


Abstract
Objectives: To determine the incidence of surgical site infection (SSI) after trauma laparotomy and evaluate variables on presentation to the emergency department (ED) associated with the development of SSI.
Methods: A retrospective cohort study was undertaken of patients presenting directly from the scene who underwent trauma laparotomy between January 2016 and December 2017. The primary outcome variable was SSI, as defined by the Centers for Disease Control and Prevention guideline. A univariate assessment with demographics, vital signs, and acute management was reported.
Results: A total of 70 patients were included for data analysis. Of these, 9 (12.9%; 95% confidence interval (CI): 6.9-22.7%) patients developed SSI, including 5 patients with bowel injury (small bowel; n=3, colonic injuries; n=2). Most cases were diagnosed after 7 days in the hospital. All patients developed superficial incisional (skin and subcutaneous tissue) SSI. No predetermined variables, including bowel injury (p=0.08) or duration of surgery (p=0.09), demonstrated a statistically significant association with the development of SSI.
Conclusion: Rates of SSI after trauma laparotomy were similar to previous reports from other centers. Surgical site infection after trauma laparotomy was diagnosed at a delayed time point after surgery, and patient demographics, injury characteristics, and acute surgical management did not appear to be associated with subsequent diagnosis of SSI.
Physical injury or trauma is predicted to become the third largest contributor to the global burden of disease by 2020. Worldwide, more than 5 million people die as a result of trauma each year, with trauma as the leading cause of death for young adults.1 Trauma represents 10% of the world’s deaths more than the deaths from malaria, tuberculosis, and HIV/AIDS combined.2,3 This global disease burden affects productive members of society, often leading to long-term disability and dependency among long-term survivors. Abdominal injury occurs in 15% of major trauma cases, and exploratory laparotomy is performed in 25%.4 While surgical site infection (SSI) after laparotomy is a growing global concern, reports on incidence, outcomes, and associated variables are limited. A single Colombian study of 614 patients reported that 13.8% of patients undergoing trauma laparotomy developed SSI.5 Other studies have reported that SSIs represent 38% of nosocomial infection in surgical patients.6 The burden of trauma in the Kingdom of Saudi Arabia is substantial. Between 1971-1997, 564,762 people died or were injured in road traffic accidents alone.7 Many facets of pre-hospital and in-hospital trauma care are being addressed to improve patients’ outcomes and reduce this burden. This study aimed to determine the incidence of SSI after laparotomy among trauma patients that presented to King Saud Medical City, Riyadh, Kingdom of Saudi Arabia (KSA) and to determine if preselected emergency department variables were associated with the development of SSI.
Methods
King Saud Medical City is a tertiary care center with 1,400 inpatient beds. A dedicated trauma unit manages all polytrauma patients, with a trauma surgeon operating on all penetrating and blunt chest, abdomen, and neck trauma when indicated. In 2017, a total of 29,671 trauma patients presented to King Saud Medical City emergency department, of which 3,459 patients were admitted.
A retrospective cohort study of patients presenting directly from the scene who underwent trauma laparotomy was undertaken. All cases of trauma laparotomy performed between January 2016 and December 2017 were included in this study. Cases transferred from other hospitals and underwent relook laparotomy were excluded. All data were extracted by a single investigator using explicit chart review and were verified by a second investigator, using the chart review methodology described by Gilbert et al.8
Data related to demographics, injury details, management, and outcomes of SSI and mortality at hospital discharge were extracted from medical records. King Saud Medical City operative triage had been defined as E1 (immediate life or limb-saving surgical intervention), and E2 (potential life or limb-saving surgical intervention within 6 hours). All physiological parameters were evaluated at the time of admission (on arrival). Afterhours was defined as the patient being operated upon by the on-call team (18:00-07:00). The day of the week when surgery was conducted, it was reported due to the previously reported association of adverse events after elective surgery.9 All patients received cefuroxime and metronidazole as prophylactic preoperative broad-spectrum antibiotics.
Our primary outcome was the presence of abdominal SSI. The definition of SSI was based on the Centers for Disease Control and Prevention guideline.10 A positive SSI was defined as the presence of symptoms and signs of infection, such as fever, localized pain or tenderness, redness, swelling, purulent discharge, and presence of the organism in an aseptically obtained culture within 30 days after laparotomy. Surgical site infection was sub-grouped as superficial incisional (skin and subcutaneous tissue), deep incisional (fascia and muscle), and organ/space (intra-abdominal) SSI.
Statistical analysis
Categorical variables were assessed using frequency tables. Numerical variables were evaluated with summary statistics (for continuous variables, mean and standard deviation; for ordinal variables or skewed distribution of variables, median and interquartile range). Differences were assessed by using Student’s t-test for continuous variables and Fisher’s exact test or the Chi-square test for difference between proportions. A p-value of <0.05 was considered statistically significant. All analyses were conducted using Stata v 11.3 (College Station, Texas, USA).
The study was approved by the King Saud Medical City Institutional Review Board (IRB ref: H1R1-08-Nov 17-02). The IRB committee approved a waiver of the requirement to seek informed consent from participants for retrospective review of their data.
Results
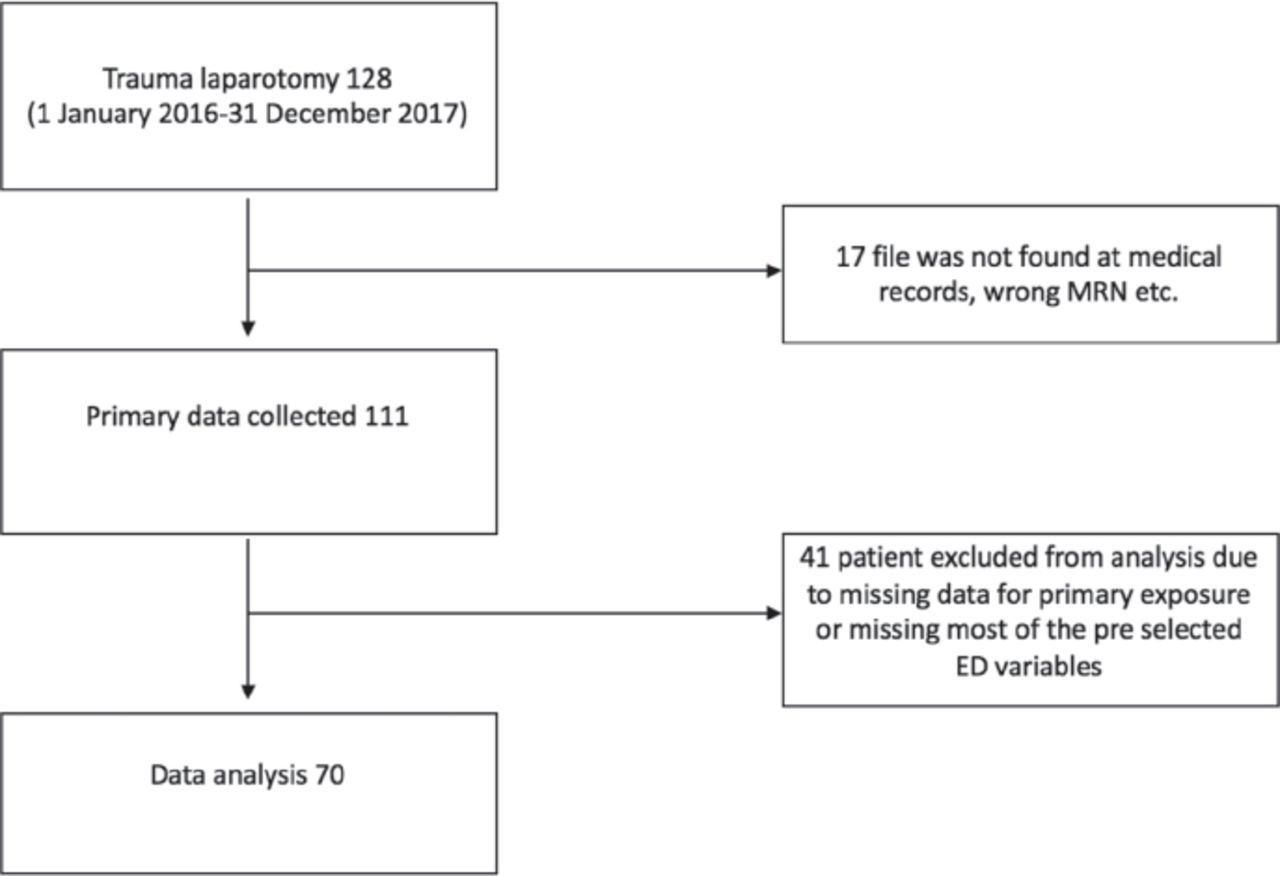
Over a 24-month period, 128 eligible trauma laparotomy patients were identified from the operation log. Of these, 17 medical records could not be located. Data was extracted from the remaining 111 patient files. In 41 cases, following chart review, the presence or absence of SSI could not be determined, or a large number of preselected exposure variables were missing. The remaining 70 patient records were included for data analysis (Figure 1).
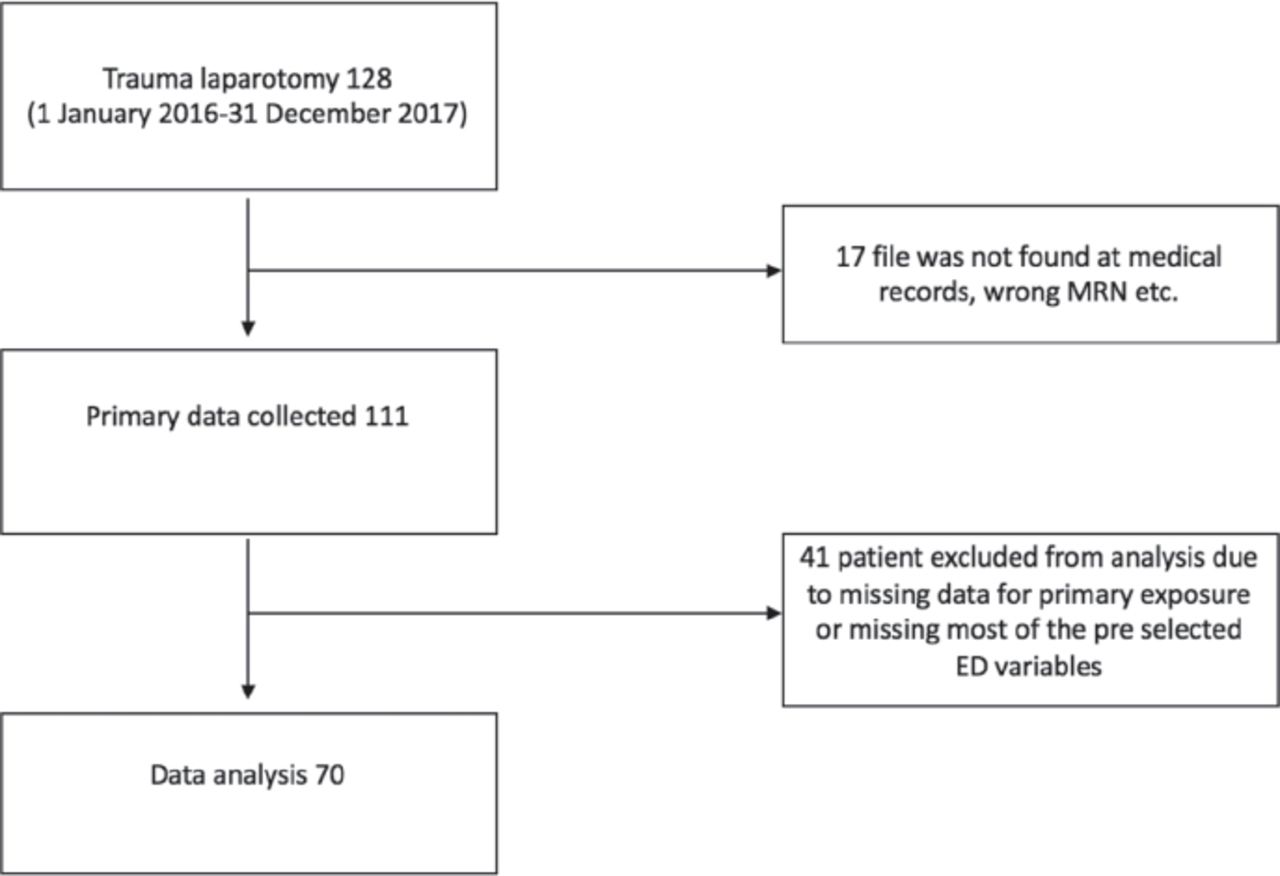
Sample selection.
Of patients included in this study, 64 (91.4%) were male, with a mean age of 30.8±13.2 years. The majority of the cases (67.2%) were due to blunt trauma (motor vehicle crash [60%]). Most trauma laparotomies occurred on Tuesday (28.5%). The mean time from emergency department to operating room was 325.1±285.6 min. Almost half (51.4%) of the laparotomies were performed after hours. The mean operating time was 130.2±67.9 min. One patient had been diagnosed with diabetes mellitus, and one patient was extremely obese (body mass index [BMI]>50). No other comorbidities were identified. The mean stay days in the intensive care unit (ICU) was 8 days and hospital stays was 20 days (Table 1).
Demographics, injury details and management (N=70).
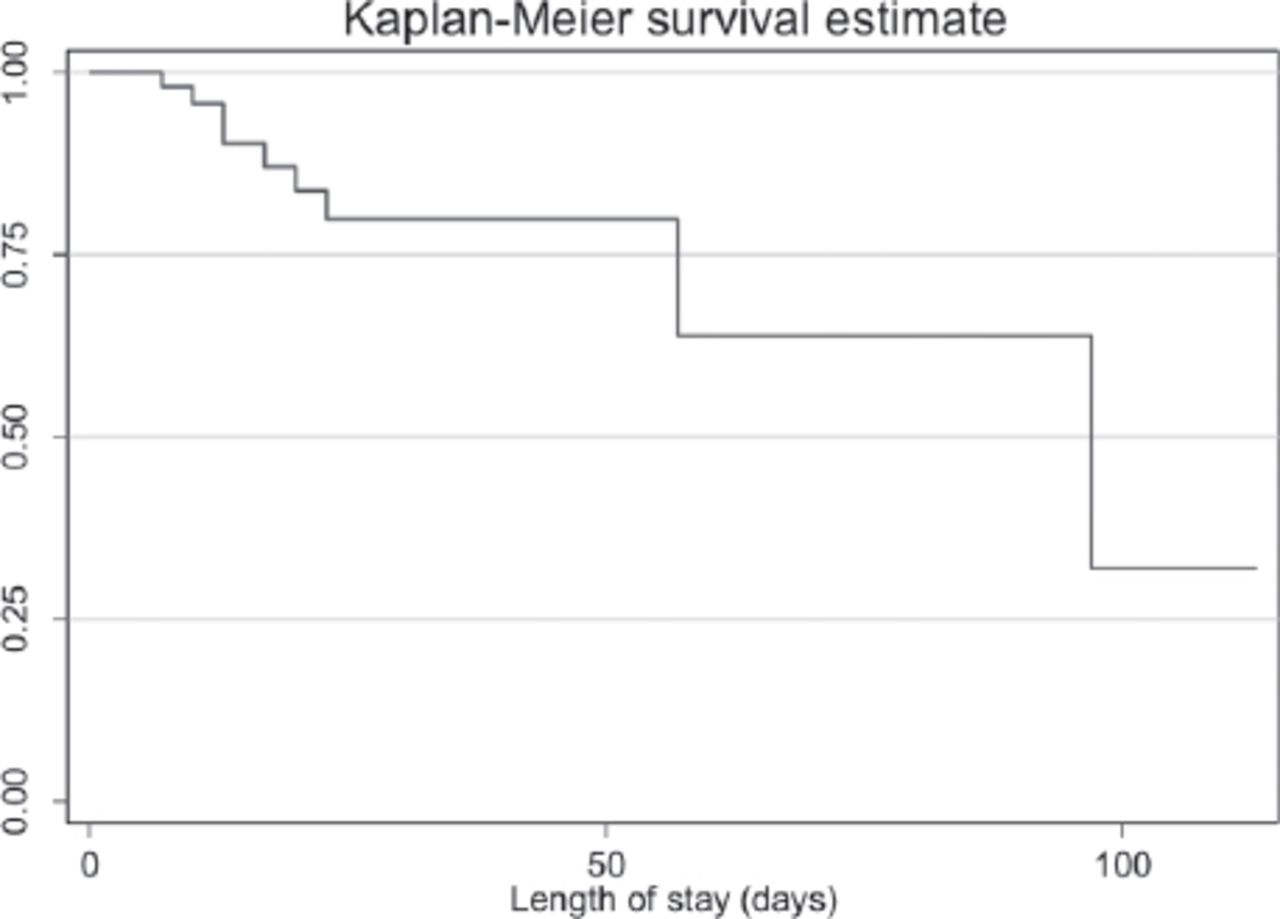
Nine (12.9%; 95% CI: 6.9-22.7) patients developed SSI. Of these, 5 patients had bowel injury (small bowel; n=3, colonic injury; n=2). The most common organisms were Escherichia coli (n=4), followed by Enterobacter cloacae (n=2), Pseudomonas aeruginosa (n=1), and Klebsiella pneumoniae (n=1). One patient had polymicrobial growth. All of these patients developed superficial incisional (skin and subcutaneous tissue) SSI. Figure 2 illustrates the time at which SSIs occurred, with most cases diagnosed after 7 days in the hospital.
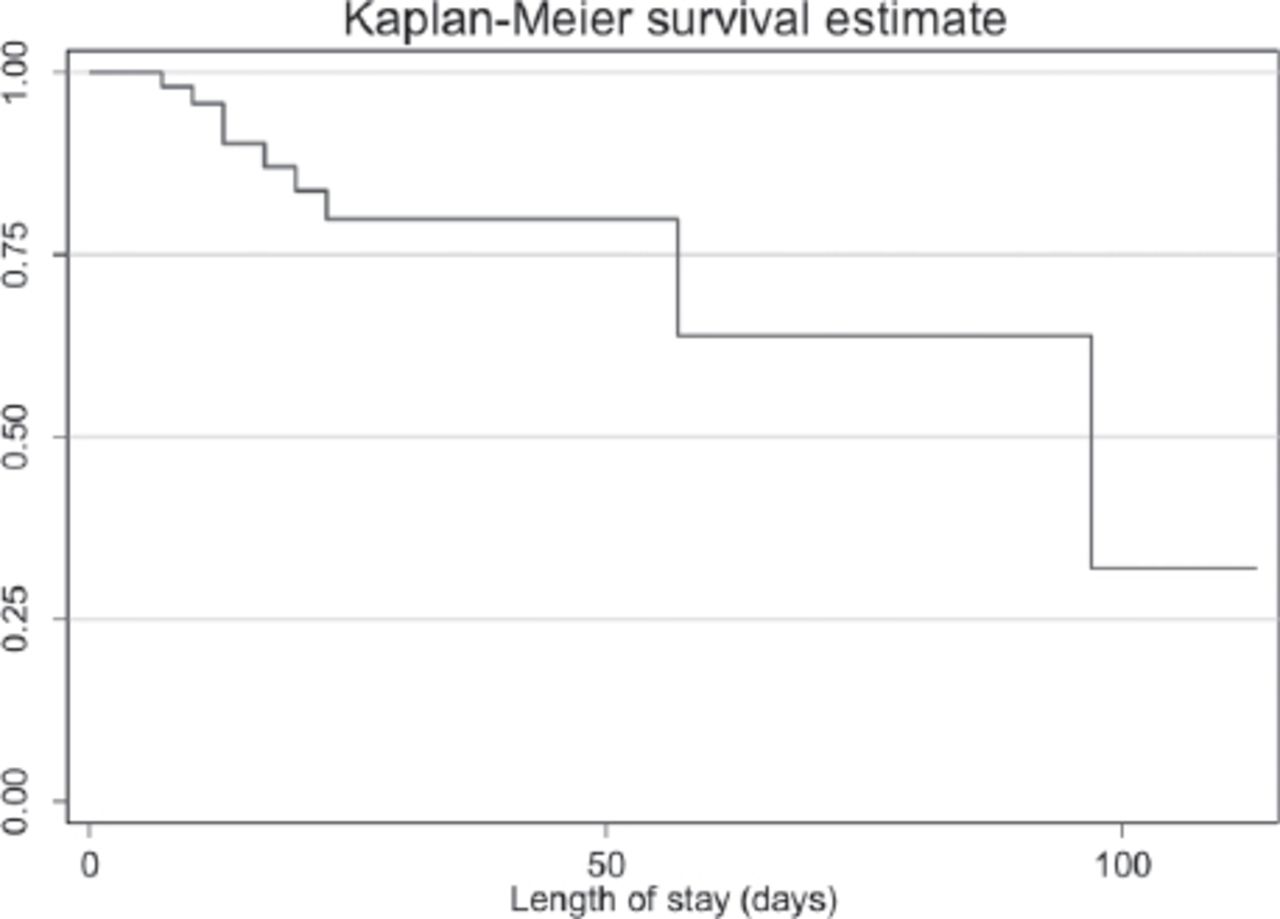
Surgical site infection over time.
No predetermined variables, including bowel injury (p=0.08) and duration of surgery (p=0.09), demonstrated a significant association with SSI (Table 2).
Univariable association of variables with SSI.
Discussion
This study demonstrated that at least one in 8 patients developed SSI after trauma laparotomies in this single large trauma center in KSA. Demographics, injury severity, and times to operative management were not associated with subsequent development of SSI. Causative factors remain undetermined and require further evaluation of surgical technique and post-surgical management.
There is a paucity of data for SSI rates after trauma laparotomy, with no agreed benchmarks for trauma centers. The study’s SSI rate of 12.9% appears acceptable relative to a previously published estimate of 13.8%.5 As this institute embarks upon a system-wide program to improve trauma care, it provides a baseline for further improved care.
Trauma from motor vehicle crashes is an increasing concern in Kingdom of Saudi Arabia, representing the second most common cause of death in all age groups.11 King Saud Medical City in Riyadh, Kingdom of Saudi Arabia is a major trauma hospital in the region and SSI is considered a common postoperative complication. Surgical site infection represents the most frequent adverse postoperative event in health care and is one of the most frequent types of hospital-acquired infection (HAI).12 Although the rate of SSI is higher in developing countries, reports from these countries are limited.12
Non-operative management is the prevailing standard of care for hemodynamically stable patients. However, for those requiring laparotomy, the delay of operative intervention is associated with postoperative complications.13 There is a scant information in the literature on the incidence of SSI after trauma laparotomy or the effects of hollow viscus injury, the duration of surgery, or the type of injury. Our cohort study suggests that a more detailed analysis of surgical technique and postoperative management in the ICU is required to understand the determinants of SSI and to develop management protocols to prevent SSIs.
Study limitations
This is a retrospective cohort, with data solely dependent on what was documented in the patients’ files. Accuracy was difficult to verify. A large number of patient records had missing data; therefore, the affected cases were deleted from the analysis. Some demographic patient details were also lacking, and we were unable to determine the causes of delay to the operating theater. Only univariate analyses are presented since the multivariable analysis was not possible without any statistically significant associations. The sample size was small but provides baseline data for evaluating outcomes and measuring improvements after trauma laparotomy. Prospective analysis, aided by the newly launched trauma registry, will be used to further evaluate SSI and its association with other outcome measures, such as patient satisfaction and correlation with other healthcare-associated infections.
In conclusion, demographic and injury characteristics were not associated with an increased risk of SSI after trauma laparotomy. Potential clinically significant variables, such as bowel injury, time to the theater, and operating time require further evaluation in prospective studies. In this series, all SSI after trauma laparotomy were diagnosed after 7 days in the hospital.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 26, 2018.
- Accepted February 8, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.