


Abstract
Objectives: To validate the diagnostic performance of Hepa-Index in predicting different stages of hepatic fibrosis in Egyptian patients with chronic hepatitis C (CHC).
Methods: Hundred treatment naïve chronic hepatitis C Egyptian patients were prospectively enrolled between June 2014 and January 2015. They were subjected to: platelet count, alpha-2-macroglobulin (α2-MG), total bilirubin, gamma glutamyl transpeptidase (GGT), total cholesterol, liver biopsy and histopathological staging of hepatic fibrosis according to METAVIR scoring system. Hepa-Index was calculated according to the formula: Hepa-Index=exp (-0.021 x platelet +1.65 x α2-MG+0.2 x total bilirubin + 0.026 x GGT -1.215 x total cholesterol) / (1+exp (-0.021 x platelet + 1.65 x α2-MG + 0.2 x total bilirubin +0.026 x GGT -1.215 x total cholesterol).
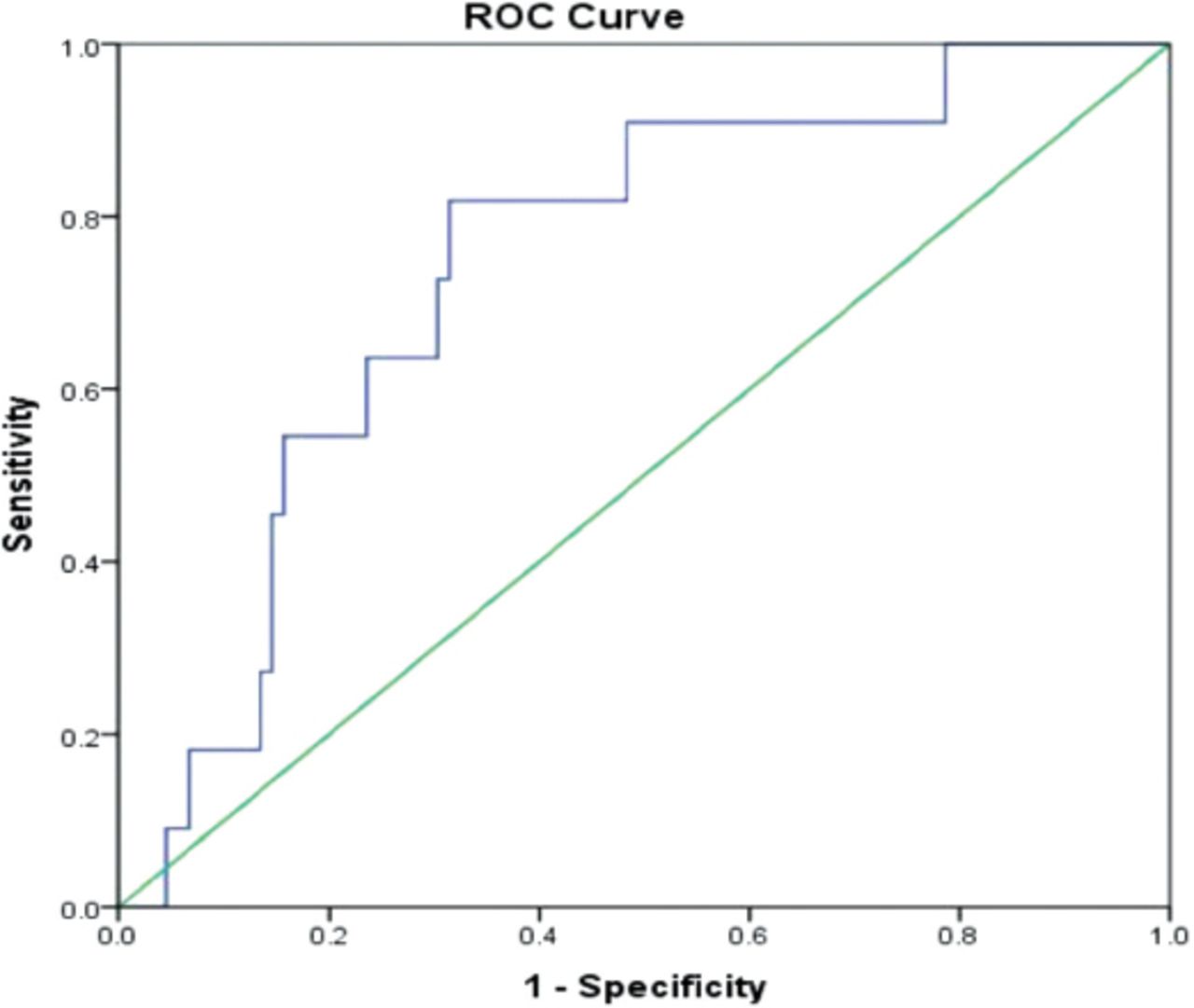
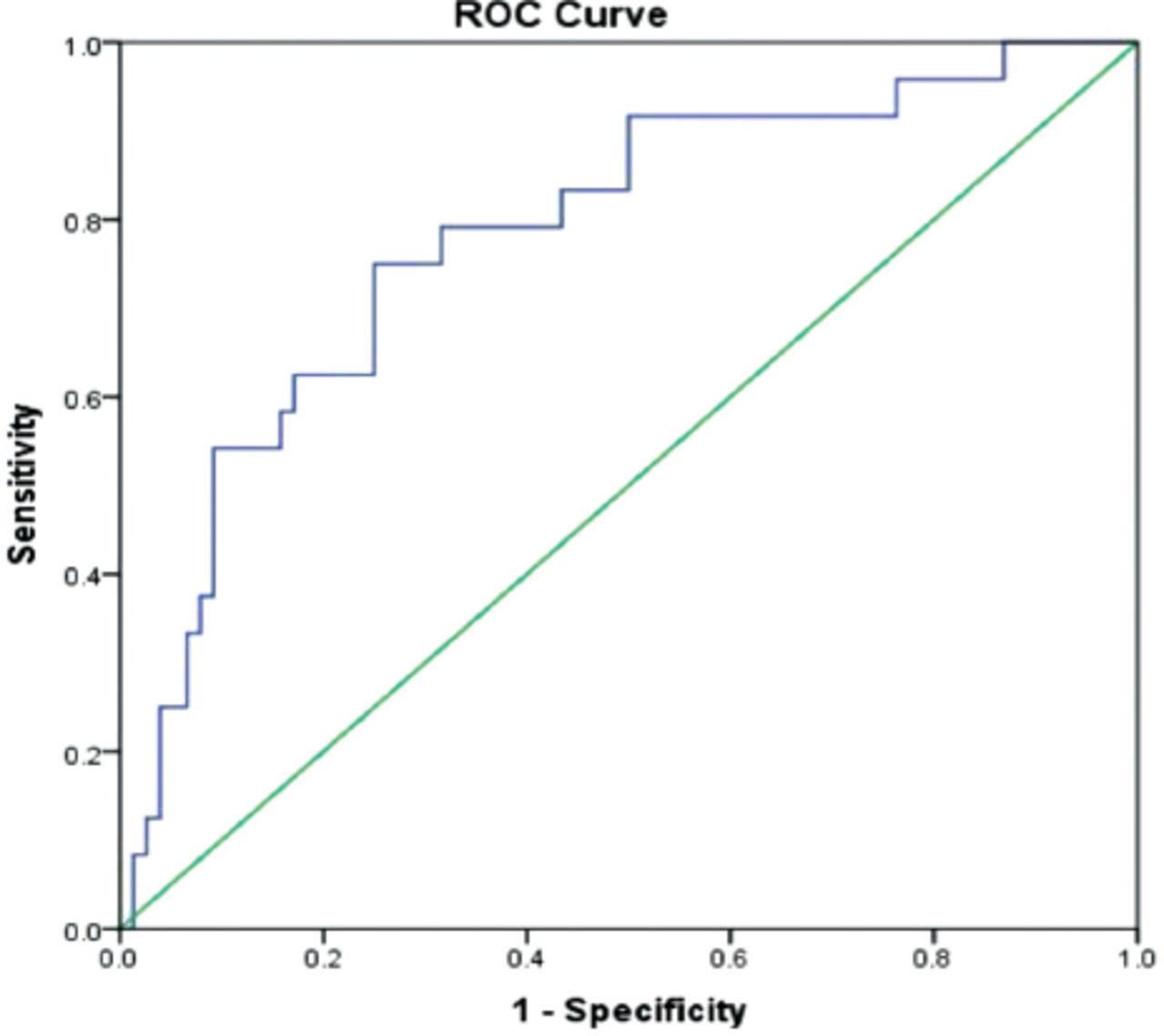
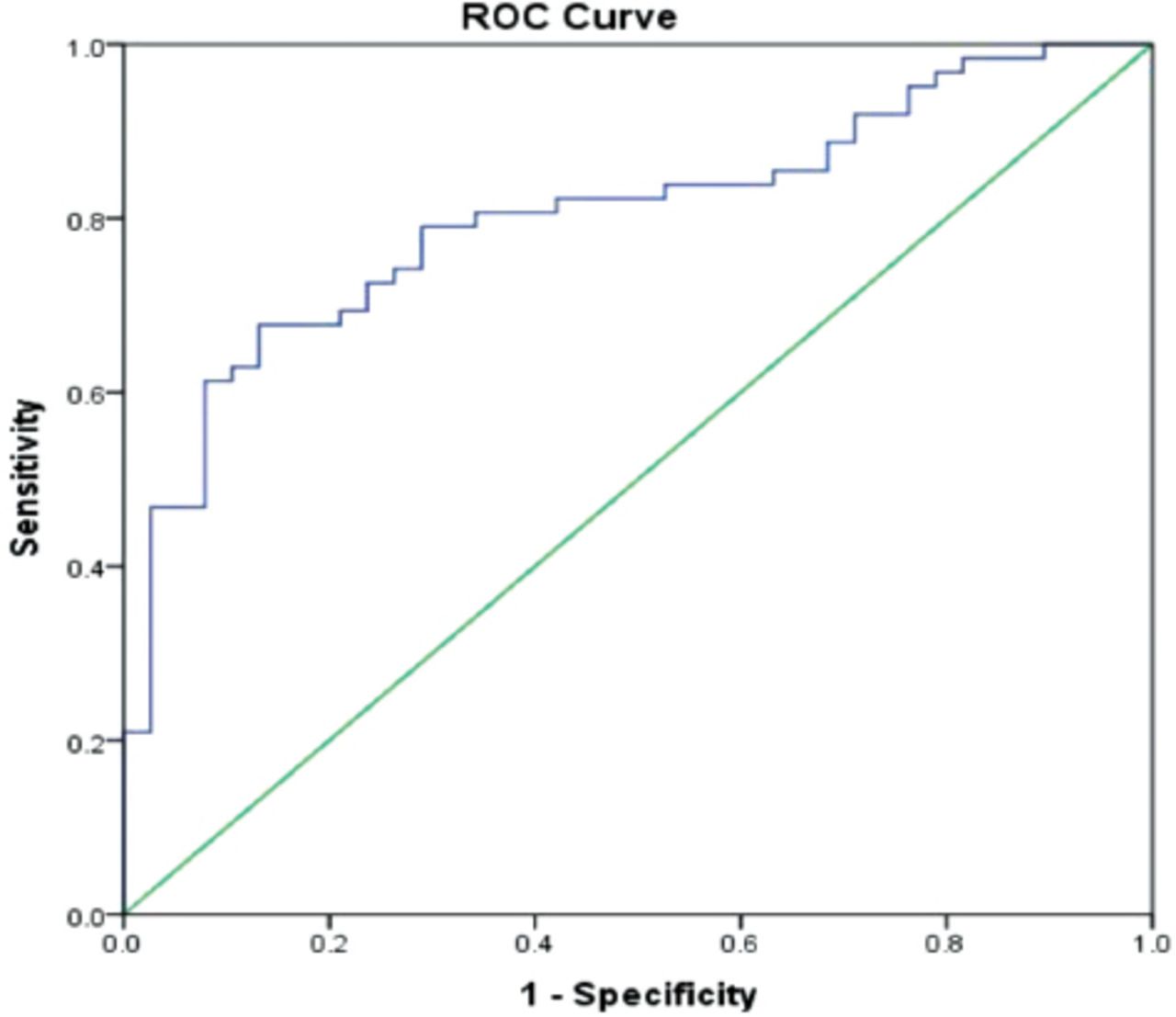
Results: Hepa-Index correlates positively with the stage of hepatic fibrosis. Cut off values of Hepa-Index were: 0.2 for predicting significant hepatic fibrosis (≥F2 METAVIR), 0.3 for severe hepatic fibrosis (≥F3 METAVIR) and 0.4 for cirrhosis (F4 METAVIR). Hepa-Index was able to detect significant fibrosis with sensitivity of 69.4%, specificity of 76.3% and AUROC of 0.803. Hepa-Index was also able to detect severe hepatic fibrosis with sensitivity of 79.2%, specificity of 64.5% and AUROC of 0.783 and cirrhosis with sensitivity of 81.8%, specificity of 68.5% and AUROC of 0.744.
Conclusion: Hepa-Index is a good non-invasive biomarkers panel that can be used for non-invasive assessment of hepatic fibrosis in chronic hepatitis C patients.
Staging of hepatic fibrosis is important for deciding about treatment initiation and treatment priority in chronic hepatitis C, it is also required to determine prognosis and to plan long-term screening for varices and hepatocellular carcinoma.1 The need for liver biopsy to assess liver fibrosis has markedly decreased over the last 2 decades due to discovery of different non-invasive methods2 that can predict not only stage of hepatic fibrosis but also long-term complications of chronic hepatitis with a level of accuracy sufficient for making proper clinical decisions.3,4 Non-invasive approaches includes serum biomarkers;5 different radiological tools,6 proteomics,7 glycomics8 and genetic markers of fibrosis.9 Serum biomarkers like aspartate aminotransferase (AST) to platelet ration index (APRI),10 FIB-4,11 FibroTest12 and many others have been developed and validated mainly in chronic hepatitis C. They gained popularity because they are fairly accurate, highly acceptable by patients and easily reproducible.13 However, these tests cannot replace liver biopsy in the present time as they less accurate in detecting intermediate fibrosis stages (F1-F2 METAVIR) than cirrhosis (F4 METAVIR). Development and validation of new non-invasive panels is still needed as long as there is no ideal non-invasive panel proved to be able to replace liver biopsy. Hepa-Index is one of the newly developed panels for non-invasive assessment of hepatic fibrosis. It has been developed from data of a heterogeneous group of patients including chronic hepatitis B, CHC, autoimmune hepatitis, alcoholic and non-alcoholic fatty liver disease patients in comparison to FibroTest and FibroScan.14 This study represents the first validation against liver biopsy for Hepa-Index in chronic liver disease patients. We aimed at exploring the accuracy of Hepa-Index in predicting different stages of hepatic fibrosis in CHC Egyptian patients.
Methods
We prospectively recruited 100 treatment naive CHC patients of any gender and body mass index and compensated cirrhosis in an observational study from our outpatient clinics between June 2014 and January 2015. Inclusion criteria included: treatment naive mono infected chronic hepatitis C Egyptian patients with compensated cirrhosis. Patients with other types of chronic liver diseases including: chronic hepatitis B, autoimmune hepatitis, alcoholic and nonalcoholic fatty liver disease were excluded. All patients were subjected to detailed history taking including demographic data (age and gender), full routine clinical assessment for manifestations of chronic liver disease in addition to the following investigations: platelet count, alpha-2-macroglobulin (α2-MG), total bilirubin, gamma glutamyl transpeptidase (GGT), total cholesterol, AST, Alanine Aminotransferase (ALT), total bilirubin, albumin, abdominal ultrasound and ultrasound guided percutaneous liver biopsy using 16 gauge semi-automated biopsy needles. Hepa-Index was calculated according to the following formula: Hepa-Index = exp (-0.021 x platelet +1.65 x α 2-MG+0.2 x total bilirubin + 0.026 x GGT -1.215 x total cholesterol) / (1+exp (-0.021 x platelet + 1.65 x α 2-MG + 0.2 x total bilirubin +0.026 x GGT -1.215 x total cholesterol).14 Liver biopsies were having at least 15 mm length and at least 4 portal tracts. Liver biopsies were fixed in 10% neutral formalin before processing and embedding in paraffin. Then they were stained with haematoxylin and eosin, and Masson trichrome. Stage of hepatic fibrosis was assessed according to METAVIR scoring system which scale liver fibrosis into 5 stages F0, F1, F2, F3 & F4 where (F0 denoting no fibrosis, F1 denoting portal fibrosis without septa, F2 denoting portal fibrosis with few septa, F3 denoting numerous septa without cirrhosis and F4 denoting cirrhosis).15 Grade of necro-inflammation was also assessed according to the METAVIR system which scales necro-inflammation into 4 grades; A0, A1, A2, A3 &A4 where (A0 denoting no activity, A1 denoting mild activity, A2 denoting moderate activity and A3 denoting severe activity).16 For purpose of statistical analysis; patients were further sub classified into three comparison groups; a group with significant hepatic fibrosis (≥F2), a second group with advanced hepatic fibrosis (≥F3) and a third group with cirrhosis (F4). Local research ethical committee approval was issued before starting data collection and a written informed consent was taken from each participant. The study protocol conformed to the ethical guidelines of the 2008 Declaration of Helsinki.
Statistical analysis
All data were processed using IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21 (IBMCorp, Armonk, NY, USA). Quantitative data was expressed as mean±standard deviation (SD) while qualitative data was expressed as frequency and percent distribution. Data were explored for normality. Comparison between quantitative variables was carried out by student T-test of 2 independent samples. Repeated measures Analysis of Variance (ANOVA) test was used instead of T-test when comparing between more than 2 groups of independent variables. Results were expressed in the form of p-values. Comparison between qualitative variables was carried out by Chi-Square test (X2). Binary correlation for ordinal variables was carried out by Spearman correlation test; results were expressed in the form of correlation coefficient (r) and p-values. Receiver operating characteristic (ROC) curves were generated by plotting the relationship of the true positivity (sensitivity) and the false positivity (1-specificity) at various cut-off points of the tests. An AUC of 1.0 is characteristic of the ideal test, whereas 0.5 indicates the test of no diagnostic value. Taking sensitivity and specificity into account, the cut-off points were selected according to max number of sensitivity and specificity. The diagnostic accuracy, sensitivity, specificity, positive predictive values (PPV) and negative predictive values (NPV) also were calculated. Both univariate and multivariate analyses were conducted, multivariate stepwise binary logistic regression analysis with significant fibrosis (F≥2), advanced fibrosis (F≥3) and cirrhosis (F4) - as the dependent factor - were done in comparison to the selected cut offs. A p-value was considered significant if ≤0.05.
Results
Our study included hundred treatment naïve Egyptian patients with chronic hepatitis C mono infection (67%, males and 33% females); their mean age (±SD) was 40.29 years (±10.98). Significant fibrosis (≥F2) was present in 62 patients, advanced fibrosis (≥F3) was present in 24 patients and cirrhosis (F4) was present in 11 patients, other general characteristics of the study population are summarized in Table 1. The mean values±SD of Hepa-Index parameters were: Platelets count (201.58±59.02 109/L), α2 MG (2.57 ±0.54 g/L), total bilirubin (13.89±3.60 umol/L), GGT (61.47 IU/L±54.10) and cholesterol (4.60 mmol/L±1.31). Hepa-Index was positively correlating with stages of hepatic fibrosis (F0-F4) r=0.65, p-value<0.001. Mean values±SD of different Hepa-Index variables in different fibrosis Stages (F0-F4 METAVIR) are presented in Table 2. Mean values±SD of Hepa-Index parameters in significant hepatic fibrosis (≥F2), sever hepatic fibrosis (≥F3) and cirrhosis (F4) are presented in supplementary Table 1. Different cut off values of Hepa-Index were tested for the ability to predict significant hepatic fibrosis (≥F2), severe hepatic fibrosis (≥F3), and cirrhosis (F4). The diagnostic value of the Hepa-Index was assessed by receiver operating characteristic (ROC) curve analysis, shown in Figures 1-3, which gave areas under the ROC curve (AUROCs) of 0.803 for the detection of significant hepatic fibrosis (≥F2), 0.783 for severe hepatic fibrosis (≥F3), and 0.744 for cirrhosis (F4). The chosen cut off values of Hepa-Index were: 0.2 for significant hepatic fibrosis (≥F2), 0.3 for severe hepatic fibrosis (≥F3), and 0.4 for cirrhosis (F4). Sensitivity, specificity, AUROC curve, positive and negative predictive values of selected cut off values of Hepa-Index for prediction of significant hepatic fibrosis (≥F2), severe hepatic fibrosis (≥F3), and cirrhosis (F4) are summarized in Table 3.
General characteristics of the study population.
Mean values±SD of Hepa-Index parameters with different fibrosis stages (METAVIR).

Receiver-operating curve for Hepa-Index for detection of significant hepatic fibrosis (≥F2).

Receiver-operating curve (ROC) for Hepa-Index for detection of severe hepatic fibrosis (≥F3).

Receiver-operating curve (ROC) for Hepa-Index for detection of cirrhosis (F4).
Selected cutoff values of Hepa-Index for detection of different stages of hepatic fibrosis.
Discussion
Serum fibrosis biomarkers are promising methods for staging hepatic fibrosis and monitoring both progression17 and regression of liver disease in chronic hepatitis C.18 Although their use is limited by being non-specific for the liver19 and cost associated with patented tests;5 they are well validated,20 they have good reproducibility and can be carried out in outpatient clinics.21
In this study, we did the first validation for Hepa-Index (a relatively new biomarkers panel for assessment of hepatic fibrosis) against liver biopsy in chronic hepatitis C. Hepa-Index showed good sensitivity, specificity, positive and negative predictive values, for predicting significant hepatic fibrosis, severe hepatic fibrosis, and cirrhosis in chronic hepatitis C patients. Hepa-Index performance is almost equal to the performance of different patented and non-patented noninvasive panels for assessment of hepatic fibrosis (FibroTest, FibroMeters, HepaScore, and APRI) which is reported to have an AUROCs ranging from 0.72 to 0.78 for detection of significant fibrosis and 0.77 to 0.86 for detection of cirrhosis.20 Hepa-Index as a serum biomarker panel carry the advantages of patented and expensive serum fibrosis biomarkers in addition to being free of charge and accurate in classifying significant hepatic fibrosis, advanced hepatic fibrosis and cirrhosis.
One more advantage of Hepa-Index over currently available tests like APRI, FIB-4, Forns index, FibroTest and FibroMeter is absence of transaminases (ALT and AST) in its formula which may lead to false positive results in acute hepatitis with use of other tests since all of them include serum levels of aminotransferases in their formulas. Although widely used and validated; APRI and FIB-4 are accurate only for the diagnosis of cirrhosis, but they are relatively inaccurate for the diagnosis of significant fibrosis in HCV-monoinfected patients. Radiological methods like transient elastography and magnetic resonance elastography are reliable for diagnosis of cirrhosis but they have some limitations. Transient elastography is unable to differentiate between intermediate stages of liver fibrosis, its applicability is less than serum biomarkers and has false positive results in acute hepatitis, hepatic congestion and cholestasis. Magnetic resonance elastography seems promising but needs more validation and requires magnetic resonance image facility in addition to its high cost.6 Combining Hepa-Index with transient elastography can increase diagnostic accuracy of both tests and warrants future investigations in prospective studies. Moreover; Hepa-Index can potentially be a marker for other different liver diseases like chronic hepatitis B, alcoholic liver disease and nonalcoholic fatty liver disease as evidenced in the first study of Hepa-Index.14 However, this needs to tested against liver biopsy in each chronic liver disease separately. This study has some limitations that should be addressed in future research: relatively small sample size has to be increased in future studies, our study included only chronic hepatitis C patients so validation in other chronic liver diseases (e.g. chronic hepatitis B, alcoholic liver disease, nonalcoholic fatty liver disease and autoimmune hepatitis) should be also considered. Our cohort of patients were all treatment naïve; so we do not know if Hepa-Index will be of value in monitoring regression of fibrosis in treatment context? Finally comparison with other noninvasive scores (namely, APRI, FORNS, FIB-4, and FibroTest) and transient elastography (FibroScan®) should be also carried out.
In Conclusion, Hepa-Index is a new panel of biomarkers that can be used as a non-invasive method for prediction of different stages of hepatic fibrosis in chronic hepatitis C. Hepa-index should be validated in larger number of patients and in different ethnic groups. Validation in other chronic liver diseases should be also carried out. Combination of Hepa-Index with transient elastography can be also an area of future research.
- Received June 7, 2017.
- Accepted August 31, 2017.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.