


Abstract
Objectives: To develop a low-cost biomaterial-covered chest tube simulation model and assess its possible usefulness for developing the chest tube insertion skills among medical interns.
Methods: This mannequin-based interventional study was performed in a University hospital setting. We included 63 physicians performing emergency medicine internship at the Faculty of Medicine, Karadeniz Technical University, Trabzon, Turkey, between January 2015 and March 2015. A dummy was prepared for training simulation using a display mannequin. Medical interns received instruction concerning pneumothorax and the chest tube procedure. A total of 63 medical interns participating in this interventional study were asked to insert a chest tube in a biomaterial-covered mannequin. A senior trainee scored their performance using a check list and the mean of the total scores was calculated (21 items; total score, 42).
Results: The mean procedural score was 40.9 ± 1.3 of a possible 42. The maximum score of 42 was achieved by 39.7% of the medical interns, while another 33.3% achieved a score of 41. Of the participants, 85% succeeded in inserting the tube via an appropriate technique, achieving a score of 40 or more.
Conclusion: Our results indicated that this model could be useful for effective training of medical interns for chest tube insertion, which is an important skill in emergency medicine. This biomaterial-covered model is inexpensive and its use can potentially be widened to improve training methods without significant financial demand.
Chest trauma, with associated pneumothorax and hemothorax, is a commonly encountered condition in multitrauma patients. Management of these patients in the emergency department, with chest tube insertion in indicated cases, is of vital importance. Insertion of a chest tube requires manual skill and experience. Physicians lacking the means to sufficiently acquire this skill subsequently may experience difficulties with patient management. The risk of complications with this procedure, such as bleeding, and vascular and solid organ injuries,1-4 is high among inexperienced physicians. Providing adequate training and enhancing skills during medical training are important. Simulation-based practice provides an important tool for this purpose. Training physicians in a simulation-based setting improves performance on living patients, as they will be better able to manage patients with pneumothorax or hemothorax.1,3-5 Teaching of procedures during medical training is a serious concern.5 Theoretical and web-based instruction in training before graduation often is insufficient in the teaching of practical procedures. Therefore, physicians may encounter medicolegal problems. For ethical and legal reasons, theoretical and practical instruction must be improved in present-day medical training. At the same time, practical training is essential for future practitioners to develop their skills with interventional procedures and also their self-confidence. However, various difficulties arise in terms of costs of tools and equipment used in practical instruction, as well as the establishment of continuity and routine. This makes practical training sessions even more problematic. Efforts have been made to develop alternative solutions with commercial simulation models produced for chest tube insertion.5-7 However, these efforts still involve difficulties in terms of costs and availability.
Our primary objective was to design a simple, inexpensive simulation model that would help medical students practice chest tube insertion and thereby gain confidence. We developed a chest tube simulation model that can be applied easily anywhere for the acquisition of chest tube insertion skills. At the same time, we assessed the chest tube skills of medical interns using this model.
Methods
Study design and setting
We studied 63 physicians performing emergency medicine internships at the Karadeniz Technical University Medical Faculty between January 2015 and March 2015. Ethical approval was received from the institutional ethical committee (Protocol no. 2017/60).
Selection of participants
Only those emergency medicine interns without any theoretical knowledge and practical experience with chest tube insertion were included in the study.
Intervention
The simulation model was developed using a display mannequin (Trabzon, Turkey). To construct a satisfactory and effective, close-to-reality simulation model, we looked for a low-cost display mannequin with an anatomic shape and size comparable to those of a real adult.
All procedures were performed in a simulated operation room. Required equipment for this procedure included sterile gloves, antiseptic solutions, a sterile cover, local anesthetics, multiple types of syringes, suture materials, clamps, a chest tube, an underwater seal drainage system, and sponges. The first stage in the preparation of this simulation model was acquisition of the display mannequin. The second involved preparation of cutaneous and subcutaneous structures from chicken meat and skin. We obtained the display mannequin for $40 from a clothing store supplier. The mannequin was of normal human size, made of polyester, 180 cm in height, and 8 kg in weight. However, a mannequin consisting of a trunk only can be obtained easily online.
We then constructed “ribs” and “intercostal spaces” in this mannequin, with the assistance of an employee from the technical services department. We drew lines where the 3rd, 4th, 5th, and 6th ribs should be on the right side of the thoracic region. We then drilled out the “intercostal spaces.” This resulted in the formation of “ribs” and “intercostal spaces” on the mannequin. Again using the drill, we opened small holes for screws to attach the chicken meat around these ribs. We then prepared 3 sections of 10-cm packaging tape, at a cost of $2. These sections were inserted from the lower part of the mannequin for the purpose of simulating the pleura, and were attached to the interior of the “ribs” and the “intercostal spaces.” It took 30 minutes to reach this stage from acquisition of the mannequin.
Chicken breast was used to simulate cutaneous and subcutaneous tissues. At this stage, a local butcher prepared a piece of chicken breast approximately 15 × 10 cm and 1-1.5 cm thick in line with our instructions. Chicken skin of the same dimensions also was prepared. Chicken meat was placed in plastic wrap and then screwed onto the mannequin to simulate subcutaneous tissue. Separately, we prepared chicken skin then was screwed over the chicken meat inside the plastic wrap to simulate cutaneous tissue (Figure 1). We used one piece of chicken skin and breast for 5 to 6 procedures, after which they were replaced with new specimens. The preparations at the butchers and application took approximately 30 minutes, at a cost of approximately $5. Thus, the simulation model was made ready for use. Together with minor materials, such as plastic wrap and screws, the total cost of this model was $50, and the total preparation time was 60 min. We believe that the costs and preparation time are acceptable.

Photograph of the A) preparation of the display mannequin and determination of the costal lines, B-C) forming intercostal spaces with a drill, D) opening small holes for screws, E) simulating the pleura, F) using chicken breast meat to simulate cutaneous tissues, and G-H) using chicken skin to simulate subcutaneous tissues.
We asked 3 senior emergency medicine interns with previous experience with chest tube insertion to perform the procedure on the prepared simulation model. They compared each stage of the simulated procedure to that of the real procedure and reported that our simulation model approximated reality quite closely. We concluded that this model was applicable for chest tube insertion. Additionally, 3 residents and one lecturer prepared a training video demonstrating our chest tube insertion model step-by-step. Since one of the residents was experienced in recording and taking videos, no costs were incurred for the video recording.
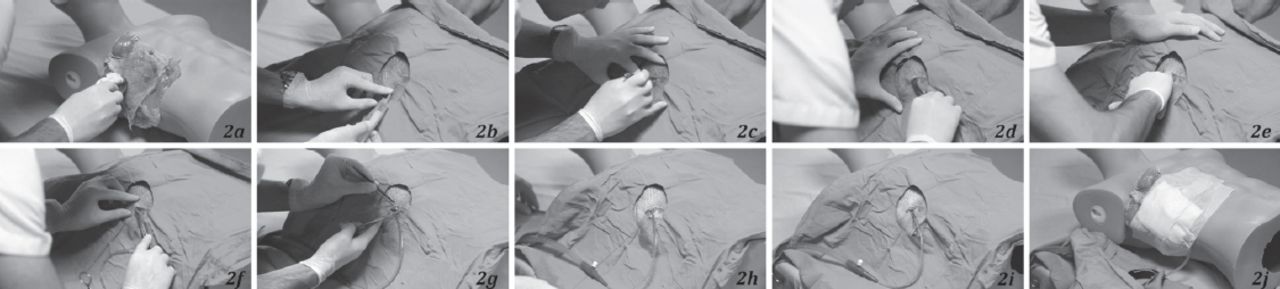
Medical interns under training at the Medical Faculty, Karadeniz Technical University attended a group presentation concerning chest trauma, pneumothorax, hemothorax, and chest tube insertion. During this interactive didactic session, the medical interns received detailed, step-by-step theoretical information concerning the indications for chest tube insertion, complications, and how the procedure should be performed. They then were shown the training video prepared using a model made from the mannequin. During this training video, all procedures required for chest tube insertion were demonstrated in a step-by-step manner (Figure 2). Thus, theoretical and practical instruction was completed.

Photograph depicting the steps of the chest tube insertion on the developed mannequin. A) Equipment preparation, protective measures, identification of the correct site for chest tube insertion and antiseptic application. B) Application of sterile cover and performing local anesthesia; C) incision; D) dissection of subcutaneous tissues in the incision site using a clamp, progression toward the upper costal margin with blunt dissection, accessing the pleura and entering the thoracic cavity with appropriate maneuvers and forming a cavity in the pleura by expanding the clamp when the pleura were entered; E) feeling the pleura by hand along the dissection line. F) Selection of an appropriate size chest tube and grasping this at both ends by clamping. G) Pushing the tube along the dissection line and inserting it by opening the clamp at an appropriate distance. H) Attaching the other end of the clamp to the underwater seal drainage system at an appropriate distance and performing oscillation control. I) Fixing the tube to the chest wall using a ‘U’ suture technique; J) Closure of area, confirmation of tube position with chest x-ray, and disposal of all waste products and hand washing.
Each medical intern subsequently was asked to perform the procedure on the model. Chest tube insertion skills were assessed using the equipment and the order set out in the chest tube insertion skill check list that we developed (Table 1). Each step in this list was scored separately as: skill score 0, incorrect application or complete overlooking of a step; skill score 1, correct performance of a step and at the correct time but without smooth transition to that step; and skill score 2, correct performance of a step and at the correct time with a smooth transition to that step. A mean value subsequently was calculated from the total scores awarded.
Chest tube insertion skill check list used in 63 interns participated in the study.
Data analysis and statistics
Descriptive data were analyzed using the Statistical Package for Social Sciences version 23 (IBM Corp., Armonk, NY, USA). Data regarding the age and gender demographic characteristics, as well as the procedure performance of each participant were evaluated by using the chest tube insertion skill check list.
Results
A total of 63 interns participated in the study: 34 (54%) were male and 29 (46%) were female. Mean age was 23.9 ± 3.5 years. No intern had ever performed chest tube insertion before. When asked to rate the simulation training for development of chest tube insertion skills, all interns awarded a score of 4, thus describing it as completely adequate. The highest total score was 42 according to the procedural performance skill scale. The mean procedural performance skill score was 40.9 ± 1.3. maximum score of 42 was achieved by 39.7% of the interns (n=25), while 33.3% received a score of 41 (n=21) and 85% succeeded in properly performing the chest tube insertion procedure with a score of 40 or more (Table 2).
Chest tube insertion procedure scores of 63 interns participated in the study.
Discussion
Medical interns may encounter cases of pneumothorax and hemothorax, which are life-threatening conditions that may occur as a result of trauma and/or spontaneously, in the early stages of their professional lives following graduation. They can save patients’ lives through timely and accurate intervention in these conditions. Although they may acquire theoretical knowledge during their medical training, they do not have enough practical opportunities to actually perform the procedure. There is little possibility of providing practical chest tube insertion training for medical interns at the bedside and allowing each intern to perform the procedure on a real patient. Therefore, simulation offers an effective manner for these physicians to acquire this skill. Several studies have shown that simulation-based instruction is effective for chest tube insertion.2,5-7 The most important problem with simulation training is the high cost. Other difficulties include maintenance expenses, the need for a separate simulation team, and problems with organizing the training. Also, it is not possible for this infrastructure to be available at all centers providing medical training. Alternative simulation methods may be effective in teaching such an important procedure. For these reasons, new and cost-effective approaches are needed in the practical training of medical students. Therefore, we sought to develop a low-cost model that can be applied everywhere and bears close similarity to the real chest tube insertion procedure. This mannequin, produced at a cost of $50, can be made easily by anyone. The instruction we provided using this model was highly adequate in terms of developing satisfactory chest tube insertion skills in our medical interns. The chicken skin we used in the model created an effect very close to that of human skin. The subcutaneous tissue dissection procedure was simulated by chicken meat pressed between plastic wrap to mimic subcutaneous tissues. Packaging tape representing the pleura was placed on the inner surfaces of the dummy. At this stage, the pleura were accessed, and pleural dissection and entry into the pleural cavity was simulated using slightly greater, but controlled force. The stages involved in the chest tube insertion procedure were performed in such a way as to mimic the real procedure. Of our medical interns whose chest tube insertion skills were assessed, 85% used a correct technique. In addition, the medial interns reported that this simulation model would be of great assistance in helping them grasp the chest tube insertion procedure. They also provided feedback to the effect that they would easily be able to apply the skills they acquired with this model when they encountered a real case in a clinical setting.
Previous studies have simulated the human chest using animal cadavers, such as pig or chicken. Other studies have used human cadavers, living animals, or mannequins.2,6,8-10 However, various problems have been reported in these studies, such as high equipment costs, difficulty in the model being used by one student after another, and inability to demonstrate the steps of the procedure in the correct sequence.7,9-11 One study reported an 80% success rate with chest tube insertion simulation training among medical interns at the Nippon Medical Faculty in Japan using an alternative simulation mannequin.12 Despite being more advantageous in terms of costs compared to commercial simulation mannequins, that model still was expensive. Another study, involving lower costs and using partial animal tissues in a manner similar to our study, simulated the thoracic cavity using a plastic box.13 We believe that the use of a dummy mannequin resembling the human body provided a greater resemblance to reality in our study.
Our aim of this study was to encourage chest tube innovation, and to overcome the cost and commercial availability barriers. Although this simulation model was developed for medical interns, it also may be useful for thoracic surgery and emergency medicine residents, advanced nursing practitioners, general practitioners, and other medical specialists. The risk of procedural complications can be reduced and physician experience can be increased using repeatable, low-cost procedures. Of course, training involving the simulation model alone will not be sufficient. Practice involving real cases will represent a complementary component of this training.
Study limitation
Lack of validation studies and data concerning similar training simulation models are the major limitations of our study. No preliminary test was applied to assess the experience and knowledge of the students receiving this training. In addition, it is impossible to assess potential complications using this model. Other limitations of this study include the fact that this model, made of chicken meat and plastic wrap, does not entirely correspond to human flesh and is unable to represent other characteristics of living humans.
In conclusion, on the basis of this study, in which theoretical and practical instruction in chest tube insertion procedures was provided and assessed using a scoring system, we believe the chest tube simulation model we developed can be used easily and at low cost in the training of interns
Illustrations, Figures, Photographs
All figures or photographs should be submitted in a high resolution (minimum 300 DPI) electronic version saved in jpeg or tiff format. Original hard copies of all figures may be requested when necessary. Photographs will be accepted at the discretion of the Editorial Board. All lettering, arrows, or other artwork must be done by an artist or draftsman. If arrows are used please ensure they appear in a different color to the background color, preferably black with a white border, or white with a black border. If arrows distinguish different items on the figure then different arrow styles should be used ie. long, short, wide, narrow. Written informed consent for publication must accompany any photograph in which the subject can be identified. Written copyright permission, from the publishers, must accompany any illustration that has been previously published.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received May 30, 2017.
- Accepted August 2, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.