


Abstract
A duodenal hematoma secondary to blunt -abdominal trauma is a relatively rare condition and is usually managed conservatively. We report a case of a post-traumatic duodenal hematoma after a road traffic accident in a 10-year-old boy, who presented with progressive vomiting 3 weeks after the accident. The case was managed using serial esophagogastroduodenoscopy (EGD) with dilatation. Controlled radial expansion (CRE) balloon dilatation was performed 4 times over a period of 11 weeks. The patient recovered uneventfully and remained asymptomatic at the 3-month follow-up after the last endoscopic dilatation. This case highlights the applicability of EGD with CRE balloon dilatation as an alternative to surgical treatment in patients with symptomatic post-traumatic duodenal hematomas.
Intramural duodenal hematomas (DHs) are relatively rare in the pediatric population, observed in only 3-5% of cases of abdominal injury in children.1-3 Commonly, the duodenum is compressed between the colliding object and the vertebral column during the injury.3 The most widely recognized causes of trauma leading to DH in the pediatric population include road traffic accidents (RTAs) and abuse.3 Intramural duodenal hematomas usually present within a few days of the trauma, with conservative management being the first choice of treatment. In general, surgical management is reserved for patients with perforation, other injuries requiring surgical intervention, or with persistent symptoms such as feeding intolerance or vomiting that do not resolve within 3 weeks.4,5 We present a case of DH in a child, aiming to describe a novel treatment using endoscopic balloon dilatation. This treatment strategy is less invasive and may serve as an alternative to surgery.
Case Report
A healthy 10-year-old boy presented with a right forearm fracture after an RTA; he exhibited no signs of abdominal pain or vomiting. An abdominal computed tomography (CT) scan was performed at the time of admission. Although he had developed a DH, this was missed during CT screening (Figure 1).

First computed tomography scan of abdomen: showing dilated wall of duodenum.
Clinical findings
Laboratory evaluations indicated a hemoglobin level of 12.2 g/dl, an alanine transaminase (ALT) level of 259 U/L, and an aspartate aminotransferase (AST) level of 412 U/L; this was thought to be related to the RTA. Other laboratory evaluations indicated that the renal profile, amylase level, and coagulation profile were within the normal range. Hemoglobin level remained stable, while ALT and AST levels decreased during admission. He exhibited no further symptoms and was discharged after 2 days with a cast on the right forearm; no other interventions were considered necessary.
Diagnostic assessment
Three days after discharge, the patient started to vomit. The frequency of vomiting increased with time and persisted for 27 days before medical advice was sought. The patient presented to our emergency department with persistent nonbilious vomiting, abdominal pain, inability to tolerate feeding, and weight loss of 2 kg. He was considered to have an intestinal obstruction. A CT scan was performed, this time revealing a DH causing narrowing of the duodenal lumen (Figure 2). His hemoglobin level was maintained, and his ALT and AST levels, amylase levels, and coagulation profile were within the normal range. He was kept nil per os (NPO) for 5 days; however, his clinical symptoms did not improve.

Second computed tomography scan of abdomen showing dilated stomach and first and second part duodenum and stenosis in third part of duodenum (arrows).
Therapeutic intervention
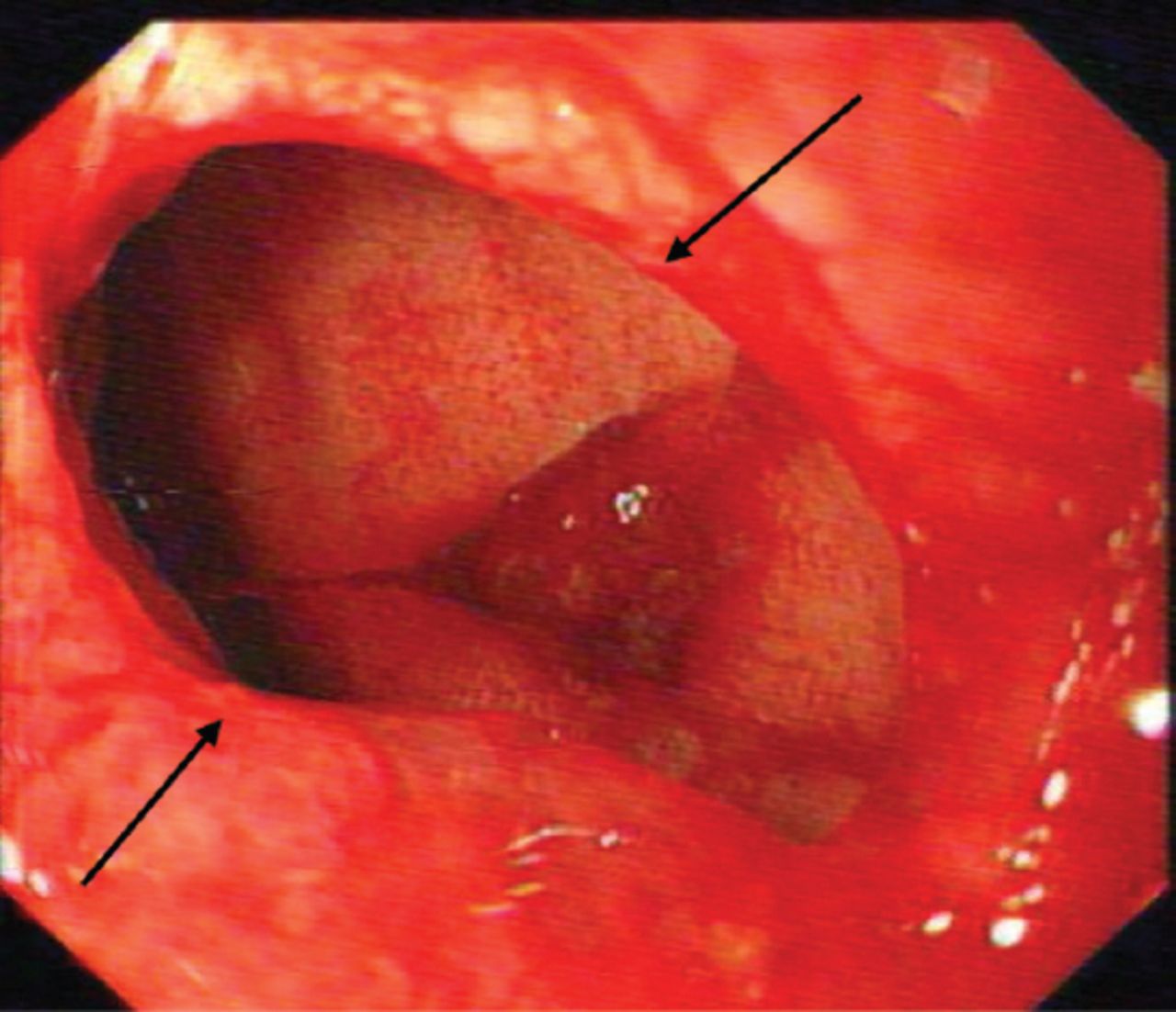
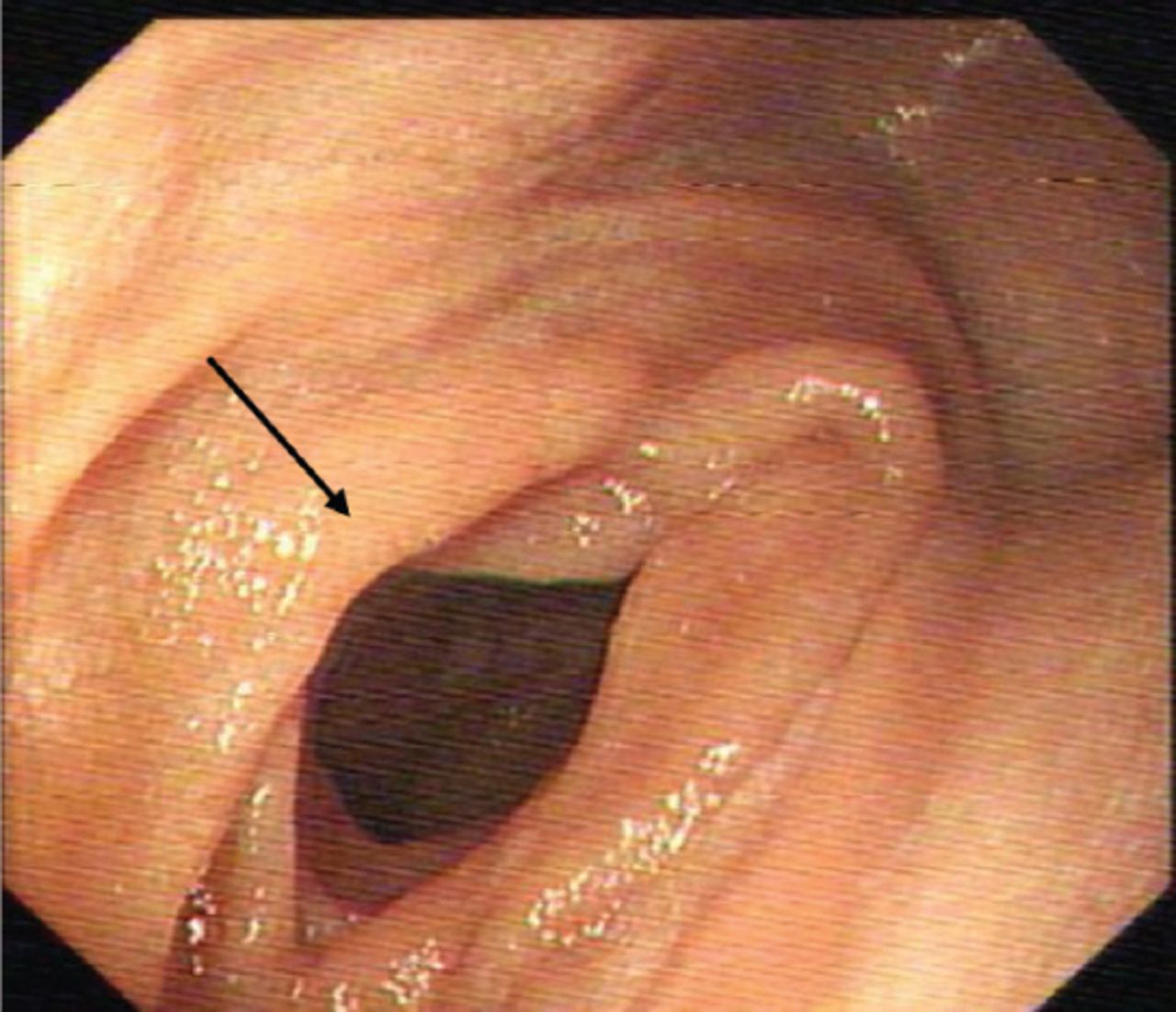
Pediatric esophagogastroduodenoscopy (EGD) was performed, revealing severe stenosis in the third portion of the duodenum; the pediatric gastroscope with an outer diameter of 8.9 mm could not pass through. A controlled radial expansion (CRE) balloon was dilated to 15 mm without complications (Figures 3-5). Omeprazole was initiated at a daily dose of 1 mg/kg. The patient tolerated full oral intake and was discharged 2 days after the dilatation procedure with a follow-up EGD appointment in 2 weeks. During the EGD follow-up, a recurrence of the severe stenosis in the same area was detected, and CRE balloon dilatation to 18 mm was performed without complications. He underwent 2 more sessions of endoscopic CRE dilatation, and a better outcome for the outer diameter of the third portion of the duodenum was achieved at the end of the fourth session.
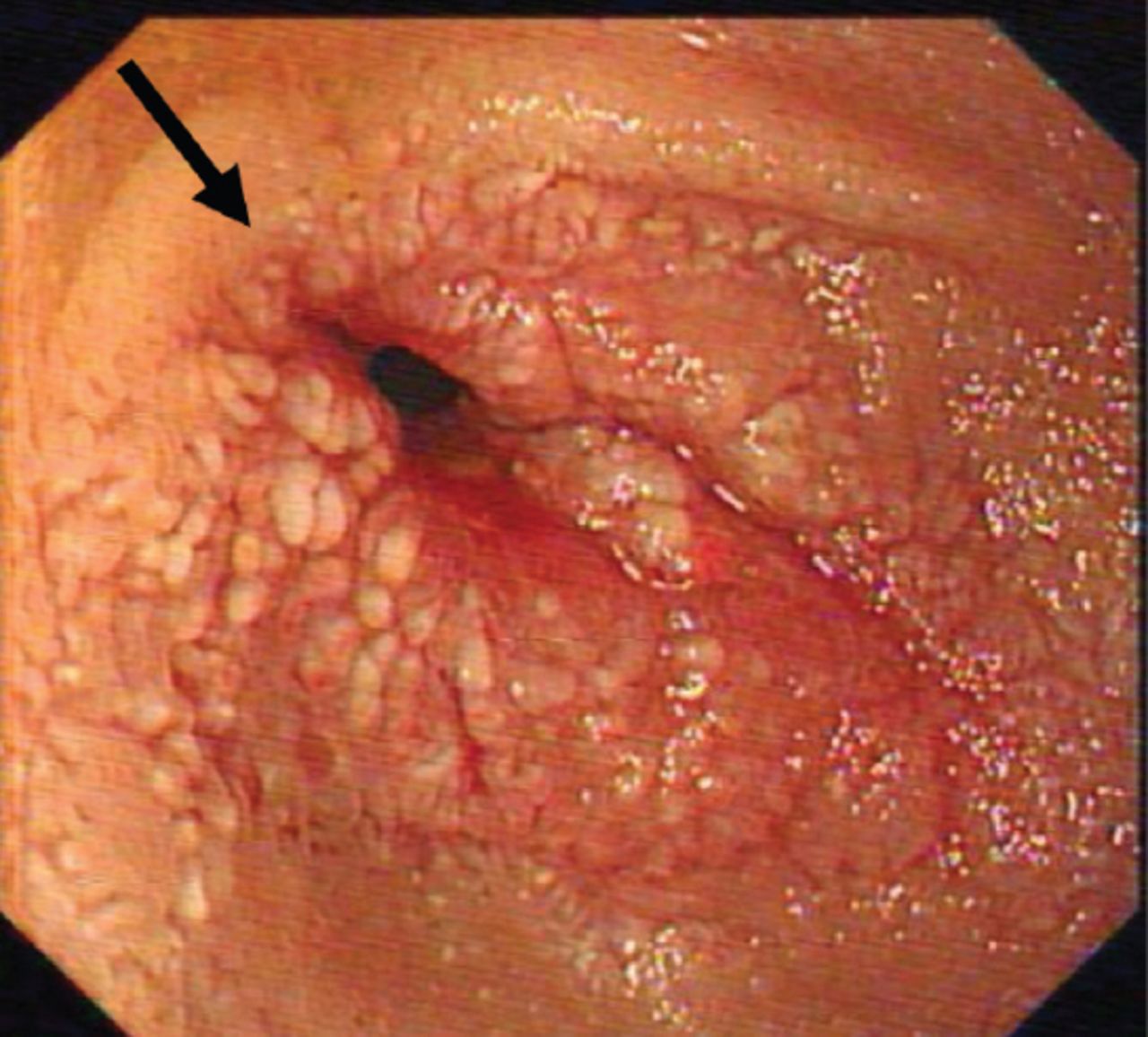
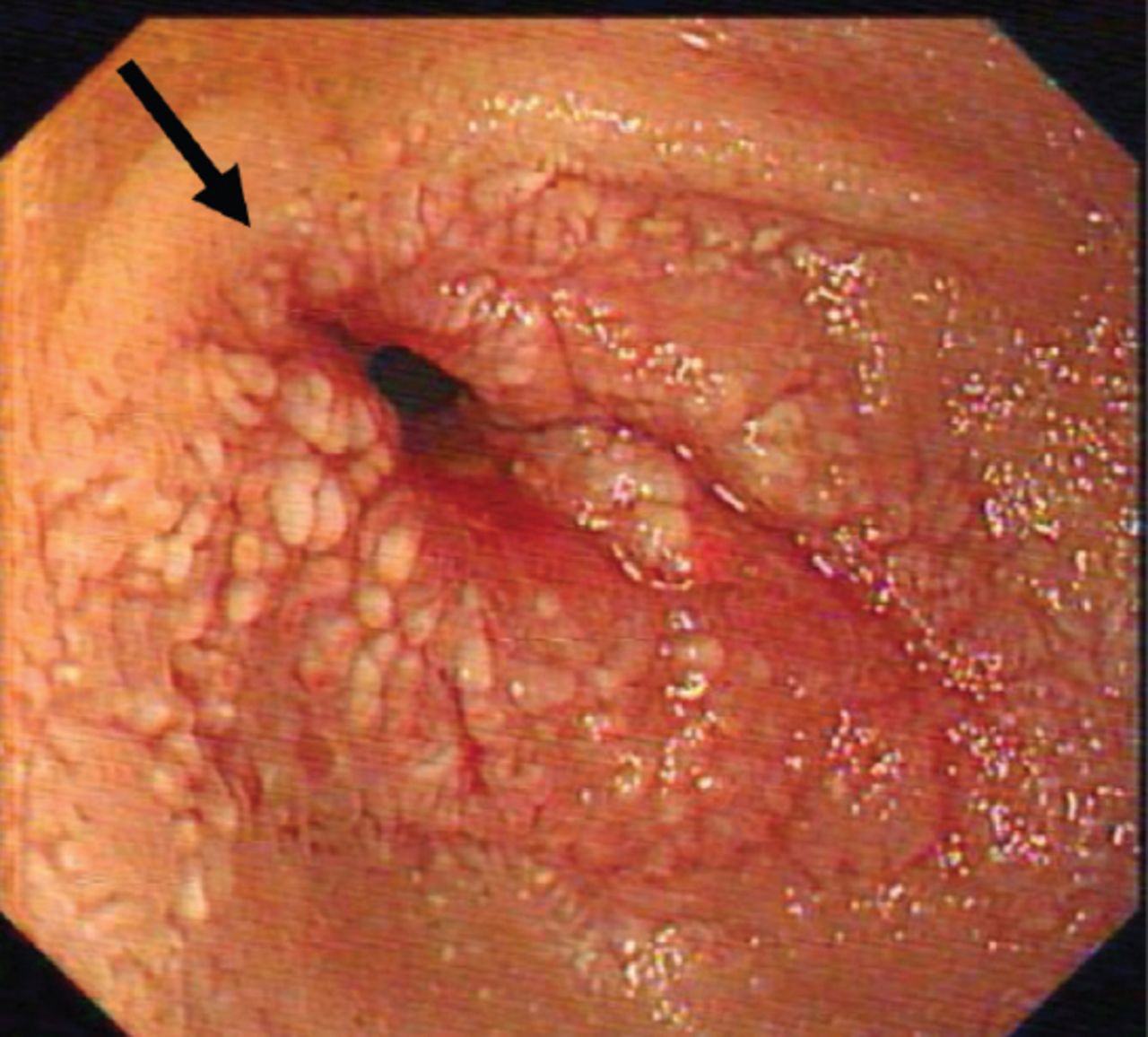
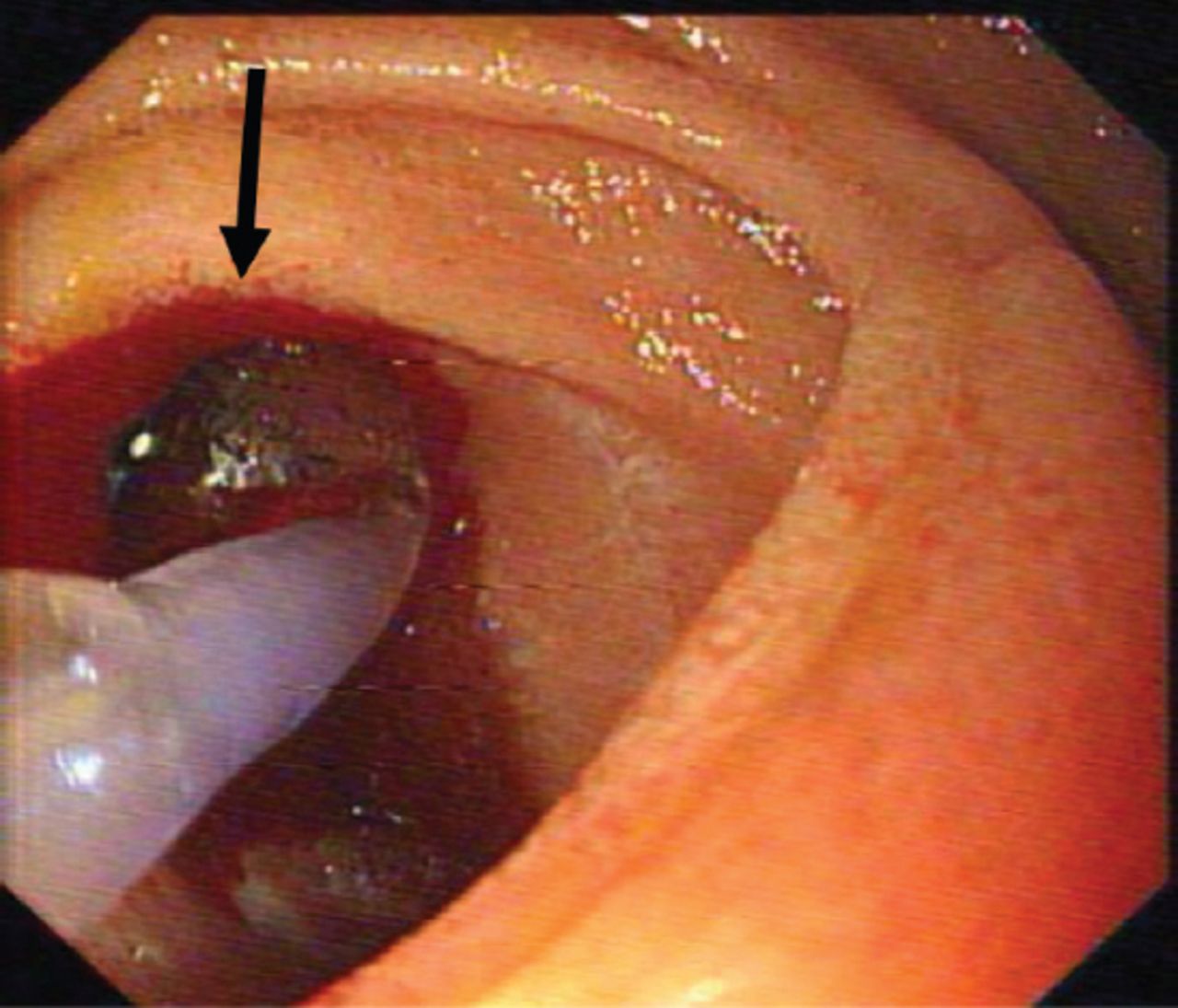
First esophagogastroduodenoscopy pre-dilatation image showing the stenosis of the duodenal lumen (arrow).

First esophagogastroduodenoscopy showing controlled radial expansion balloon dilatation of the stricture of the duodenal lumen (arrow).
First esophagogastroduodenoscopy post-balloon dilatation image showing improvement of the stricture of the duodenal lumen (arrows).
Follow-up and outcomes
At the fifth EGD (performed 11 weeks after the first EGD), no stenosis was detected and no interventions were required (Figure 6). He remained asymptomatic throughout the 3-month follow-up period in our outpatient clinic and experienced improved weight gain.
Last esophagogastroduodenoscopy showing a complete resolution of the stricture and normal duodenal lumen (arrow).
Discussion
We were successfully able to manage the DH via EGD with endoscopic balloon dilatation. While a patient’s history and physical assessment may aid in detecting the cause of the duodenal obstruction, a radiological study is needed to confirm the diagnosis.6 Ultrasound may be used, which will show a thickened wall or an obstruction of the lumen. An upper gastrointestinal series may also aid in identifying the obstructed area; however, a diagnosis cannot be achieved using this method.6,7 Computed tomography scan remains the gold standard for establishing the diagnosis of DH as heterogeneous attenuation of the duodenal wall may be observed and will aid in ruling out perforation.6 Recurrent abdominal pain, vomiting, and feeding intolerance are noted in children who exhibit late presentation, as seen in our case.4 Intramural duodenal hematomas are usually treated conservatively by keeping the patient NPO, starting total parenteral nutrition (TPN), and performing nasogastric tube decompression; in most cases, the patient resumes a normal diet after an average of 2-3 weeks.4,5 However, surgical treatment is required in cases of bowel perforation or where symptoms persist after 2 to 3 weeks.2,3
Another management modality that may be used after the failure of conservative management is CRE balloon dilatation, although this procedure is not widely used, as noted upon review of the available literature. Samra et al,8 reported successful treatment of an intramural hematoma in an adult patient via the simple passage of the gastroscope; this passage aided in opening of the duodenal stricture, suggesting the possibility of endoscopic balloon dilation as another treatment method.
Our patient was a survivor of an RTA with a delayed presentation (21 days after the RTA) of intestinal obstruction. The obstruction was managed using serial endoscopic balloon dilatation over a period of 11 weeks. The patient was successfully discharged 1-2 days after each procedure, that is, with a decreased hospitalization duration, and the patient showed good oral intake. During the 3-month follow-up period after the last endoscopic dilatation, the patient remained asymptomatic with rapid weight gain. Controlled radial expansion balloon dilatation was performed successfully with no immediate or late complications. This novel modality may, therefore, be used to treat cases of DH instead of surgical management.
Study limitations
First, this specific approach to treatment has not been previously described and is thus not standardized. Second, further research is required to confirm the efficacy of this technique.
In conclusion, EGD with dilatation of a CRE balloon for management of a DH is feasible, safe, and effective and could help avoid surgical intervention. We believe that this approach could herald a change in the practice of DH management.
Acknowledgment
The authors gratefully acknowledge Dr. Bashar A. Ahmad, consultant pediatric radiologist, in Prince Sultan Military Medical City, for reviewing the CT scan images and we would like to thank (www.editage.com) for editing service.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 5, 2020.
- Accepted April 29, 2020.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.