


Abstract
Objectives: To evaluate whether using laryngeal mask airway (LMA) made a difference in terms of airway security, hemodynamic changes, complications, and recovery times compared to tracheal intubation during the procedure in patients undergoing general anesthesia for endovascular treatments of unruptured cerebrovascular aneurysms.
Methods: The electronic medical records database, patient files, and anesthesia charts were examined between May 2008 and September 2016 to identify patients with the following inclusion criteria: 1) aged 18-70 years; 2) American Society of Anesthesiologists (ASA) classification I-III; 3) diagnosis of unruptured CVA; 4) Glasgow coma scale of 15 without neurological deficit; and 5) underwent elective EVT under general anesthesia.
Results: Tracheal tube (TT) was used in 46 patients (group TT, n=46) and LMA in 42 patients (group LMA, n=42). Mean arterial pressure (MAP) levels were increased to >20% of baseline in 14 patients (30.4%) after intubation and in 6 (13%) after extubation in group TT. All LMA patients remained within normal MAP limits (p<0.05). Six patients (13%) displayed coughing or straining at extubation in group TT whereas none in group LMA (p<0.05). Recovery and discharge times were similar (p>0.05).
Conclusion: Laryngeal mask airway and TT provided comparable airway security during procedure. Laryngeal mask airway attenuated stress response in hemodynamic parameters at intubation and extubation and smoother emergence compared to TT without delay in recovery.
Endovascular treatment (EVT) for cerebrovascular aneursyms (CVAs) became one of the primary therapeutic options after the introduction of detachable coils, because this technique is reported to be minimal invasive and similar efficient with lower complication rates compared to open surgery with surgical clipping.1
Anesthetic management for EVT shares many principles with neurosurgical anesthesia including hemodynamic stability, immobilization of patient, control of arterial blood pressure (ABP) and early recovery to diagnose neurological deficits.2-4 General anesthesia (GA) is still the most preferred technique because it fulfills the requirements of the procedure with ensuring airway safety.5,6 It has been also proposed to use tracheal intubation for GA as in neurosurgery.4,6,7 Supraglottic airway devices are recently introduced in EVT settings, but the availability of their routine use is currently not clear. Only 3 reports have addressed the use of supraglottic airway devices in an EVT setting in the past 10 years.8-10 In the interventional neuroradiology unit of the hospital, we have been using both laryngeal mask airway (LMA) and tracheal tube (TT) for airway management in EVTs under GA for nearly 8 years. In this retrospective study, we aimed to evaluate whether using LMA made a difference in terms of airway security, hemodynamic changes, complications, and recovery times; compared to tracheal intubation during the procedure in patients undergoing GA for EVTs of unruptured CVA.
Primary outcome was to compare the effect of airway management using LMA or TT on hemodynamic parameters. Secondary outcomes were to compare adverse respiratory events related to the airway technique, recovery and discharge times, including time to extubation, time to neurological assessment, and time to discharge.
Methods
This retrospective study was approved by the hospital’s ethics committee (protocol 042010/1780) and registered with the Australian New Zealand Clinical Trials Registry (ACTRN12618000509268). It was carried out at radiology units in 29 Mayıs and Çankaya Hospitals, Turkey.
The electronic medical records database, patient files, and anesthesia charts were examined between May 2008 and September 2016 to identify patients with the following inclusion criteria: 1) aged 18-70 years; 2) American Society of Anesthesiologists (ASA) classification I-III; 3) diagnosis of unruptured CVA; 4) Glasgow coma scale of 15 without neurological deficit; and 5) underwent elective EVT under general anesthesia.
The patients with accompanying cerebrovascular disease including arteriovenous malformation, stenosis, and so forth, history of surgical treatment for cerebrovascular disease, history of difficult ventilation and intubation, and failed airway management after the induction of GA were excluded from the study.
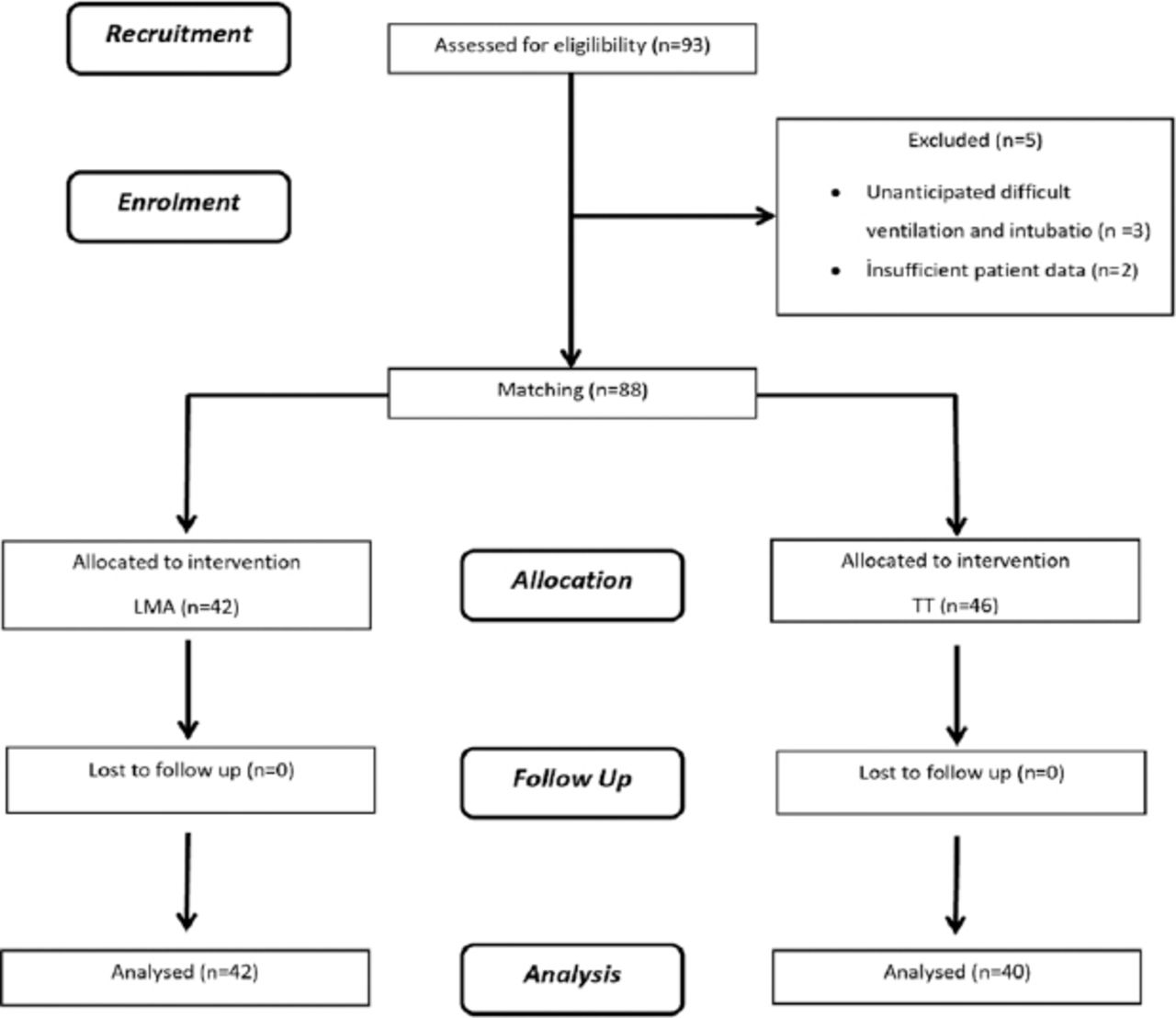
All pre-anesthesia documents and intraoperative anesthesia charts were reviewed by study members in detail to obtain: 1) demographic characteristics; 2) type of anesthesia used for induction and maintenance; 3) choice of airway management technique (TT or LMA); 4) vital parameters - before induction (baseline), before (pre-intubation), after tracheal intubation or LMA insertion (post-intubation), and after extubation or removal of the LMA (post-extubation); 5) recovery and discharge times (time to extubation or to removal of the LMA, time to neurological assessment, and time to discharge from the INR unit to the intensive care unit [ICU]); and 6) complications and adverse events related to EVT and anesthesia. All data were collected and 2 groups were identified according to the type of airway management for GA that was performed: group LMA and group TT (Figure 1).

Study flow diagram of 88 patients.
The same anesthetic protocol is used for the patients undergoing EVTs under GA. All patients were monitored according to standards for basic anesthetic monitoring of ASA in the interventional neuroradiology unit. In addition, an arterial catheter was inserted in the left radial artery after local anesthetic infiltration to monitor intra-arterial bood pressure. Baseline vital parameters were measured and recorded.
General anesthesia was induced with intravenous propofol and fentanyl. A cuffed TT (internal diameter 7.0-8.5 mm) was placed using direct laryngoscopy and orotracheal intubation or a correctly sized LMA (no. 3-5) was inserted for airway securing. A neuromuscular blocking agent, rocuronium 0.6 mg kg-1 was given to facilitate orotracheal intubation in patients whose airway management was achieved with TT. Maintenance of GA was achieved by using remifentanil and propofol based total intravenous anesthesia. Infusion doses were adjusted to keep the mean arterial pressure (MAP) between 50 and 60 mmHg. All drugs and interventions were used in the same manner for all patients including ventilatory settings, activated clotting time (ACT) measurements, heparinization to a target ACT levels, renal protection to prevent contrast- induced nephropathy, gastric protection, bladder catheterization for urine output measurement, and warming of patients to prevent hypothermia.
A single neuroradiologist performed all interventions. Digital subtraction angiography was performed to visualize the 3-dimensional structure of the aneurysm after femoral artery catheterization. Multiple Guglielmi detachable coils were deployed through a microcatheter into the aneurysm until sufficient occlusion was achieved. After completion of the EVT, anesthesia was discontinued and airway instruments were removed after achieving extubation criteria. Neostigmine, an anticholinesterase agent, was given to patients who were intubated to reverse the effect of the neuromuscular blocking agent (rocuronium) to facilitate orotracheal intubation.
Clinical outcome was assessed with the Glasgow outcome scale (GOS). Criteria for transfer to the intensive care unit were stable neurological and cardiovascular status, a modified Aldrete recovery score >9, and a dry femoral artery puncture site.
Anesthetic protocol, MAP levels, peripheral oxygen saturation (SpO2), end-tidal CO2 levels and heart rate were monitored and recorded before and after induction of anesthesia, of airway management, of removal of airway instruments and also with 5 min intervals throughout the procedure. Bolus doses of metoprolol (40 µg kg-1), a selective ß1- blocking agent, were given when the MAP increased >20% above baseline values to avoid further increase in blood pressure. Also, respiratory adverse events including laryngospasm, coughing, and straining, time to extubation, time to neurological assessment (with GOS) and time to discharge (using modified the Modified Aldrete Recovery Scoring Sytem) were recorded in all patients.
Statistical analysis
Data were analyzed using the Statistical Packages for Social Sciences for Windows version 11.5 pocket program (IBM Corp., Chicago, IL, USA). For intergroup comparisons, the Chi-square test and Fisher’s exact test were used to analyze nominal data and the t-test for independent samples was used for quantitative data. Data were expressed as means ± SD for continuous variables and numbers, and percentages for categorical variables. The value of p<0.05 was considered significant.
Results
A total of 93 anesthesia documents were reviewed, and 5 cases were excluded. Of those, unanticipated difficult ventilation and intubation occurred in 3 cases, in which EVT was cancelled and the patients were awakened without complication and referred to awake fiberoptic intubation. The other 2 cases had insufficient anesthetic data in their medical records. Finally, the data obtained from 88 cases were used for the analysis. TT was used in 46 patients (Group TT, n=46) and LMA in 42 patients (Group LMA, n=42). Patient characteristics and the duration of the procedures did not differ between groups (Table 1). All neuroradiological treatments were completed successfully without procedure-related complications.
Adverse respiratory events, recovery and discharge times of 88 patients.
After the induction of anesthesia, MAP levels were within ± 20% of the baseline levels in 30 TT patients (65.2%) and 37 LMA patients (88.1%) (p<0.05). In the remaining patients in both groups, MAP levels were reduced to >20% below baseline but did not reach >30%. Therefore, vasopressor drugs were not used to increase blood pressure after induction (Table 2). After securing the airway with the TT or LMA, postintubation MAP levels were >20% of the baseline level in 14 patients (30.4%) in the TT group and 0 patients in the LMA group (p<0.05) (Table 2). Those 14 TT patients received metoprolol.
Mean arterial pressure and heart rate at 3 periods of the procedure. (N=88)
Peripheral oxygen saturation, end-tidal CO2 levels, and peak airway pressures were within normal limits in both groups during the procedure. Recovery times were longer in the TT group than in the LMA group after completion of the procedure and anesthesia, but the difference was not statistically significant (p>0.05) (Table 3). No extubation event was observed in the LMA group, whereas coughing was observed in 3 patients and straining in another 3 in the TT group (p<0.05) (Table 3). Postextubation MAP levels were >20% of the baseline levels in 6 patients in the TT group (13%) and no patients in the LMA group (p<0.05) (Table 2). Further increases in the MAP levels were prevented by administering metoprolol. The postoperative GCS score was 15 in all patients, with no neurological impairment. Discharge times were similar in both groups (p>0.05) (Table 3).
Adverse respiratory events, recovery and discharge times.
Discussion
The results of this retrospective study demonstrated that the use of LMA decreased the incidence of hemodynamic changes during airway management and extubation, providing a smoother emergence from anesthesia without airway complications compared to TT. However, the recovery times for neurological evaluation were similar between LMA and TT.
In one of only 3 reports in the literature address this issue, Golshevsky and Cormack8 reported on the use of LMA during GA in 3 patients undergoing EVT for ICAs and concluded that LMA may be a safe alternative by avoiding the hemodynamic effects of tracheal intubation. In a non-randomized study, Karwacki et al9 evaluated the usefulness of GA with propofol and LMA for EVT of unruptured ICAs in 26 ASA I patients. They concluded that the use of LMA is the optimal method for securing the patency of the upper airways during anesthesia for endovascular ICA repair.9 The 3rd study, Tan et al10 reported no complications related to the use of LMA for GA in endovascular coil embolization.
In contrast to the surgical treatment of cerebral aneurysms, securing the airway with tracheal intubation may not be necessary for EVTs under GA in which the patient lies supine on the operating table and the positions of the head and body are not changed. Moreover, the procedure is shorter and painless and has minimal blood loss compared to intracranial surgery. In the present study, the mean duration of the EVT procedures was approximately 75 ± 20 min (range, 30-125 min). This result is consistent with previous studies that have reported a typical time frame of approximately 1.5 hours (range, 1-2 hours) for coiling an intracranial aneurysm.11
Studies have reported that LMA can be used safely without gastroesophageal insufflation when inserted properly and used with positive-pressure ventilation at volumes of less 10 mL kg-1, with ventilation pressuråes kept lower than 20 cm H2O during procedures that last longer than 120 min.12,13
The integrity of a cerebral aneurysm depends on the transmural pressure (TMP), which is determined by the difference between the pressure within the aneurysm (equivalent to the MAP) and the pressure surrounding the aneurysm (equivalent to the ICP).14 A rise in MAP increases the TMP and makes rupture of the aneurysm more likely, which is the most dangerous complication of the procedure, with a mortality rate of up to 50%.14,15 Thus, the prevention of exacerbated hemodynamic responses related to anesthetic management is essential.
Generally, hemodynamic fluctuations occur during the induction and emergence stages of GA.16,17 Laryngoscopy, tracheal intubation, or insertion of supraglottic airway devices, as well as laryngospasm, coughing, and straining caused by extubation, may stimulate pain and airway reflexes, resulting in ABP and ICP elevations. This hemodynamic response is associated with cerebral hemorrhage with an incidence of one percent during surgical clipping.18 Studies comparing LMA with TT during induction and extubation have indicated that the cardiovascular responses induced by laryngoscopy and intubation may be more than twice as great as those induced by the insertion of an LMA.19,20
Rapid recovery is an important factor in assessing neurological status and the early diagnosis of post-procedural complications. In the present study, a total intravenous anesthesia technique with propofol and remifentanil was used to for the maintenance because these drugs reduce cerebral blood flow and ICP. They also provide stable hemodynamics and rapid recovery from GA.6,7,9 Recovery and discharge times in our study were similar between 2 groups.
One limitation of this study is that the anesthetic depth was not monitored during the procedure due to the unavailability of a bispectral index, which is also useful for detecting cerebral ischemia and intraventricular hemorrhage.21,22
Another limitation is the retrospective design of the study. Retrospective studies may suffer from selection and recall bias. Therefore, we used the same inclusion and exclusion criteria for both groups to minimize selection bias. Additionally, all patients received the same EVT and anesthetic regimens except for the airway management interventions. We also attempted to minimize recall bias by using multiple data sources including an electronic medical records database, patient files, and anesthesia charts.
In conclusion, LMA may be routinely used in patients undergoing EVTs under GA due to airway securing without respiratory complications. Hemodynamic stress responses at insertion and removal periods were attenuated and emergence was smoother compared to tracheal intubation. Further prospective and randomized studies are required to determine the availability of the routine use of supraglottic airway devices in interventional neuroradiology.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received January 13, 2019.
- Accepted March 19, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.




{kind=link}