


Abstract
Objectives: To compare analgesia nociception index (ANI) values, visual analog scale (VAS) values, and hemodynamic parameters in hysteroscopy patients who received remifentanil and dexmedetomidine during general anesthesia.
Methods: In total, 30 patients who underwent hysteroscopy between March and September 2016 at the University of Health Sciences Fatih Sultan Mehmet Health Research and Application Center, İstanbul, Turkey were included in this prospective study. Standard hemodynamic monitoring, ANI, and bispectral index (BIS) monitoring were applied to the patients. At 10 min prior to induction, 1 µg/kg of remifentanil was applied in Group R (n=15) and 1 µg/kg of dexmedetomidine was applied in Group D (n=15). After induction, sevoflurane was used for maintenance with dexmedetomidine at 0.2-0.7 µg/kg/hour in Group D and remifentanil at 0.05-0.5 µg/kg/minute in Group R. Perioperative and postoperative analgesia levels (ANI and VAS, respectively), hemodynamics, and complications were recorded.
Results: Even though the ANI levels in Group D were lower at the perioperative 5th and 10th minutes, the ANI values were between the targeted limits, except for the measurement after I-gel insertion, in both groups. Hemodynamic parameters were within normal limits, but the mean arterial pressures in Group R after induction, following I-gel placement, and at the perioperative 5th, 10th, and 20th minutes were lower and at postoperative 30th minute were significantly higher.
Conclusion: Dexmedetomidine and remifentanil are both efficacious agents for perioperative analgesia in hysteroscopy cases.
Most gynecological procedures are carried out with hysteroscopy, which is the main diagnostic and treatment method for endometrial pathologies. While hysteroscopy is regarded as a minimally invasive procedure, patients report experiencing pain, especially during cervical dilation. Pain during hysteroscopy is a serious cause of discomfort and makes exposing the intrauterine cavity more difficult.1 A 0.21% to 30% incidence of vasovagal syndrome has been reported as a result of pain during this procedure in non-anesthetized patients.2 Despite the short duration of the procedure, pain management retains its importance.
Remifentanil, a µ-opioid receptor agonist, has a short action duration with rapid elimination and is cleared independently of hepatic and renal functions. Despite its short acting time, it can result in respiratory depression.3 Dexmedetomidine, an α2-agonist, appears to be an ideal sedative and analgesic agent in light of recent publications.4-8 Conscious sedation without respiratory depression and a short acting time are its advantages. Myocardial depression with dexmedetomidine is not observed until high doses are reached.9 Remifentanil has been used for a long time to maintain balanced anesthesia; however, dexmedetomidine as an adjuvant has seen increasing interest.
Sufficient intraoperative anesthesia and analgesia with adequate suppression of the sympathetic response is a principle in anesthesiology practice. The Analgesia Nociception Index (ANI), which measures parasympathetic tonus under anesthesia, has arisen as a new parameter for the balance of nociception and analgesia, and thereby the adequacy of perioperative analgesia. Analgesia Nociception Index is a numeric value from 0 to 100 that reflects the parasympathetic tonus obtained by evaluating fluctuations in the R-R interval on electrocardiography with each respiratory cycle.10,11
This study compared the effects of remifentanil with dexmedetomidine on intraoperative pain levels in hysteroscopy cases in terms of ANI values; perioperative hemodynamics; and postoperative visual analog scale (VAS) scores, hemodynamics, and complications.
Methods
With the approval of the University of Health Sciences Fatih Sultan Mehmet Health Research and Application Center Ethical Board (FSM EAH-KAEK 2016/22) and after obtaining written informed consent, 30 patients aged 18 to 65 years, with an American Society of Anesthesiologists score of I or II, who underwent hysteroscopy between 15 March and 15 September 2016, were recruited to this randomized prospective study according to the principles of the Declaration of Helsinki.
Patients with known coronary artery disease, arrhythmia, diabetes mellitus, preoperative beta-blocker use, or known allergies to the drugs used in the study, unstable hemodynamics, and those requiring endotracheal intubation were excluded from the study. Patients were randomized into Group R (remifentanil group, n=15) and Group D (dexmedetomidine group, n=15) by the sealed envelope technique. The study was performed in the gynecological operation room.
After intravenous cannulation with a 20 G needle in the dorsum of the hand, a normal saline infusion was started. In the operating room, standard monitoring of blood oxygen saturation (SPO2), electrocardiography, non-invasive blood pressure, and bispectral index (BIS) values (Covidien, Dublin, Ireland) were established and basal values were recorded. Analgesia Nociception Index (MetroDoloris, Lille, France) values were monitored with 2 adhesive electrodes, one on the sternum and one on the 6th intercostal space at the anterior axillary line. An ANI value below 30 indicates severe pain, between 30 and 50 indicates moderate pain, between 50 and 70 is interpreted as sufficient analgesia, and above 70 indicates no pain.
At 10 min before induction as loading doses, the patients in Group R (n=15) received 1 µg/kg of remifentanil and patients in Group D (n=15) received 1 µg/kg of dexmedetomidine, both drugs in 20 ml of normal saline. Next, 2 mg/kg of propofol and 0.5 mg/kg of rocuronium were administered for induction of anesthesia. After the BIS values reached 40-60, I-gel was placed. Anesthesia was maintained with a 50% O2/50% air mixture, 2% of sevoflurane, and 0.05-0.5 µg/kg/min of remifentanil infusion for Group R and 0.2-0.7 µg/kg/hour of dexmedetomidine infusion for Group D. Bispectral index level between 40 and 60 was targeted. Oxygen saturation, heart rate, mean arterial pressure, end-tidal carbon dioxide, and ANI values were recorded after induction and at 5-min intervals perioperatively. Study drug infusions and anesthesia management were conducted by an anesthesiologist who was blinded to the patients’ groups.
Patients received 1000 mg of paracetamol and 0.1 mg/kg of ondansetron before the end of the intervention. Anesthetics were stopped at the completion of surgery and 2 mg/kg of sugammadex was applied intravenously. The supraglottic airway was removed with resumed spontaneous breathing. The duration of anesthesia, duration of surgery, time to removal of the I-gel from the end of anesthesia, time to respond to verbal stimuli, and ANI and VAS values after I-gel removal were recorded. Patients were transferred to the recovery room once the I-gel was removed and stable hemodynamics were assured.
A VAS was used to assess postoperative pain in the postanesthesia care unit on a scale from 0 to 10, with 0 for no pain and 10 for most severe pain. An anesthesiologist who was blinded to the groups evaluated the postoperative SPO2, heart rate, mean arterial pressure, and VAS score immediately after arrival in the postanesthesia care unit and at 5, 10, and 30 minutes after surgery. Any perioperative side effects were recorded. Patients were observed for at least 30 min in the postanesthesia care unit, and once the Modified Aldrete Score was 9 or higher they were transferred to the wards. During anesthesia and the postoperative period, a mean arterial pressure <60 mm Hg was considered hypotension and a heart rate <45 beats/min was considered bradycardia. The 2 groups were compared for analgesia (intraoperatively using the ANI and postoperatively using the VAS), hemodynamic parameters, recovery duration, and complications.
Statistical analysis
The primary outcome of the study was ANI at the perioperative 5th minute. In our pilot study on 5 patients for each group, we calculated a mean ANI value of 41.25 with a standard deviation of 15.37 in the dexmedetomidine group and a mean value of 65.50 with a standard deviation of 9.26 in the remifentanil group at the perioperative 5th minute. It was suggested that a sample size of 11 patients per group would be sufficient to detect differences significant at p<0.05 with at least 90% power in this study. We included 15 patients per group to compensate for possible dropouts.
Statistical Package for Social Sciences Version 22 (IBM Corp., Armonk, NY, USA) was used for statistical analysis, to determine the normal distribution of data. The Shapiro-Wilk test was used. Besides descriptive statistics (mean, standard deviation, and median), when comparing groups for quantitative data with normal distributions Student’s t-test was applied. The paired sample t-test was applied to compare quantitative data within groups. For qualitative data, Pearson’s Chi-squared test, Fisher’s exact test, and Yates’ continuity correction test were used. A Pearson correlation analysis was applied to analyze the association between parameters. Significance was set at p<0.05.
Results
The mean age of the 30 participants was 45.57±9.8 years. The demographic properties of the patients, anesthesia duration and operation duration were similar between groups (Table 1).
Demographic data of 30 patients with an American Society of Anesthesiologists (ASA) score of I or II, who underwent hysteroscopy.
Group D had significantly lower ANI values at the 5th (p=0.041), and 10th minutes of the procedure (p=0.041) than Group R. The ANI levels were below 50 after I-gel insertion in both groups (Figure 1). According to our in-group evaluations, the ANI level at the time of I-gel insertion was lower than the basal ANI value in Group D (p=0.00). Analgesia Nociception Index levels at the time of I-gel insertion was lower than the basal ANI value (p=0.027) and higher at perioperative 20th and 25th minutes in Group R (p=0,002 and p=0,001). When compared with Group D, the mean arterial pressure was lower in Group R after induction of anesthesia (p=0,029), at insertion of the supraglottic airway (p=0,002) and the perioperative 5th (p=0,002), 10th (p=0,010), and 20th (p=0,038) minutes, but higher at the 30th minute postoperatively (p=0,027). In-group evaluations revealed that the mean arterial pressure measurements throughout the study were lower than the basal value in both groups (p<0.05). The heart rate values in the operative period were similar but were significantly higher at the time of I-gel removal (p=0.003) and postoperative 5, 10, and 30 minutes in Group R (p=0.001). The heart rate values in Group R were similar to the baseline values, while the heart rate values in Group D were lower than the baseline values during the operative period based on in-group evaluations (p<0.05).

Comparison of analgesia nociception index levels between groups. Student’s t-test, *p<0.05, t - time
The time to I-gel removal and time to respond to verbal stimuli were significantly longer in Group D (Table 2).
Comparison of operation duration, anesthesia duration, time to I-gel removal, and response time to verbal stimuli.
The postoperative VAS scores were similar (Figure 2). Three patients had an additional analgesic requirement, and one patient had nausea in each group (p=1.000).
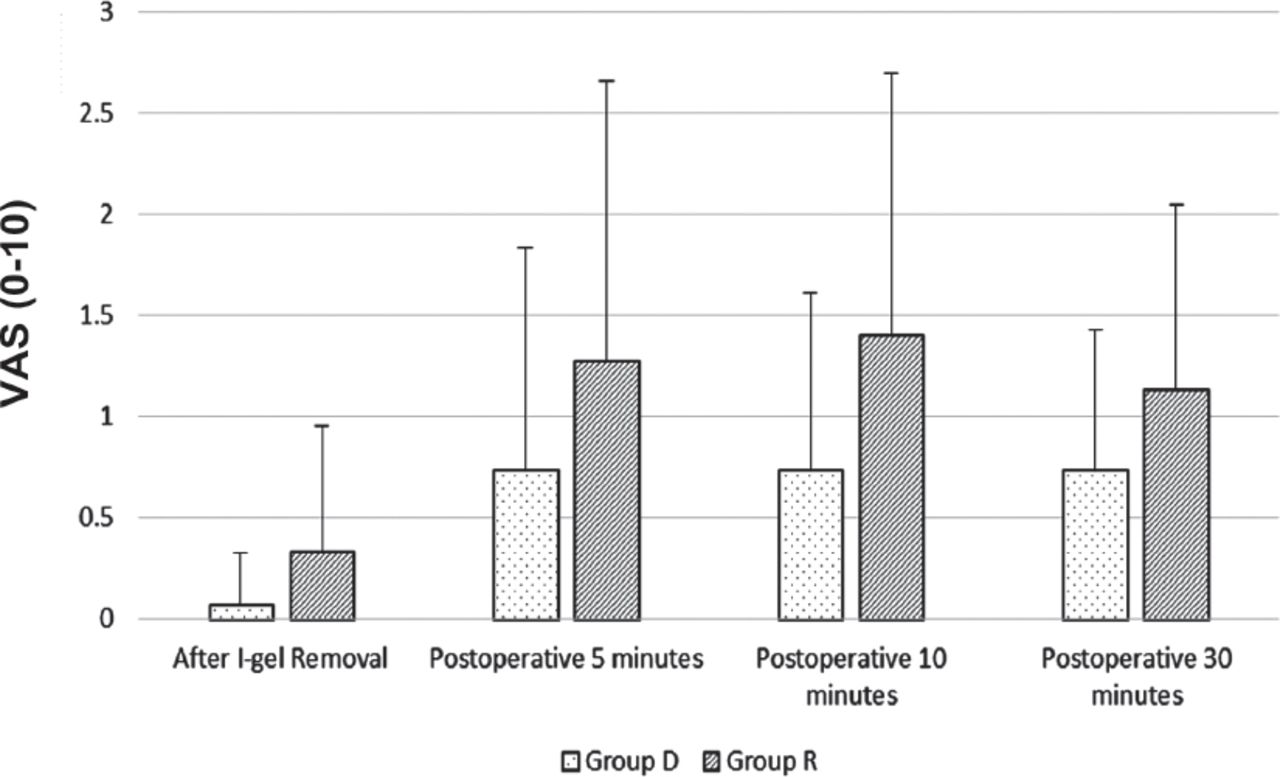
Comparison of visual analog scale (VAS) values between groups. Mann-Whitney U test
There were no differences in the perioperative and postoperative SpO2 and end-tidal CO2 levels between the groups. No intraoperative or postoperative side effects were observed during the study, and no patients were excluded after the study was initiated.
Discussion
Sympathetic system responses such as tachycardia, hypertension, sweating, mydriasis are indicators of the patient’s pain during surgery. Like hemodynamic parameters, respiratory parameters and sedation status that can be monitored under general anesthesia; numerical monitoring of pain can be advantageous for patient and anesthesiologist. Analgesia Nociception Index is a monitor used for this purpose that creates a numerical information by analyzing sympathetic system responses of unconscious patient. Thus, it may be o guide to measure the analgesic effects of drugs used in anesthesia.
This study investigated the effects of remifentanil and dexmedetomidine on pain, hemodynamics, and complications in patients undergoing hysteroscopy. The analgesic effects of remifentanil and dexmedetomidine were compared by ANI monitoring perioperatively. At the perioperative 5th and 10th minutes, the ANI was statistically higher in the remifentanil group but the ANI measurements of both groups were in the target range (50-70). In the remifentanil group, the mean arterial pressure readings in the perioperative first 20 min were lower, and the heart rate values in the postoperative period were higher, than in the dexmedetomidine group. In the postoperative period, because ANI could be effected in the awaked patient, VAS was used to assess the analgesic effects of the 2 drugs. As with the perioperative period, the 2 agents showed similar analgesic effects after anesthesia. The time to respond to verbal stimuli and time to removal of I-gel were higher in patients who received dexmedetomidine. In a study that investigated the effects of remifentanil and dexmedetomidine on pain during chest tube removal, assessed by a numerical rating scale, dexmedetomidine provided better analgesia during the procedure.12 In our study, at the time of I-gel insertion the ANI values were similar but were lower than the target limits in both groups. Both agents failed to suppress pain during I-gel insertion. At the 5th and 10th perioperative minutes, the ANI values were significantly higher in the remifentanil group, while both groups had ANI values above the targeted cutoff point for analgesic effect; both groups had adequate analgesia levels after I-gel insertion. Analgesia Nociception Index values were also recorded after removal of the laryngeal mask airway, and the values were similar at this point. It was thus observed that the 2 agents have adequate analgesic effects in the intraoperative and emergence periods. Our study is the first to use ANI monitoring to compare the perioperative analgesic effects of these 2 drugs. Several studies have compared the intraoperative use of remifentanil and dexmedetomidine.4-7 In a study comparing dexmedetomidine and remifentanil in spinal fusion surgery, dexmedetomidine caused a more prominent drop in intraoperative arterial pressure and heart rate.8 A study of craniotomies noted lower postoperative mean arterial pressures in the dexmedetomidine group.4 In our study, while the mean arterial pressure levels were within normal limits but lower than the basal values in both groups in all measurements, in the remifentanil group they were significantly lower within the first 20 min after induction and higher at postoperative 30 min. The perioperative heart rate was similar in the 2 groups but was lower in the dexmedetomidine group at I-gel removal, and at the 5th, 10th, and 30th minutes postoperatively, and these values were also lower than the baseline values of the same group. These differences in postoperative mean arterial pressure and heart rate indicate that dexmedetomidine may be better at suppressing the hemodynamic response during I-gel removal and the postoperative period. Current findings suggest that remifentanil is a better choice for controlled hypotension. In a study comparing remifentanil and dexmedetomidine, it was shown that patients receiving dexmedetomidine had a higher sedation score following extubation and a lower postoperative pain score.8 In another previous study, the authors concluded that remifentanil resulted in earlier eye opening, spontaneous ventilation, and tracheal extubation, but no difference in time of stay in the recovery room.13 Another study revealed a later postoperative response to verbal stimuli with dexmedetomidine.14 In our study, the time to I-gel removal and time to respond to verbal stimuli were longer with dexmedetomidine, which is explained by its longer duration of action than remifentanil. A study comparing remifentanil and dexmedetomidine found a lower additional postoperative analgesic requirement in the remifentanil group.13 Another study has shown a lower additional analgesic requirement with dexmedetomidine.14 We did not find any difference between the groups in their postoperative VAS scores, and three patients from each group required additional analgesic treatment. A study of obese patients comparing remifentanil and dexmedetomidine found no difference between the groups in terms of postoperative nausea and vomiting (PONV).13 In another study, 0.3 mg of ramosetron was administered for prophylaxis, and the authors found a lower incidence of PONV with dexmedetomidine.14 In our study, the patients received 0.1 mg/kg of ondansetron before the end of surgery, and the PONV incidence was similar between the groups. Turan et al15 reported the significance of ANI monitoring for perioperative analgesia in patients undergoing spinal surgery. Daccache et al,16 in their prospective study, concluded that ANI monitoring guides remifentanil dosing, and this results in low opioid consumption. Another study, while finding ANI measurements reliable in the sedated patient, pointed out that they may not be as reliable on the awake patient.17 According to Ledowski et al,18 the ANI was more valuable for patients under anesthesia. Jess et al19 pointed out that the ANI did not allow the differentiation of painful and nonpainful stimuli in alert patients. Intraoperative ANI monitoring was used in our study to compare the analgesic properties of the 2 agents and to circumvent external influences on the ANI; thus, we opted for a VAS in the postoperative period. To evaluate pain at removal of the supraglottic airway, we utilized both a VAS and the ANI, with no differences between groups.
Study limitations
The limitations of our study include the short infusion durations of the drugs and the limited number of samples. Another limitation is the lack of recorded sedation scores in the recovery room; if sedation scores had been evaluated, they might have been higher in the dexmedetomidine group because of the drug’s longer duration of action. In addition, because the study group was composed of women, it is difficult to generalize our results to the general population.
According to ANI measurement; dexmedetomidine and remifentanil are both sufficient and efficacious agents for perioperative analgesia in hysteroscopy patients.
Acknowledgment
We would like to thank Textcheck (www.textcheck.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received May 17, 2018.
- Accepted August 22, 2018.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.