


Abstract
Objectives: To study and evaluate the first phase of the Saudi Central Board for Accreditation of Health Institutions (CBAHI) in primary health care (PHC) accreditation cycle.
Methods: A descriptive analytical study of to evaluate 93 PHC survey visits in 20 regions, over the period October 2016 to May 2017.
Results: In the period October 2016 to January 2017, only 28 out of 93 PHC center (30%) targeted PHC in phase-1 were surveyed, 8 PHC got accredited (29%), while 11 PHC received conditional accreditation letters (39%) and 9 PHC were denied the accreditation (32%). During February 2017 to May 2017 visits were shifted to one day site visit, all the health care facilities training’s workshops were completed and the mock survey visits were started to precede the real survey visits, Since then, 65 PHC centers were surveyed (70%). At this time 47 PHC centers were accredited (72%), while 9 PHC were conditionally accredited (14%), and another 9 PHC were denied the accreditation (14%). Overall, 55 out of 93 PHC accredited (59%), 20 PHC got conditional accreditation (22%), and 18 PHC were denied the accreditation (19%).
Conclusion: Surveys per month were doubled with the one-day visit site visit. Both the intensive training and mock visits, showed a great impact as the accreditation and conditional accreditation status were increased by twofold due to better understanding of the PHC staff about the standards, as well as early identification of performance gap which allowed the PHC to mitigate these gaps sufficiently enough to avoid zero scores especially in the ESR requirements.
In the dawn of the evidence-based health practice and information technology era, healthcare institutions struggle with paradoxes of vast varieties.1 They need to focus on multiple goals, such as medical education and patients’ health care through different strategic axes like managerial, professional, technocratic, and others.2,3 They must allow the medical staff to exercise their clinical judgments while promoting the standardization of practices.4 They must act autonomously and innovate, in coordination with other related health providers, to meet their goals and the community expectations. This has been established to increase pressure to improve performance, as many publications have reported serious limitations in the quality and safety of health care practices.5 One important mean of tackling this burden is accreditation. Accreditation for healthcare institutions involves an accrediting body surveying and verifying compliance with recognized criteria/standards.6 It has been considered as a useful tool to establish national standards and reduce variations in medical practice,7 it has been shown to mitigate inappropriate medical care8 and improve the cost-effectiveness especially in with strict and recessive economy. One study showed that almost 95% of contracted services made by health care governing companies in the United States are with accredited health care facilities.9 This demonstrates that accreditation status of health care facilities plays a major role in the health care clients’ decisions. Failure of an organization to go through an accreditation process may indicate that the facility is not open to external evaluation of its performance.10
There are many international accrediting bodies to evaluate the quality and patient’s safety in health care institutions, yet the Saudi Central Board for Accreditation of Healthcare Institutions (CBAHI) is the only national agency authorized to grant accreditation certificates to all governmental and private healthcare facilities operating in Saudi Arabia. CBAHI has emerged from the Saudi Health Council as a non-profit organization.11 The principal function of CBAHI is to set the healthcare quality and patient safety standards against which all healthcare facilities are evaluated for evidence of compliance.
The Primary health care centers’ general directorate of the ministry of health in Saudi Arabia decided to utilize CBAHI to evaluate 2386 Primary Health care (PHC) centers affiliated to its own administration aiming to ensure high-quality standards and safe health care environment. The general directorate of PHC centers in MOH selected 502 PHC centers in 20 regions as a target in the period between October 2016 and May 2020 in 4 consecutive phases. The aim of this descriptive analytical study is to highlight the result of the 1st phase of CBAHI PHC accreditation cycle in Saudi Arabia.
The objective of this study is to highlight the results of the 1st phase of CBAHI PHC accreditation cycle in Saudi Arabia, including the accreditation decision status, the impact of 3 mid-cycle interventions, and the most scored essential safety requirements (ESR) standards.
Methods
A descriptive analytical study that involved 93 PHC centers visited for survey in 20 regions within Kingdom of Saudi Arabia (KSA) to evaluate their compliance with national primary health care standards by CBAHI, over the period from October 2016 to May 2017. It represents the 1st CBAHI accreditation cycle of the PHC facilities affiliated to the ministry of health in KSA. Visits were conducted by 28 surveyors who received intensive cross training all over the 23 chapters to evaluate Leadership, Manpower, Management of Information, Quality Management and Patient Safety, General clinics, referrals, Health Record, Dental and Oral Health, Patient and Family Rights, Health Promotion and Education, Radiological Services, Maternal and Child Health, Immunization, Communicable Diseases, Non-Communicable Diseases, Geriatric Care, Environmental Health, Emergency Services, Community Participation, Facility Management and Safety, Infection Prevention and Control, Laboratory Services, and Pharmaceutical Services.
Each survey visit was commenced by 2 surveyors, over 1-2 days’ survey agenda. The accreditation decision was done after robust reports review by health care accreditation specialists and the PHC surveyors’ team leader as well as in depth discussion by the accreditation decision committee. The accreditation decision matrix relies on three items; total score, Essential safety requirements (ESR) score, and the number of zero scored ESR. Table 1 demonstrate the cut points of the accreditation decision matrix:
Central Board for Accreditation of Healthcare Institutions (CBAHI) primary health care Accreditation Decision Matrix.
In the period from October 2016 to January 2017, the survey visits were conducted over 2 days ranging from 3-9 visits per month. In the period from February 2017 to May 2017, visits were only for one day through merging of evidence of compliance without any modification in the standards and/or the sub-standards which led to an increase of the survey visits to 12-20 visits per month. CBAHI also exerted an effort to educate and train 500 PHC centers’ staff through 10 workshops for Health care facilities orientation, aiming to improve their knowledge as well as understanding and compliance with the standards. All workshops were started by October 2016 and completed by end of February 2017. One more intervention was applied through mock survey visits by CBAHI-MOH surveyors to augment and support the standards implementation through early identification and analysis of performance gap.
Inclusion and exclusion
All the 93 PHC visits were included in the study and none were excluded.
Statistical analysis
Descriptive analytical were used to measures of central tendency frequency distribution and spread using Microsoft Excel 2016.
Results
In the period from October 2016 to January 2017, only 28 out of 93 PHC centers (30%) targeted in phase-1 were surveyed (Figure 1). Eight PHC centers got accredited (29%), while 11 received conditional accreditation letters (39%) and 9 were denied the accreditation (32%) (Figure 2).

Comparison between one day visit verses 2 days visits during February 2017 to May 2017.

Primary health care results of accredited, conditional accreditation, and denial between October 2016 and January 2017.
Since February 2017 through May 2017 visits were changed to a one-day site visit. Health care facilities training workshops and the mock survey visits now preceded the actual survey visits; afterwards 65 PHC centers (70%) were surveyed. Subsequently, 47 PHC centers were accredited (72%), 9 were conditionally accredited (14%), and another 9 centers were denied the accreditation (14%) (Figure 3). Overall, 55 out of 93 PHC centers were accredited (59%), 20 PHC got conditional accreditation (22%), and 18 PHC were denied the accreditation (19%) (Figure 4).

Primary health care results of accredited, conditional accreditation, and denial between February 2017 and May 2017.

Primary health care results of accredited, conditional accreditation, and denial between October 2016 and May 2017.
The highest total score was 98.87% and the lowest total score was 44.91%; both were achieved by PHC centers in the period from February 2017 to May 2017. The lowest essential safety requirements (ESR) score was 14.29% in the period from October 2016 to January 2017. A total of 25 out of 93 PHC centers managed to get 100% score in ESR. Three ESR were scored frequently as not met (zero score). The most frequently scored ESR as not met was GC.19.EC.1 (documentation of the plan of care in the patients’ health records) in 14 cases. The second most-commonly scored ESR deficiency was IPC.22.EC.5 (compliance in the central sterilization unit and sterilizations requirements) in 12 cases. The ESR of evaluation and completion of all the required items in prescriptions (PH.14.EC.2) was the third most common deficiency, in 11 cases.
Discussion
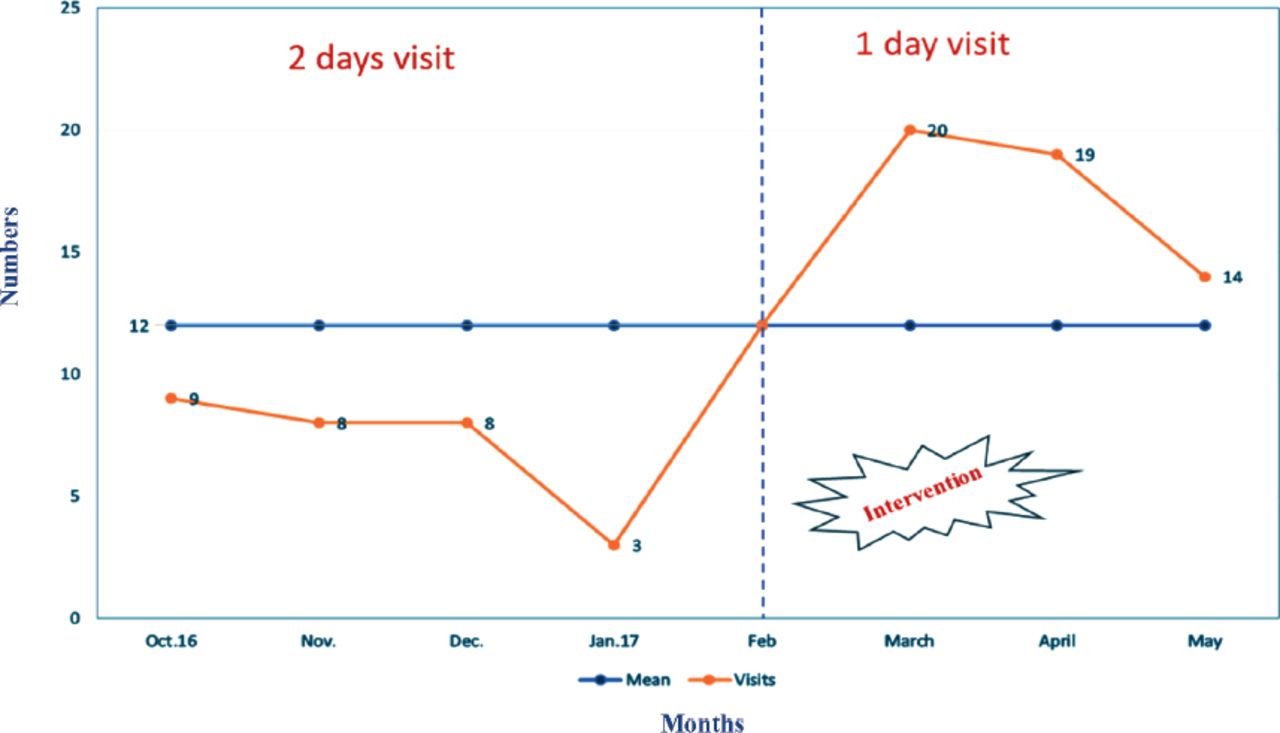
The PHC survey visits originally followed a 2-day agenda and, although the mean site visits per month was 12, the number of visits per month did not exceed nine visits. After four months, the CBAHI primary health care team reviewed the evidence of compliance and shortened the visits agenda without affecting the standards and sub-standards numbers or contents, through merging of evidence of compliance by focusing on the implementation rather than bulk documents review. Two pilot visits were conducted to evaluate the modification in the evidence of compliance and agenda, which showed no significant changes in survey visit accreditation status results, suggesting that shorter visits would not fail to find deficiencies due to lack of time. Thereafter, PHC centers were scheduled for one day visits, and the total number of visits per month increased to 20 visit per months (Figure 5). Clearly, the number of visits per month doubled with one day visits which could be explained by the increased availability of surveyors, who are all part-time employees of the CBAHI. The one day agenda reduced the interruption in their full-time job schedules.

Primary health care visits per month between October 2016 and May 2017.
Ten intensive training workshops to train 500 PHC staff from all over the 20 regions in Saudi Arabia in the targeted PHC centers were conducted through strategic collaborative relationship between CBAHI and MOH. Each workshop was conducted by senior CBAHI primary health care surveyors over 3 days. The workshop was intended to improve the ability of the staff to understand the intent of the standards and how to comply with the standards requirements, as well as the quality concepts and quality tools. Post-tests were conducted to ensure that the staff accomplished the objectives of the training.
Based on the improvement in accreditation results, the mock survey visits appeared to be of great help to the PHC centers as they assisted the PHC leaders and staff to identify the gaps for improvement and helped to focus their efforts to a significant few through utilizing what they have learned in the training workshop, in accordance with “the rule of 80:20” (namely, an economic principle of ‘factor sparsity’ which states the as much of 80% of an effect stems from only 20% of potential causes).
One limitation in this study, is that there is no comparison with international accreditation process and it was designed as a descriptive analytical theme to describe the first CBAHI Primary Health Care Accreditation Cycle in Saudi Arabia with the impact of 3 mid-cycle intervention.
In conclusion, the change to a one-day site visit doubled the number of visits efficiently while both the intensive training and mock visits showed a great impact in the results as the accreditation and conditional accreditation status were increased by 2 fold due to better understanding of the PHC staff about the standards as well as early identification of the performance gap which allowed the PHC to mitigate these gaps sufficiently enough to avoid zero scores especially in the ESR requirements.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 22, 2017.
- Accepted August 9, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.