occurred, the outcome of PIL patient may be severe, or even life threatening.9
In conclusion, after excluding secondary causes like rheumatic, neoplastic, and parasitic infections, the diagnosis was confirmed with endoscopic and histological examinations in these 2 patients with PIL. Both patients showed a positive clinical response to dietary modification with low-fat and MCTs. However, further reports are needed to clarify the effect of different therapeutic options on the long-term outcome of IL patients.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Acknowledgment
The authors gratefully acknowledge Dr. Ashok K. Malik and Dr. Eman Al-Jufairi, Pathology Consultants, for reviewing the histopathology figures; and Dr. Husain Naser and Dr. Hakeema Al-Hashemi, Radiology Consultants, for reviewing the radiology figures, and all the medical staff and technicians registered at Salmaniya Medial Complex, Manama, Bahrain.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received August 25, 2015.
- Accepted October 13, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.