


Abstract
Objectives: To assess meningitis treatment in Lebanon’s compatibility with the Infectious Diseases Society of America (IDSA) guidelines and the effect of non-compliance on mortality.
Methods: This is a retrospective study, conducted in 5 Lebanese hospitals, and enrolling all patients diagnosed with meningitis who presented to the involved hospitals from January 2008 to December 2016.
Results: A total of 252 participants were enrolled in the study. Of these patients, 205 (82.7%) were diagnosed with viral meningitis and 47 (17.3%) with bacterial meningitis, which was confirmed using laboratory tests. For patients with viral meningitis, 128 (62.4%) remained on the initial prescribed antibiotics despite the negative cerebrospinal fluid (CSF) and blood culture results. For bacterial meningitis patients, 30.8% received treatment regimen incompatible with the IDSA guidelines. The most common reason for the treatment incompatibility was the definitive drug choice after the culture results (49.1%) and the least common reason was inappropriate hospital stay days (25.9%). The mortality rate was 13.5%. Having low proteins values in the CSF (odds ratio=0.095) was associated with lower mortality compared to patients with normal protein values.
Conclusion: This study shows a high percentage of inappropriate treatment in Lebanese hospitals despite these hospitals having adopted international treatment guidelines. This inappropriate management was associated with an increasing rate of mortality and neurological complications.
Meningitis is an inflammation of the meninges that presents as fever, headache, and nuchal rigidity.1 It is a serious illness for which emergency treatment should be implemented, to avoid a mammoth span of systemic and neurological sequelae.2 Knowing that meningitis is a preventable disease, vaccination and chemoprophylaxis guidelines have been prepared and their use has ensued a notable reduction in meningitis prevalence in the United States of America.3 Despite the progress and development of therapeutic treatment guidelines, early identification, and emergence of vaccinations and chemoprophylaxis, meningitis is still posing a weighty medical challenge due to the devastating mortality and morbidity rate associated with it.4 In fact, studies have revealed that individuals at least 16 years of age demonstrated a case fatality rate of 27% with persistent neurologic deficits present in 9% of survivors.5 Based on the Lebanese epidemiological surveillance unit at the Ministry of Public Health, the annual meningitis incidence increased from 1.5-4.6 per 100,000 inhabitants between 2000-2013, with the lowest incidence reported during the colder months of December and January, and highest during the hotter months of June and July.6 Although these reports have demonstrated a remarkable increase in the prevalence of meningitis over the last 13 years, they lack details about treatment, complications developed, or patients’ risk factors. The Infectious Disease Society of America guidelines, developed in 2004, state that meningitis treatment is divided into 2 parts: the first is the empiric therapy given after taking CSF through a lumbar puncture, and the second is microorganism-oriented therapy, after the identification of the causative pathogen.7 According to the Infectious Disease Society of America guidelines, age was classified into 3 categories: 0-1 month, 1.1 months-50 years and >50 years old. An increased risk of negative and positive bacterial infections is seen in patients aged one month to 50 years old. This would necessitate a treatment with vancomycin and a third-generation cephalosporin (ceftriaxone or cefotaxime). People over the age of 50 are at risk of infection from aerobic gram-negative bacilli that require therapy with vancomycin plus ampicillin and a third-generation cephalosporin. As for the dose, it was considered appropriate if it was consistent with the recommended doses in the IDSA guidelines. According to IDSA guidelines, each pathogen recommends a specific duration of therapy. The route of administration was considered compatible if the antibiotics were given intravenously or intraventricularly to reach the CSF. Medication adherence is defined by the World Health Organization (WHO) as “the degree to which the person’s behavior corresponds with the agreed recommendations from a health care provider”.8 Thigpen et al,9 conducted a surveillance study in the United States of America, and concluded also that the prevalence of bacterial meningitis had been reduced dramatically since the introduction of the Pneumococcal conjugate vaccine and the Haemophilus influenzae type b vaccine. Because meningitis cases can deteriorate in a short period, immediate treatment should be implemented, after a lumbar puncture. Empiric treatment based on patient’s age group and predisposing factors is administered until culture results are obtained, then therapy is adjusted according to the antibiogram sensitivity results. The primary scope of this study is to assess the clinical management of meningitis in Lebanese hospitals.
This study was performed with a primary objective of assessing meningitis treatment compatibility with the IDSA guidelines, due to the absence of national Lebanese guidelines. Secondary objectives aimed at assessing the correlations between treatment inappropriateness, patient characteristics, and the morbidity and mortality rate and to assess the correlation between inappropriate treatment, patient characteristics, and the morbidity and mortality rate.
Methods
This study was a retrospective descriptive study, conducted in 5 Lebanese hospitals, from January 2008 to December 2016. All patients admitted to these hospitals during the study period with a definitive diagnosis of the meningitis infection were screened for possible involvement in the study. Patients were included in the study if they had a lumbar puncture (LP) performed within 24 hours of hospital presentation, and the indication for the LP was documented in the medical record as being to evaluate for suspected acute bacterial meningitis. A minimum sample size of 114 patients was targeted to allow for adequate power for bivariable analyses to be carried out according to the Epi Info sample size calculations with a population size of 4 million in Lebanon, a 0.6% expected frequency of overall IDSA compliance, a 2% acceptable margin of error, and a 5% confidence limit.10 A total of 254 patients were initially screened; 2 immunocompromised patients were excluded. Of the remaining 252 patients, 47 were diagnosed with bacterial and 205 with viral meningitis.
The study protocol was approved by the institutional review boards of the involved hospitals and that of the Lebanese international university. No written informed consent was obtained, as this was a retrospective study. Data was stripped of any personal identifying information for confidentiality.
A pre-prepared data collection sheet was used to collect data from the hospital’s medical records. The data collection sheet was aimed at collecting socio-demographic information about the patients, as well as information on past vaccinations, medical history, empirical treatment, culture and gram stain based treatment, hospital stay duration, and treatment outcomes. This questionnaire assessed socio-demographic characteristics, including age, gender, region, number of rooms and the number of persons living in the house, and the level of education of both parents. Active smoking was determined by several questions (namely, number of daily cigarettes, weekly waterpipes smoked, other nicotine/tobacco use), categorizing subjects as non-smokers or current smokers. Questions about smoking or alcohol intake, the kind of alcohol along with the quantity, were included. Diagnosis was based on physical examination and laboratory tests; CSF and blood cultures were the main diagnostic tools. It is of note that only a few patients had undergone a computed tomography (CT) scan. Vaccination history was recorded based on the patient’s chart and the physician’s notes, to emphasize the critical role of vaccines on the meningitis incidence rate. The administered antibiotic treatment (empiric or culture based) in terms of drug, dose, duration of therapy, and route of administration were assessed for appropriateness and compatibility with the guidelines. Complications were recognized if the patient experienced any neurological or systemic problem. Neurological sequelae were evidenced by seizure or motor deficit, whereas systemic sequelae were evidenced by septic shock or respiratory failure. Mortality rate was also studied to evaluate the relationship between medication errors and death.
The primary outcome was to determine the extent of adherence of physicians to international guidelines for meningitis management, determining the appropriate antibiotic prescriptions based on drug selection, dosing, or both.7 The choice of drug depends on the age and on the most common predisposing pathogens.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Science (SPSS) version 22 (IBM Corp., Armonk, NY, USA). Descriptive analysis was presented as percentages for categorical variables or as mean and standard deviation for continuous variables. The Chi-square test was used to compare the percentages of 2 groups, whereas the Student t-test was used to compare the means of 2 groups. A logistic regression, using the enter method, was conducted, taking mortality as the dependent variable and all variables that showed a p<0.2 in the bivariate analysis as independent variables. The threshold of statistical significance was set at p<0.05.
Results
The socio-demographic characteristics of our sample are summarized in Table 1. No significant difference was detected between patients who had bacterial versus viral meningitis with regard to their socio-demographic characteristics, vaccination history, or predisposing risk factors (p>0.05 for all variables). Patients aged between 2-50 years old were the most common age group, at 50% for bacterial and 53% for viral meningitis. From the enrolled patients, 26 of the bacterial meningitis and 32 of the viral meningitis patients had comorbidities. Overall 78.2% of the CSF analysis and 71.8% of the blood analysis resulted in a negative culture. Confirmed meningitis cases were made up of 58 CSF culture positive bacteria and 39 blood culture positive bacteria. The most prevalent bacteria was Streptococcus pneumonia (12% for CSF and 6% for blood culture). Concerning the area of residence, there were more cases in urban areas (66.4%) than in rural areas (33.2%). From the collected vaccination history, 47.9% of patients had not had the required meningitis vaccines. It is noteworthy that 34 (13.5%) patients died during the study period.
Baseline characteristics of patients with bacterial and viral meningitis.
Assessment of viral meningitis treatment
Of the total of 205 viral meningitis diagnosed patients, 128 (64.2%) remained on the initial prescribed antibiotics despite the negative culture results, which is incompatible with the guidelines.
Evaluation of meningitis treatment compatibility with guidelines
The percentages of treatments and imaging conformities according to the guidelines are summarized in Figure 1. Adherence to guidelines for meningitis treatment showed that overall 89.7% of the patients were given treatment considered incompatible with IDSA recommendations.

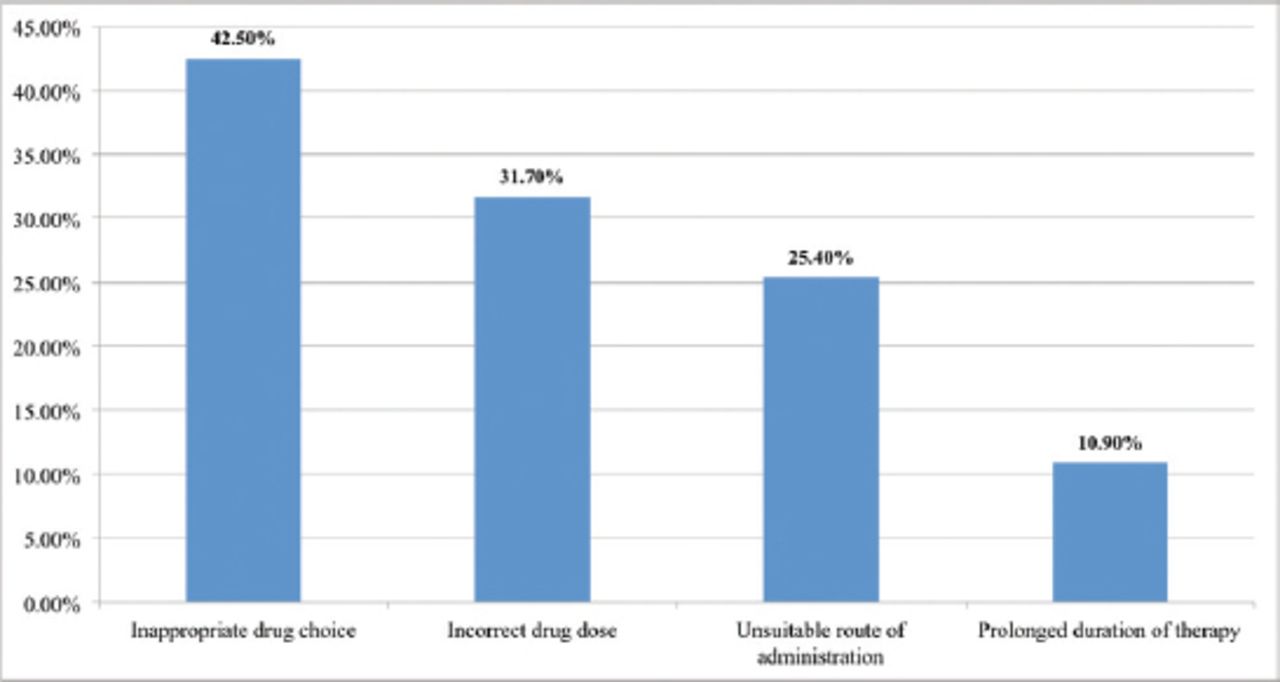
Treatment incompatibility with the Infectious diseases society of America (IDSA) guideline, in terms of drug of choice, dose, route of administration and duration of treatment.
Assessment of bacterial meningitis
Of the 112 subjects with diagnosed bacterial meningitis, 77 (68.7%) patients’ treatment regimens were incompatible with the IDSA guidelines. The incompatibility was due to drug choice (42.5%), dose (31.7%), the route of administration (25.4%), or the duration of therapy (10.9%) as illustrated in Figure 1. Meanwhile, in the definitive therapy (therapy administered after culture and sensitivity results were obtained, organism-oriented therapy), 49.1% of patients received an inappropriate definitive drug, 39.3% received an inappropriate dose, and 17% of patients received parenteral therapy for the whole hospital stay period. In 42.9% of cases, treatment duration was adjusted inappropriately according to the causative agent and the patient response. Finally, in 25.9% of cases, hospital stay days were incompatible and inappropriate.
Evaluation of meningitis complications
Sixty patients (29.26%) with viral meningitis developed complications at discharge, compared to 19 patients (40.42%) with bacterial meningitis. The most commonly encountered complication in both types of meningitis was seizure (100%). Seizures occurred in 51% of the elderly group’s patients (>50 years), 30% of the pediatric group patients (<1 month and 1 month-2 years), and 19% of patients in the group aged 2-50 years. The bivariate analysis of factors associated with neurological complications showed that a significantly higher percentage of patients living in an urban area (77.5%) had contracted meningitis compared to those who did not live in urban regions (62.7%; p=0.02). No significant difference was found for gender, smoking, alcohol consumption, allergy to drugs, and vaccination history.
Bivariate analysis
The bivariate analysis of factors associated with mortality showed that a higher number of patients who died were smokers (35.3% vs. 15.2%; p=0.005). A significantly higher percentage of patients who died had a marked increase of protein levels in the CSF compared to those who survived (41.4% vs. 28.4%). No other significant differences were found with all variables and mortality. There was no significant association between mortality rate and different age groups (p=0.47) and the causative microorganism (p=0.287) (Table 2).
Bivariate analysis of factors associated with mortality.
Multivariable analysis
A logistic regression, taking mortality as the dependent variable, showed that having low proteins values in the CSF (adjusted odds ratio=0.095; confidence interval [CI:0.01-0.905]) was associated with lower mortality compared to patients with normal protein values (Table 3).
Multivariable analysis. Logistic regression taking mortality as the dependent variable.
Discussion
This study was conducted knowing that no prior studies assessing meningitis treatment, prevention or prognosis were conducted in Lebanon. The results of this study showed that meningitis can affect all age groups, but in this study the highest attack rate was observed in patients aged 2-50 years (51.8%). Sixty percent of the meningitis cases were viral and 40% bacterial. The most commonly encountered bacteria in CSF and blood was Streptococcus pneumonia, which is consistent with reports by the Ministry of Public Health,11 but in opposition to the study of Jarousha et al,12 which found that Neisseria meningitidis was the most prevalent pathogen. The increase in the incidences of viral meningitis, accompanied with a significant decrease in the bacterial, is best explained by the emergence of vaccines and their introduction in the routine immunization schedule. The statistical results revealed that a high percentage overall of inappropriate treatment (89.7%), a higher percentage than the one found by Sheley et al,13 (47.4%) with a lower mortality as well. Starting with bacterial meningitis, the results showed that 68.7% of patients received treatment not recommended by the guidelines. The most common reason behind this incompatibility was the wrong definitive antibiotic given after culture results. In case of viral meningitis, most physicians kept using antibiotics even after culture results (76.2%), despite the recommendation of Logan et al,14 which notes that viral meningitis is a self-limiting infection and needs only supportive treatment, acyclovir if severe. Neurological complications, mostly seizures, at discharge occurred in 40.2% of bacterial and 35.7% of viral meningitis patients. This percentage is higher than that reported by Ciofi et al,15 who assessed complications after hospital discharge in Italy. Risk factors found to be associated with poor prognosis were old age, and inappropriate treatment. The mortality rate increases linearly with increasing age, being highest in elderly patients (51.7%), in contrast to the results of Strelow et al,16 which concluded that age and mortality were independent, but consistent with those of Choi.17
Based on these results, physicians should stay up-to-date through continuous education sessions and their own readings in order to follow the most updated guidelines for meningitis treatment. Also, conjugate vaccines for haemophilus influenzae type B and S. pneumoniae should be initiated in early childhood, the effect of which have been highly effective in reducing the incidence of bacterial meningitis, not only in children but also in adults.
Study limitations
It is a retrospective study in which it is impossible to control exposure or outcome assessment. Selection bias might have occurred, depending on the accuracy of medical records. Long-term follow-ups was not possible after discharge because patients were not accessible, so rate of neurological complication, especially cognitive impairment, was underestimated. Since meningitis is a rare condition and Lebanese hospitals preserve their medical records for maximum of 5 years, the sample size was small. There was no unified documentation in patient information among the different medical centers. Other risk factors involved in meningitis such as poverty, high population density, or travelling to the meningitis belt regions, could not be assessed because of limited data.
In conclusion, inappropriate meningitis treatment was associated with a significant morbidity and mortality rate. Future awareness campaigns highlighting the vital role of the clinical pharmacist in adjusting and individualizing meningitis treatment, and an assessment of adherence to guidelines, should be implemented. Also, the role of vaccinations and chemoprophylaxis should be addressed.
Acknowledgment
The authors gratefully acknowledge Dr. Mohamad Iskandarani for his help in the statistical analysis and Miss Susan Wilson for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company
- Received October 4, 2018.
- Accepted January 28, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.