


Abstract
Objectives To compare dynamic thiol/disulfide homeostasis between patients with community-acquired pneumonia (CAP) and healthy controls.
Methods This prospective, case-control study was conducted in the Department of Pulmonary Diseases, Ankara Ataturk Training and Research Hospital, Yildirim Beyazit University, Ankara, Turkey, between August 2016 and August 2017. In total, 50 hospitalized patients with CAP and 35 healthy individuals were enrolled. Patients with comorbidities and smokers were excluded. The thiol/disulfide state was evaluated in each group. Thiol levels (native/total) and % polymorhonuclear leukocytes and C-reactive protein levels association were evaluated in patients with CAP.
Results There was no significant difference between the CAP and control groups in age or gender (both, p>0.05). The disulfide (SS) levels were similar between the 2 groups (p=0.148). The total thiol (TT) and native thiol (SH) levels were significantly lower (all, p=0.001) and the SS/TT levels were significantly higher (p=0.019) in the CAP group compared with the controls.
Conclusions This study showed that the oxidant/antioxidant ratio was shifted to the oxidative side in CAP patients. An abnormal thiol/disulfide state may be an important factor in the pathogenesis and monitoring the treatment response. The thiol resources may use for treatment in CAP and may positively affect the prognosis.
Pneumonia is a common cause of morbidity and mortality in adults worldwide.1 Among all infectious diseases, community-acquired pneumonia (CAP) is a leading cause of death in both the developed and developing worlds.2,3 Over the past 10 years, a 34% increase in hospital admissions has been observed, especially of elderly patients, due to CAP.4 Lungs are susceptible to oxidative damage due to their location and function. Oxidative stress and environmental oxidants resulting from an oxidant/antioxidant imbalance play an important role in respiratory tract diseases and inflammation.5 Plasma thiols have anti- and pro-oxidant properties and contain a sulfhydryl group (-SH).6,7 The plasma thiol pool is comprised of albumin, protein thiols, and low molecular weight thiols (cysteine, cysteinylglycine, glutathione, homocysteine, and γ-glutamylcysteine).7 When thiol compounds undergo oxidation reactions, they form disulfide bonds. Dynamic thiol/disulfide homeostasis plays a critical role in metabolism and homeostasis.6,8,9 Recently, a variety of biomarkers have been examined in the serum of CAP patients.4 Many studies have focused on acute phase proteins.10 However, few studies have shown the importance of oxidative stress in the etiopathogenesis of pneumonia.
The aim of this prospective, case-control study was to compare dynamic thiol/disulfide homeostasis between patients with CAP and healthy controls.
Methods
This prospective, case-control study was conducted in the Department of Pulmonary Diseases, Ankara Ataturk Training and Research Hospital, Yildirim Beyazit University, Ankara, Turkey, between August 2016 and August 2017. The study was approved by the Ethics Committee (approval No. 26379996/188) and informed consent was obtained from all participants. This study was conducted in accordance with the tenets of the Declaration of Helsinki.
In total, 50 hospitalized patients with CAP and 35 healthy individuals were enrolled. Healthy controls were randomly selected from healthy individuals who came to outpatient polyclinic of chest diseases for routine control. Exclusion criteria were patients with comorbidities, including cardiovascular, cerebrovascular, liver and rheumatic diseases, as well as intensive care patients, acute-on-chronic kidney injury, malignancies, diabetes mellitus, immunosuppression were excluded. Patients using antioxidants, lipid-lowering drugs, cigarettes, or vitamin supplements were also ineligible for inclusion, as were those younger than 18 years and pregnant women. The thiol/disulfide state was compared in both study groups. The correlations between the percentage polymorphonuclear leukocytes (%PMNLs) and C-reactive protein (CRP) and thiol (native/total) levels were evaluated in patients with CAP.
Laboratory tests
Blood samples were collected and serum was separated by centrifugation at 1,800 g for 10 minutes and stored at -80°C until analysis. The serum native and total thiol (TT) levels were measured using the method described by Erel and Neselioglu using a Roche cobas-c501 automated analyzer (Roche, Mannheim, Germany). Briefly, the native thiol (SH) levels in each sample ere measured by reacting the thiol groups with 5,5’-dithiobis-(2-nitrobenzoic) acid (DTNB). To measure the TT levels of the samples, the disulfide bonds (SS) were first reduced with sodium borohydride to form free 2 thiol groups. The remaining sodium borohydride was eliminated with formaldehyde to prevent the reduction of DTNB, and the thiol groups, including both reduced and SH groups, were determined spectrophotometrically at 412 nm after the reaction with DTNB. The amount of dynamic disulfides equals half of the difference between the TTs and SHs. After determining the native and TTs and amount of disulfides, the SS/TT, SS/SH, and SH/TT percentage ratios were calculated.6
The CRP levels were measured turbidimetrically with the CardioPhase hsCRP kit (Siemens Healthcare Diagnostics Products, Marburg, Germany) using a BNII Nephelometer Analyzer (Siemens, Munich, Germany).
The PMNLs were counted using a Sysmex XE-2100 automated hematology system (Sysmex, Kobe, Hyōgo, Japan).
Statistical analysis
IBM SPSS Statistics for Windows, Version 20.0. (IBM, Armonk, NY, USA) was used for the statistical analyses. The normality of distribution of the data was evaluated with the Kolmogorov-Smirnov test. Variables were compared using the mean and standard deviation for continuous data. Student’s t-test was used to evaluate differences between group means for continuous variables. The chi-square test (x2) was used to evaluate differences for categorical variables. A p-value ≤0.05 was taken to indicate significance. To assess the associations between %PMNLs and CRP and the thiol/disulfide parameters, correlation analysis was performed.
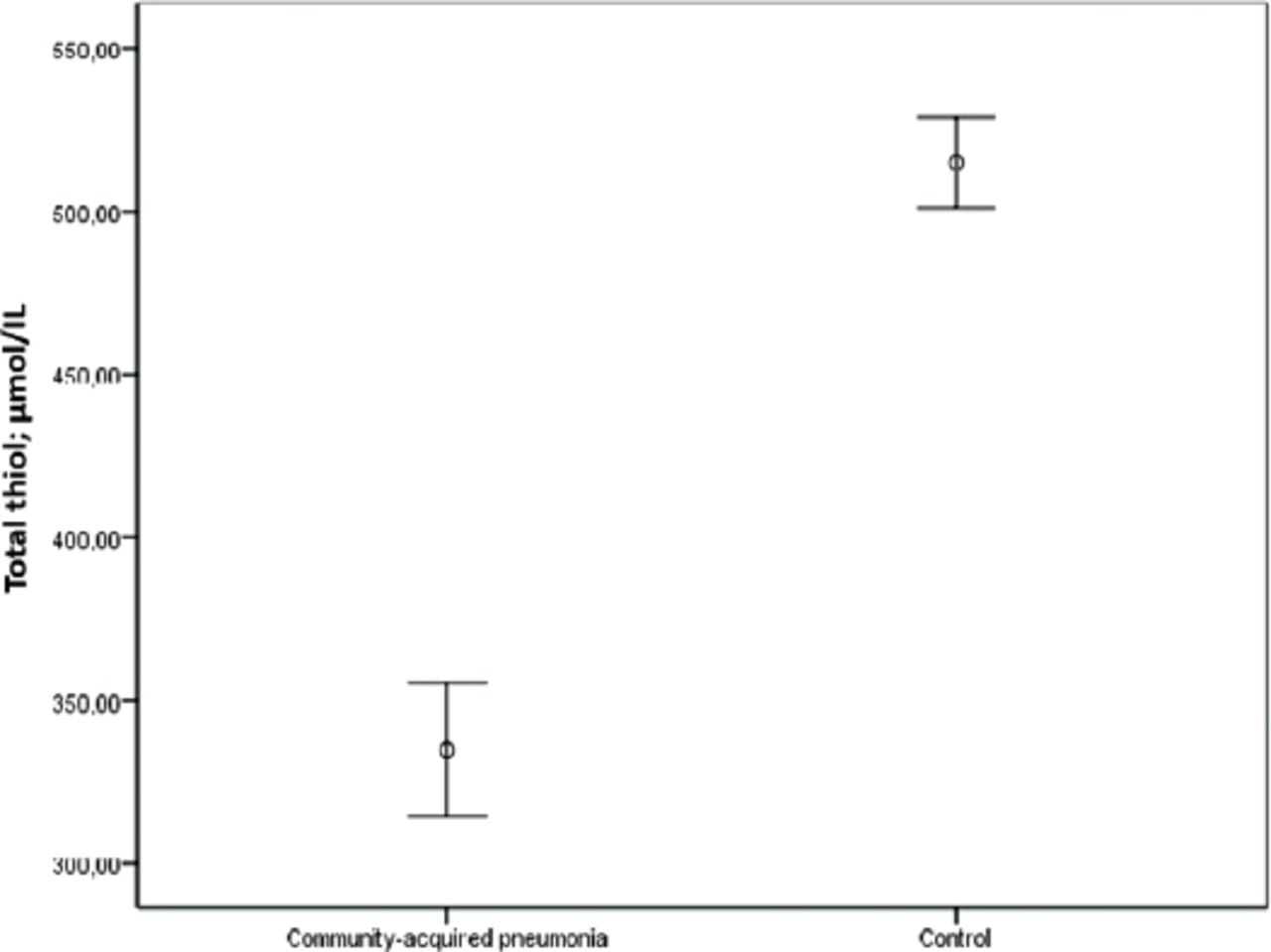
Results. The study population comprised 50 patients with CAP (mean age 52.64 ± 17.78 years) and 35 healthy controls (mean age 47.37 ± 9.83 years). There was no significant difference between the CAP and control groups in terms of age or gender (both, p>0.05). The TT and SH levels were significantly lower (all p≤0.05), and the SS/TT levels were significantly higher (p≤0.05) in the CAP group compared with the controls. Table 1 summarizes the demographic data and laboratory findings of the CAP and control groups. Figure 1 shows the distribution of the TT levels (µmol/L) in the 2 groups. The correlations between the thiol/SS parameters and %PMNLs and CRP were evaluated in the CAP group. Correlation analysis showed significant negative correlations between the TT levels (p=0.005, r= -0.389) and SH (p=0.004, r= -0.402) and %PMNLs and the TT levels (p=0.002, r= -0.421) (p=0.009, r= -0.365) and SH (p=0.865, r= 0.027) and CRP (mg/L).
Demographic data and laboratory parameters in the CAP and control groups.

Distribution of the total thiol levels (µmol/L) in the community-acquired pneumonia (CAP) and control groups (p=0.001).
Discussion
This is the first study to evaluate thiol/disulfide homeostasis in patients with CAP. Thiols are antioxidant molecules that play an important role in the extracellular defense system.6,7,11 In the presence of oxidant molecules, proteins in cell walls and extracellular liquid become oxidized by the cysteine residue of the thiols.12 Thiols reveal disulfide bonds via this reaction. The oxidation of thiols is reversible.6 The thiol/disulfide balance entails that the physiological activities of the cell cycle play an important role.13 Many diseases are associated with oxidative stress, including malignancies, cardiovascular disease, and neurodegenerative disease.12 A standard approach for evaluating the response of biological systems to oxidative stress involves measuring the increase or decrease of a redox-sensitive molecule.14 There are few studies in the literature regarding the oxidant/antioxidant ratio in CAP. Duflo et al15 found that in plasma and bronchoalveolar lavage fluid, the levels of thiobarbituric acid reactant substances (TBARS), which constitute an index of the degree of oxidative damage, were increased significantly in patients who developed ventilator-associated pneumonia (VAP) compared with a non-VAP group. Moreover, alveolar glutathione peroxidase concentrations were lower in VAP. Trefler et al16 showed that TBARS levels were higher in CAP patients than in controls. Katsoulis et al17 evaluated the total antioxidant status (TOS) of 30 patients with CAP. They found that decreased serum TOS is associated with CAP. Muravlyova et al18 found that malondialdehyde and reactive carbonyl derivatives were significantly lower in CAP patients than in controls. Castillo et al14 showed that the antioxidant capacity of plasma, as well as glutathione and glutathione disulfide levels, were lower than in controls. In this study, we found that the total and native thiol pools were lower in patients with CAP compared with healthy controls. Moreover, the SS/TT ratio was significantly higher in the CAP group. An increased disulfide/TT ratio indicates that the thiol/disulfide ratio had shifted towards disulfide bond formation, and that oxidative stress was increased. Therefore, in CAP, the thiol/disulfide redox balance system shifted to the side of disulfide bond formation with increased oxidation.
Lung cells are vulnerable to the detrimental effects of oxidants.19 In the normal lung, there is a balance between antioxidants and oxidants in the airway lining fluid and extracellular spaces, which helps to maintain normal physiological functions.20 In respiratory tract infections, an influx and activation of phagocytes into the lower airways, protecting against invading microorganisms, has been observed.14,21 Polymorphonuclear leukocytes and macrophages eliminate these microorganisms via reactive oxygen species (ROS) and lysosomal enzymes. An increased systemic ROS concentration may be seen in respiratory tract infections.14 Reactive oxygen species released from PMNLs and macrophages cause tissue damage in respiratory tract infections.21 Lung cells release inflammatory mediators and cytokines/chemokines in response to oxidative stress.19 The neutrophil percentage and CRP are important prognostic parameters in CAP. Curbelo et al22 found that higher CRP levels and neutrophil percentage predicted the 30-day mortality in CAP. We found negative correlations between the %PMNLs and thiol levels (native/total). We think that the ROS released from the increased PMNLs in CAP patients decrease the thiol levels by oxidizing the thiols. We also found a negative correlation between CRP and the thiol levels (native/total).
The results of the current study suggest that an abnormal thiol/disulfide ratio is important in the etiopathogenesis of CAP. Evaluation of thiol/disulfide parameters in CAP can make a significant contribution to assessing and monitoring patients with CAP. Moreover, thiol sources may be beneficial in stabilizing the oxidant/antioxidant ratio in CAP. N-acetyl cysteine (NAC) is an excellent source of sulfhydryl groups.23 Therefore, thiol sources such as NAC could contribute to CAP treatment.
Study limitations
The study population was small. Dynamic thiol disulfide homeostasis can be affected by various diseases and conditions. Therefore, many patients were excluded from the study because they had comorbid diseases.
More extensive studies are needed to determine the prognosis and importance of thiols in CAP.
Several biomarkers have been used to predict the prognosis of CAP. Most of these are acute-phase proteins. However, information on the importance of oxidative stress in the etiopathogenesis of pneumonia is lacking. This study showed that the oxidant/antioxidant ratio shifted towards the oxidative side in CAP. Abnormal thiol/disulfide homeostasis could be an important factor in the pathogenesis of CAP and may be useful for evaluating the severity of the disease and treatment response. Future studies should investigate the importance of the thiol/disulfide redox state in the etiopathogenesis of CAP and answer the questions “Can thiol levels be used to predict the severity of CAP?” and “Are thiol resources useful for the treatment of CAP?”
Acknowledgment
We would like to thank Textcheck (www.textcheck.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 19, 2018.
- Accepted April 19, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.