


Abstract
Objectives: To provide more data regarding the role of an amperometric glucometer in diagnosing meningitis.
Methods: This is a prospective study conducted at the Pediatric and Neonatology Department, Qatif Central Hospital, Qatif, Saudi Arabia between March 2017 and September 2018. We measured glucose concentrations in cerebrospinal fluid (CSF) and blood using a central laboratory and amperometric glucometer (AG). We compared CSF/blood glucose ratios obtained in a central laboratory from clinical bedside examination with a glucometer, and calculated the sensitivity and specificity for detecting cases of meningitis.
Results: A total of 101 patients with clinical suspicion of meningitis were recruited for CSF sampling. Of 101 CSF samples, 61 (60%) were suggestive of meningitis. Of 101 samples, 47 had hypoglycorrhachia identified by a standard laboratory, and 17% of them were also detected by AG. The correlation between CSF/blood glucose by AG and laboratory ratios was substantial (r=0.894, p<0.01, 95% CI: 0.805-0.983). The AG sensitivity was 100% and specificity was 55% in pediatric cases, while in neonates the sensitivity was 86% and the specificity was 26%.
Conclusion: Amperometric glucometers can be used to detect hypoglycorrhachia accurately. This point-of-care testing tool is easily accessible and can be used by health care providers for cases suspected of meningitis.
Hypoglycorrhachia (abnormally low cerebrospinal fluid (CSF) glucose) is associated with a variety of diseases that can affect both neonates and pediatric age groups, such as meningitis, glucose transporter 1 deficiency, central nervous system leukemia, and others.1,2 One of the most common diseases that causes hypoglycorrhachia is bacterial meningitis, which has high mortality and morbidity rates and accounts for more than 1.2 million cases estimated to occur worldwide each year.3 The International Journal of Infectious Diseases published an article in 2012 stating that there were 274 reported cases of meningococcal meningitis in Saudi Arabia in 2001.4
Early diagnosis and initiation of meningitis management are of utmost importance inform of decreasing mortality and improving outcomes significantly.5 In 2016, Bodilsen et al6 observed that the delay in the management of bacterial meningitis more than 6 hours from admission was associated with undesirable outcomes compared to those who received the treatment within 2 hours. Immediate bedside diagnosis of meningitis and initiation of treatment, like cytological analysis is crucial, though not feasible in many situations. Other measures could improve the decision of starting antibiotics earlier and improve outcomes. Evidence for such methods, including point-of-care (POC) strip reagent testing for cerebrospinal fluid (CSF) glucose, protein, and leucocytes, are lacking, though it could facilitate decision-making if demonstrated to be accurate. Several studies have analyzed other methods, which have been suggested using a POC glucometer to determine glucose level in CSF.7,8 In 2015, Nirupam et al7 evaluated the accuracy between an amperometric glucometer (AG) and an autoanalyzer (AA) with 50 neonates and concluded that AG is a potential tool for bedside measurement of CSF glucose. Another study with pediatric subject up to the age of 12 years found that glucometer strips have 87% sensitivity and 96% specificity.8 However, both studies had a limited sample size.
In this study, we aim to provide more data regarding the role of AG in facilitating the detection of suspected meningitis in clinical practice.
Methods
This study was conducted in the Pediatric and Neonatology Department, Qatif Central Hospital (QCH), Qatif, Saudi Arabia. The prospective study period lasted for 15 months between March 2017 and September 2018. Ethical approval was obtained by an institutional review board from QCH.
Pediatric patients from 0 to 14 years who were admitted to QCH with a clinical suspicion of meningitis were included in the study. Preterm neonates, patients with missing data or delay in sample analysis were excluded from the study. A total of 101 CSF samples were obtained from neonates and pediatric patients. All CSF sampling was performed by pediatric residents using a lumbar puncture. Cerebrospinal fluid glucose was tested by AG. Cerebrospinal fluid samples were sent immediately for processing in the laboratory for cytology (white blood cell and red blood cell count), cultures, gram staining, latex agglutination testing, and biochemical analysis. Biochemical analysis was carried out with the Siemens Dimension Glucose analysis device (Siemens Healthcare GmbH., Erlangen, Germany). Sampling and laboratory analysis were carried out within a window of 30-60 minutes. We excluded patients with delayed CSF laboratory analysis of more than one hour from the study.
Bedside measurement was performed by pediatric residents immediately after collection. The glucometer used in this study was the FreeStyle Optium Neo Rev. A 05/14 (Abbott’s Diabetes Care, Berkshire, UK) with an amperometric system that measures the electric current generated at a specific point in time by the glucose reaction. Serum blood glucose was measured within one hour before CSF sampling.
Patients were classified into the normal CSF group or high clinical suspicion of meningitis group according to CSF analysis. The cases identified were thought to have high suspicion of meningitis by having positive CSF culture, hypoglycorrhachia defined as a CSF-to-serum glucose ratio of <0.6,9 CSF protein more than 100 mg/dL,10 or CSF white blood cell count more than 6 cells/uL for children older than 3 months of age, more than 9 cells/uL for infants 29 to 90 days, and more than 20 cells/uL for neonates.10-12
Statistical analysis
We used IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, N.Y., USA) program for statistical analysis. A t-tailed test with a p-value of <0.05 was used to determine significance. Shapiro-Wilk normality testing was applied for describing the distribution of the data. The concordance correlation coefficient was analyzed, with a score of one indicating perfect agreement.
The primary outcome of the study was to verify AG measurements in comparison with standard laboratory biochemical analysis in children with high suspicion of meningitis. The secondary outcome was evaluating the accuracy of glucose values obtained by AG compared with standardized methods used at Qatif Central Hospital.
Results
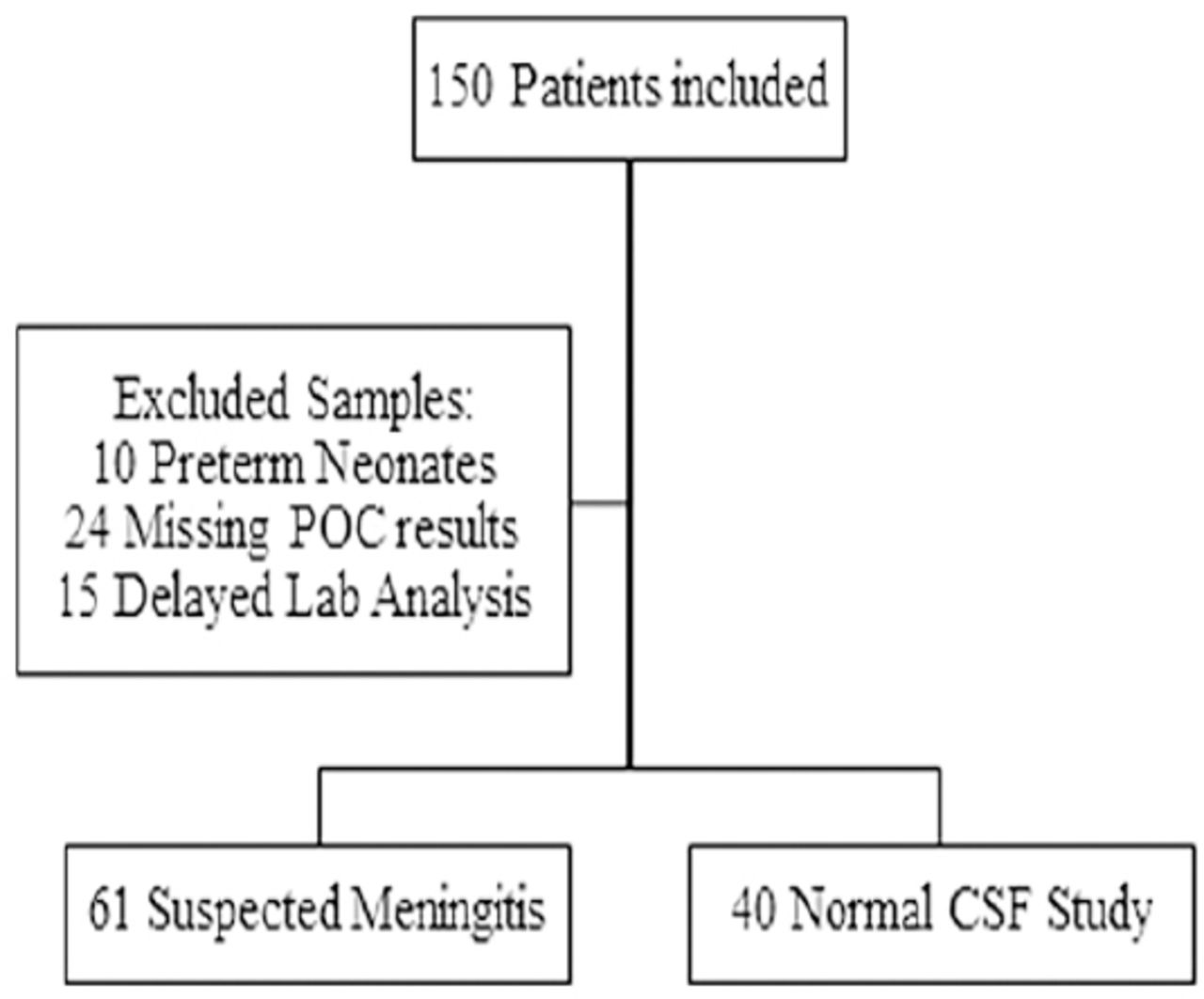
A total of 150 patients had CSF sampling during the study’s duration at QCH. In terms of exclusion, 49 samples were excluded from the study as demonstrated in Figure 1. We analyzed 101 patients with clinical suspicion of meningitis in total (54% pediatric and 46% neonates). From each, a CSF sample was taken for CSF glucose measurement. From the 101 patients evaluated, 61 CSF samples (26 pediatric and 35 neonates) indicated high suspicion of meningitis by laboratory analysis. Proportionally, 17% of CSF samples with high suspicion of meningitis had abnormal white blood cell counts while 21 samples had significantly high protein count. The CSF characteristics are summarized in Table 1.

Flow diagram showing flow of participants. POC: point-of-care, CSF: cerebrospinal fluid
Initial cerebrospinal fluid analysis.
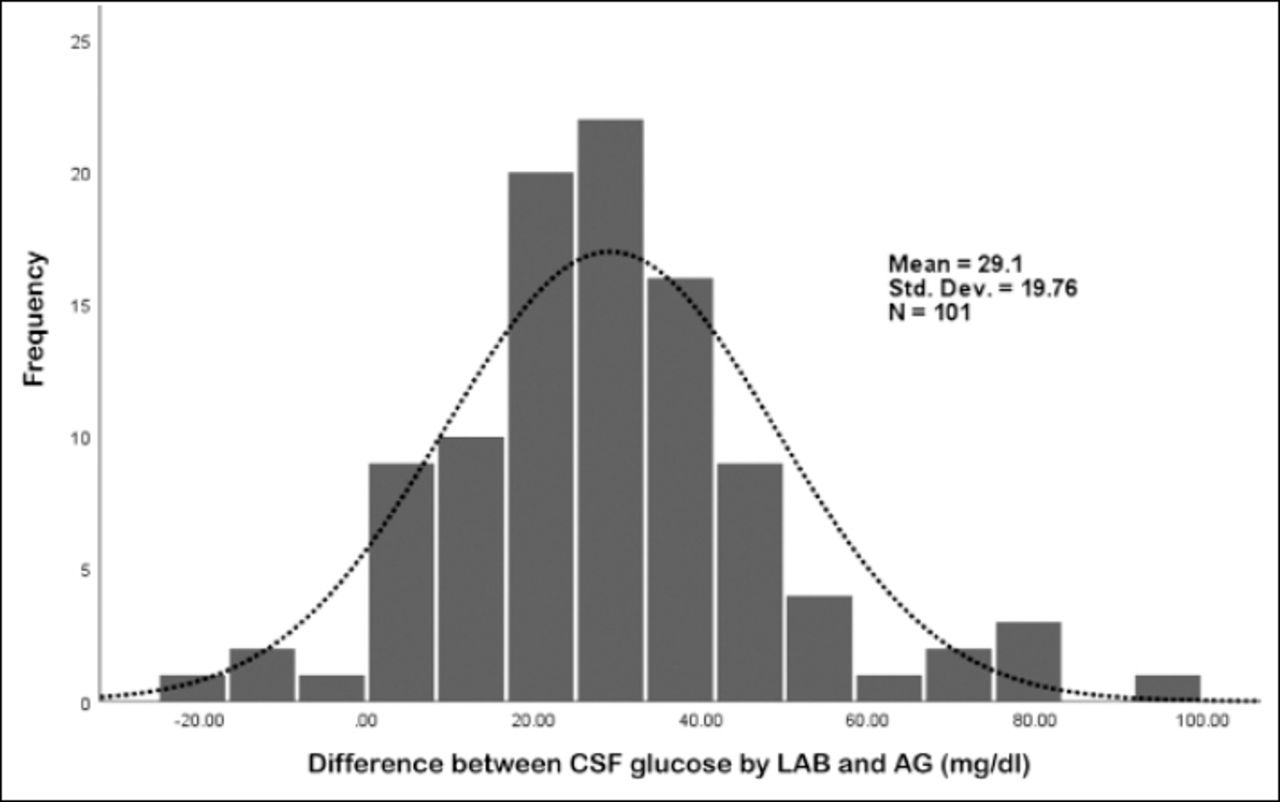
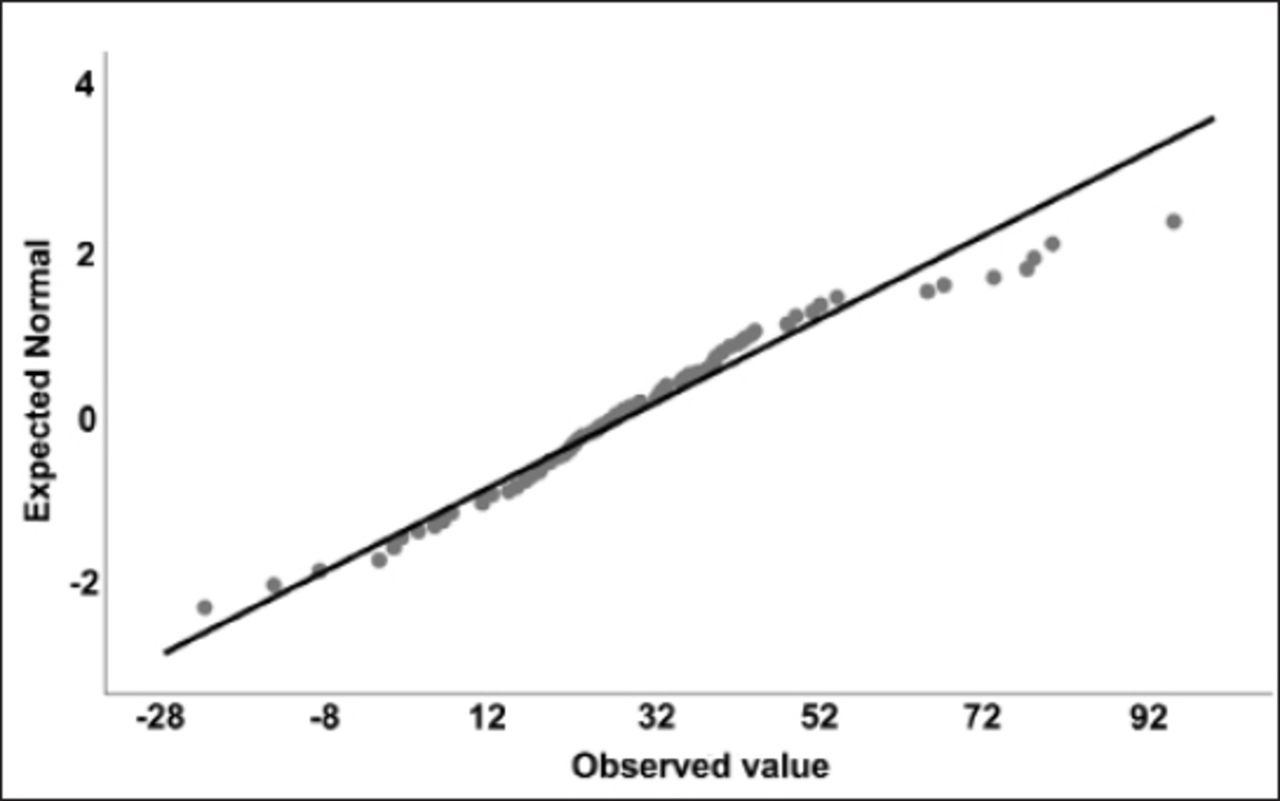
A total of 47 samples had hypoglycorrhachia identified by the standard laboratory. Proportionally, 17% of them were also detected by the AG. Most of the remaining 54 cases that were reported to have normal glucose levels by the laboratory were also found to be normal by AG (98%). The difference in measurements between CSF laboratory glucose and AG values were normally distributed (Figures 2 & 3) with Shapiro-Wilk normality testing significance of 0.13.

Histograms for the difference between CSF glucose measurements by LAB and AG. CSF: cerebrospinal fluid, LAB: standard laboratory, AG: amperometric glucometer

Q-Q Plot for the difference between CSF glucose measurements by LAB and AG
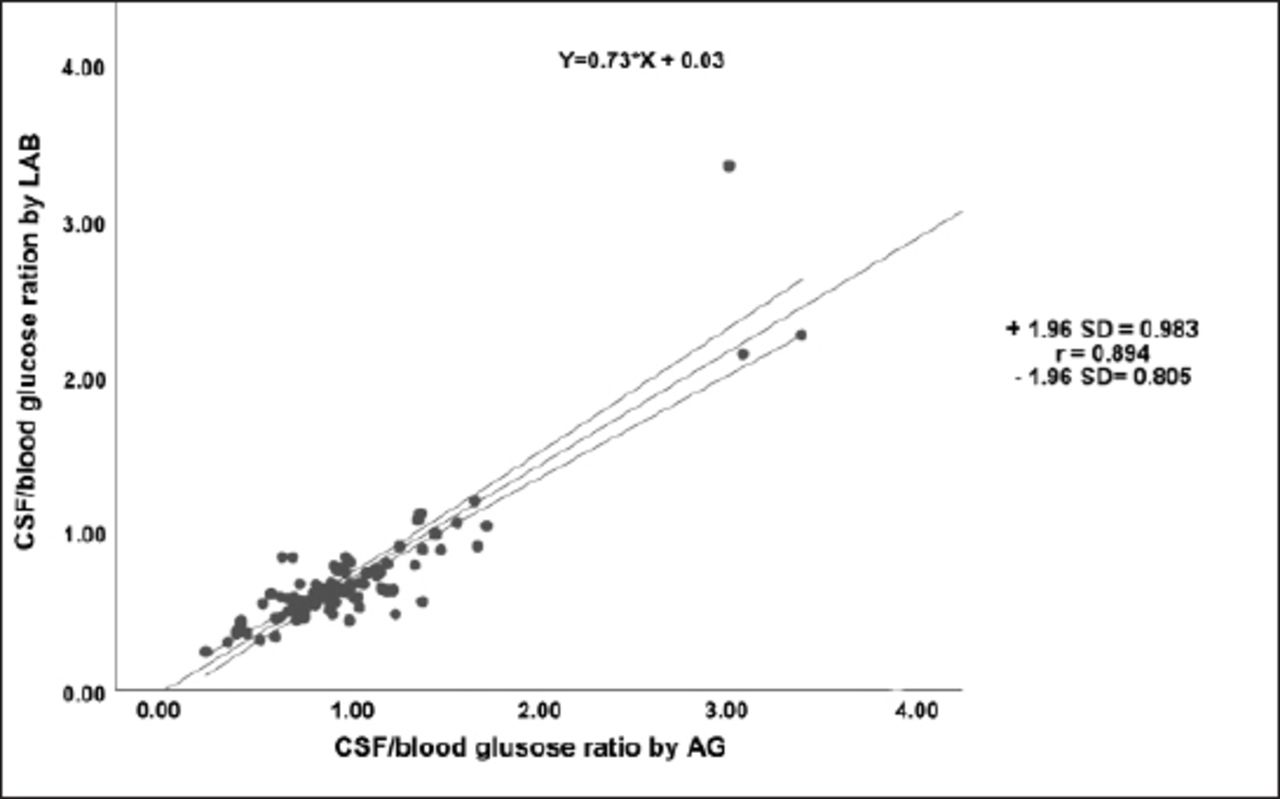
The correlation between the CSF/blood glucose by AG and LAB ratios was substantial (r=0.894, p<0.01, 95% CI: 0.805 - 0.983) (Figure 4). The paired-mean difference for glucose measurements between the 2 methods was 29.11±19.76 mg/dl (1.6±1.1 mmol/L) (p<0.000) for all CSF samples while in cases of hypoglycorrhachia, the paired-mean difference was not significant (4.2±4.9 mg/dl [0.2±0.3 mmol/L], p=0.18).

Correlation curve of the CSF/blood glucose ratio obtained by amperometric glucometer and the laboratory
When the POC glucometer was used to enhance confirming suspicion of meningitis, the sensitivity of the AG was 100% and specificity was 55% in pediatrics, while the sensitivity of neonates was 86% and specificity was 26%. Both groups combined showed that AG is 89% sensitive and only 42.3% specific.
Discussion
Measuring CSF glucose is an important diagnostic tool for a variety of diseases. In cases of meningitis, hypoglycorrhachia is a significant finding. Early detection of hypoglycorrhachia in patients suspected to have meningitis can aid in the early initiation of antibiotics and thus improve mortality and morbidity.
There have been many studies published regarding different POC methods to detect hypoglycorrhachia.7,8,13-16 Point-of-care tools and methods have pre-analytical and analytical errors while diagnosis also depends on the health care provider’s knowledge surrounding how to use them. In 2018, Mazumder et al13 employed a urine reagent strip test as a quantitative method for CSF analysis of 100 samples and indicated that it is highly specific (100%), but less sensitive for glucose. This study also quantified leukocytes and protein, endowing the urine strep method with more value in POC CSF analysis. This study and many others indicated that urine reagent strips can be used in detecting pleocytosis and low glucose in CSF at facilities that do not have the appropriate laboratory settings for CSF analysis, though it does not yield numeric readings and cannot be applied to differentiate between bacterial or viral meningitis.15,16 Another group used the iSTAT CHEM8 and CG4+ cartridges for analysis with correlating results compared to traditional methods for measuring CSF glucose,14 which is also a helpful method for fast detection of hypoglycorrhachia but not as accessible as other POC tools.
Few studies have investigated the ability of POC glucometers to measure CSF glucose, especially in the pediatric age group.7,8 Different models of glucometers with various technologies are widely available at lower prices compared to other tools. In 2015, Nirupam et al7 assessed the CSF glucose in 50 neonates, of which 13 had meningitis. They demonstrated the difference between a photometric glucometer and an AG, concluding that a photometric glucometer is poorly correlating with standard laboratory methods compared with an AG, which was significantly correlated with 100% sensitivity in detecting CSF hypoglycorrhachia in cases with meningitis.7
Rousseau et al17 analyzed 172 CSF samples utilizing a POC AG and standard laboratory methods. The median age of the study population was 55 years (range: 28-77 years). They concluded that a bedside glucometer has a sensitivity of 94.1% (95% CI: 71.3-99.9%) and specificity of 91% (95% CI: 85.3-95%).17
This study included a larger sample size (101 CSF samples of the neonatal and pediatric age groups) compared to other studies of the same age group.7,8 Using AG for CSF glucose measurement, the study found that the readings were correlated significantly with laboratory results. The paired-mean difference for AG CSF glucose measurements was 29.11±19.76 mg/dl (1.6±1.1 mmol/L) compared with laboratory methods across all CSF samples, whereas the paired-mean difference was 4.2±4.9 mg/dl (0.2±0.3 mmol/L) when compared for cases with hypoglycorrhachia. This narrow range difference is acceptable for clinical use and supports the findings described by Nirupam et al in 2015.7
Overall, this study showed that AG is highly sensitive in detecting hypoglycorrhachia, but has low specificity (sensitivity: 89%; specificity: 42.3%) compared to what was reported by Rousseau et al17 when they performed a similar study on an older age group (sensitivity: 94.1%; specificity: 91%).
Study limitations
Few cases were discovered to have hypoglycorrhachia, which can affect the sensitivity and specificity of AG, as well as the time difference between sampling, which can be minimized further in facilities where the laboratory method can be applied at the same time as AG to CSF samples. Studies with larger sample size can overcome these limitations.
In conclusion, AG can be a potential tool for measuring CSF glucose for the rapid detection of hypoglycorrhachia with just slight overestimation in glucose readings. This overestimation can be explained by the time difference between measurements by the 2 methods as described by Rajesh et al18 in 2010 when they established that delays in CSF analysis can decrease glucose value.
Acknowledgment
We would like to thank Cambridge Proofreading LLC (www.proofreading.org) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 5, 2020.
- Accepted May 13, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}
{kind=link}
{kind=link}
{kind=link}