


Abstract
Objectives: To determine the sensitivity and specificity of computed tomography (CT) and ultrasound (US) in predicting acute appendicitis in relation to histopathology reports at King Fahad Specialist Hospital in Buraidah, Saudi Arabia.
Methods: A retrospective cohort study included 500 medical records of patients diagnosed with acute appendicitis upon admission to King Fahad Specialist Hospital, Buraidah, Saudi Arabia, between January 2015 and January 2017.
Results: Of the 200 patients, 187 (93.5%) were diagnosed with acute appendicitis by histopathology. Of these 187 patients, 57 (30.5%) underwent CT and 54 (29%) underwent US. Computed tomography correctly identified 86.0% of the patients as having acute appendicitis and incorrectly identified 14% as not having acute appendicitis. Similarly, US correctly identified 37% of the patients as having acute appendicitis, while the remaining 63% were incorrectly identified as not having acute appendicitis. Thirteen patients (6.5%) did not have acute appendicitis (confirmed by histology report). Six (46.15%) of these 13 patients underwent CT. Five of these 6 (83.3%) were incorrectly diagnosed with acute appendicitis by CT, whereas one of the 6 (16.7%) was identified as a true negative. On the other hand, US correctly identified 100% of the 13 patients as true negative.
Conclusion: Computed tomography was shown to have sensitivity 86% and a specificity of 16.7% for the diagnosis of acute appendicitis. On the other hand, US had a sensitivity of 37% and a specificity of 100%. Therefore, we conclude that if imaging needed to confirm the diagnosis of appendicitis, CT is the choice. Ultrasound can be used only to exclude gynecological disorders.
Appendectomy for acute appendicitis is one of the most commonly performed types of emergency surgery. More than 300,000 appendectomies are performed annually in the United States of America.1 Acute appendicitis is considered a differential diagnosis for all patients who present with acute abdomen, which means the ability to differentiate it from other conditions is crucial. Historically, acute appendicitis has been diagnosed through patient history, physical examination, and laboratory tests. All of which contribute to the patient’s Alvarado score. However, detecting acute appendicitis remains challenging, because it does not have a typical presentation. A patient with a high Alvarado score should undergo surgery without additional investigation. On the other hand, if the Alvarado score is in the intermediate range, or if the diagnosis is otherwise questionable, ultrasound (US), computed tomography (CT), or magnetic resonance imaging (MRI) should be used. The diagnostic accuracy achieved by patient history and physical examination was approximately 80% in both men and women (men were diagnosed accurately 78% to 92% of the time, while women were diagnosed accurately 58% to 85% of the time).2 Because untreated acute appendicitis leads to perforation, which increases mortality and morbidity rates, the percentage of negative appendectomy is considered to be acceptable.3 A negative appendectomy is defined as the removal of a normal appendix from a patient operated on due to suspected appendicitis.4 Although appendectomy is generally well tolerated, it is a major surgical intervention that can be associated with postoperative morbidity.5,6 In recent years, radiological tests, beginning with the first report on compression US by Puylaert7 have emerged as useful tools to decrease the rate of negative appendectomies and to rule out other differential diagnoses. Computed tomography is considered the gold standard for evaluating patients with suspected acute appendicitis.3,8 Magnetic resonance imaging has also demonstrated a high rate of accuracy in the detection of acute appendicitis and is useful when radiation is not appropriate (example, cases of children and pregnant women).3,8
In this study, the reliability of CT and US for the detection of acute appendicitis at King Fahad Specialist Hospital, Buraidah, Saudi Arabia was assessed. The study aimed to establish the sensitivity and specificity of CT and US in predicting acute appendicitis and compared the abilities of radiological tests and histopathology reports to accurately diagnose acute appendicitis.
Methods
This study consisted of a retrospective chart review and analysis of medical records of patients diagnosed with acute appendicitis upon admission to King Fahad Specialist Hospital in Buraidah, Saudi Arabia.
All patient data were anonymized and no personal identifiers were used. None of the data in this study can be linked with the personal identity of the patients. The ethical approval was obtained from the Regional Research Ethics Committee, Ministry of Health, Qassim Province, Saudi Arabia before starting data collection.
Buraidah, the capital of the Al-Qassim region of Saudi Arabia, has 3 health institutions, the largest of which is King Fahad Specialist Hospital. The city has a typical desert climate and a population of almost 600,000.
All patients were admitted between January 2015 and January 2017 with a diagnosis of acute appendicitis, regardless of their gender, age, or surgical procedure. Inclusion criteria were: 1) patients admitted due to suspected appendicitis; 2) patients who underwent CT; and 3) patients with histopathological reports.
Exclusion criteria were: 1) patients with urological or gynecological diseases; 2) patients without a radiological investigation; 3) patients without a histopathology report; and 4) all medical records before January 2015 and after January 2017.
Two CT scanners have been used; GE 64 slices and Siemens dual energy 128 slices. The protocol was variable according to the patient status and tolerability to oral or intravenous contrast (IV). Most of the patients had gastrografin and IV contrast, while others had it with IV contrast only. Any patient had following CT findings; thick appendix more than 6 mm, mucosal enhancement, periappendiceal fat stranding, thickened cecum at the base of the appendix, or free fluid in the right iliac fossa or US findings; blind ended tubular structure in the right iliac fossa bigger than 6 mm with inflamed fat and free fluid considered positive for acute appendicitis.
Data were retrospectively collected from the medical records of 500 patients who met the study criteria. After the inclusion and exclusion criteria were applied, the selected files were numerically labeled from 1 to 500 to protect the identity of the patients. The radiological and histopathological reports were reviewed, after which the data were entered into an Excel spreadsheet and analyzed using the Statistical Package for Social Sciences (SPSS) software version 2.0 (IBM, Armonk, NY, USA).
Statistical analysis
Categorical variables were presented as frequencies and percentages, and continuous variables were presented as the mean ± standard deviation (SD). Receiver operating characteristic curves were presented for the sensitivity and 1- specificity of the CT scan and US for the diagnosis of acute appendicitis. The true positive and false negative values for CT and US diagnosis of acute appendicitis were calculated.
As all the required data were retrospectively collected, no data was missing in this study, and missing data management was not required. The analysis was performed with a 95% confidence interval using SPSS.
Results
Of 500 medical records, 200 met the inclusion and exclusion criteria. The mean ± SD age of all patients was 25.50 ± 9.61 years. Approximately one-third (33%) of the patients were female. More than half (n=104, 52%) underwent open appendectomy, and the remaining patients underwent laparoscopic appendectomy. The mean ± SD Alvarado score of all patients was 6.41 ± 1.89. The clinical probability of acute appendicitis (according to Alvarado score) was high. The majority (93%) had acute appendicitis. Others had fibrous obliteration of the tip granulomatous appendicitis luminal fibrosis with chronic inflammatory cells or serosal congestion. The imaging statuses of the patients are found in Table 1.
Distribution of all variables (n=200).
Of the 200 patients who met the study criteria, 187 (93.5%) were diagnosed with acute appendicitis by histopathology. Of these 187 patients, 57 (30.5%) underwent CT, and 54 (29%) underwent US (Table 2). Computed tomography correctly identified 86% (49 out of 57) of patients as having acute appendicitis (true positive) and incorrectly identified 14% of patients as not having acute appendicitis (false negative). Similarly, US correctly identified 37% of patients as having acute appendicitis (true positive), while the remaining 63% of patients were incorrectly identified as not having acute appendicitis (false negative).
Imaging status of patients with confirmed acute appendicitis (n=187).
Thirteen patients (6.5%) did not have acute appendicitis (confirmed by histology report). Six (46.15%) of these 13 patients underwent CT and 5 of the 6 (83.3%) were incorrectly diagnosed (false positive) with acute appendicitis by CT, whereas one of the 6 (16.7%) was correctly identified as a true negative. On the other hand, US diagnosed 0% of these patients as false positive and 100% patients as true negative (Table 3).
Imaging status of patients with confirmed diagnosis other than acute appendicitis (n=13).
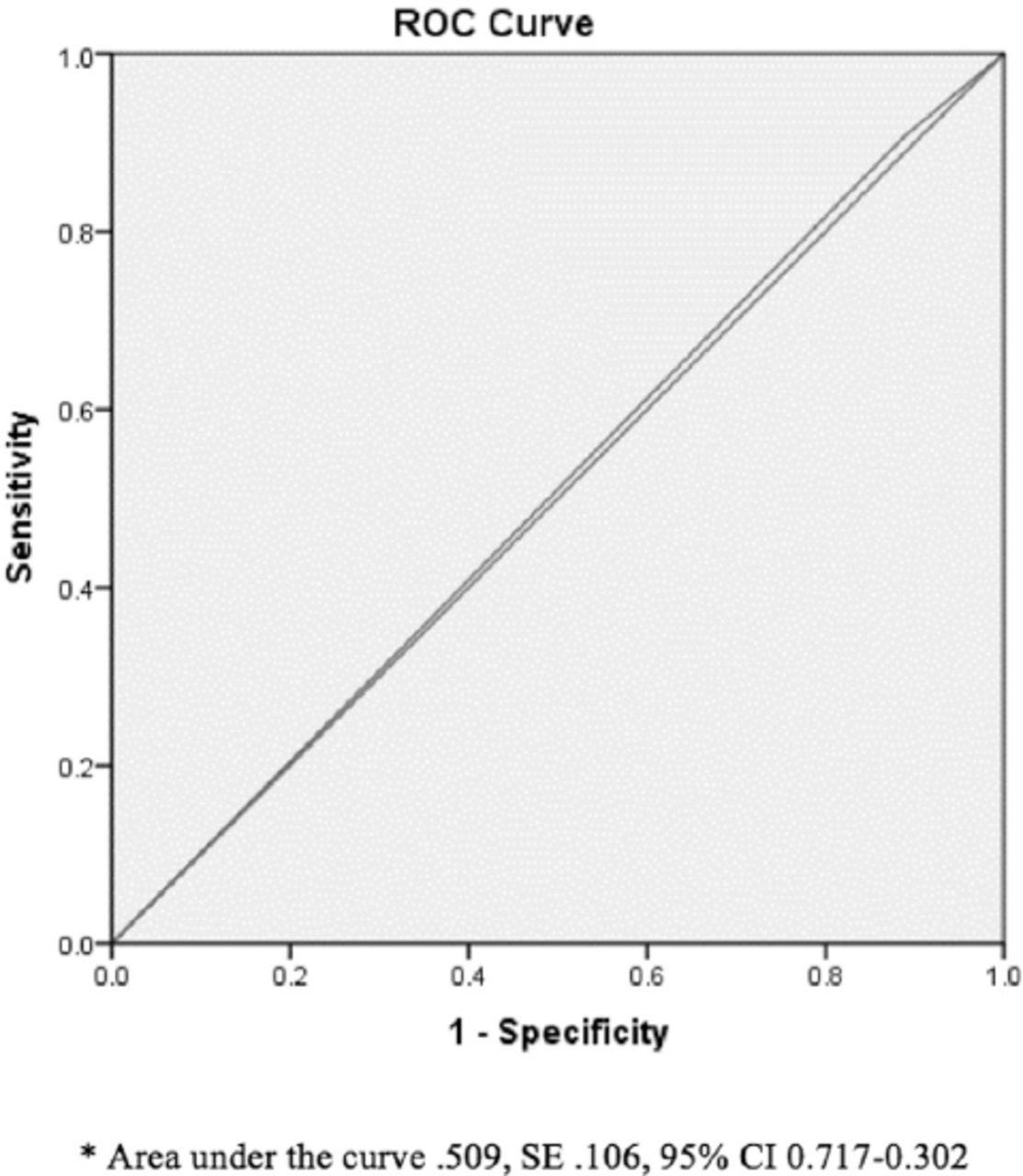
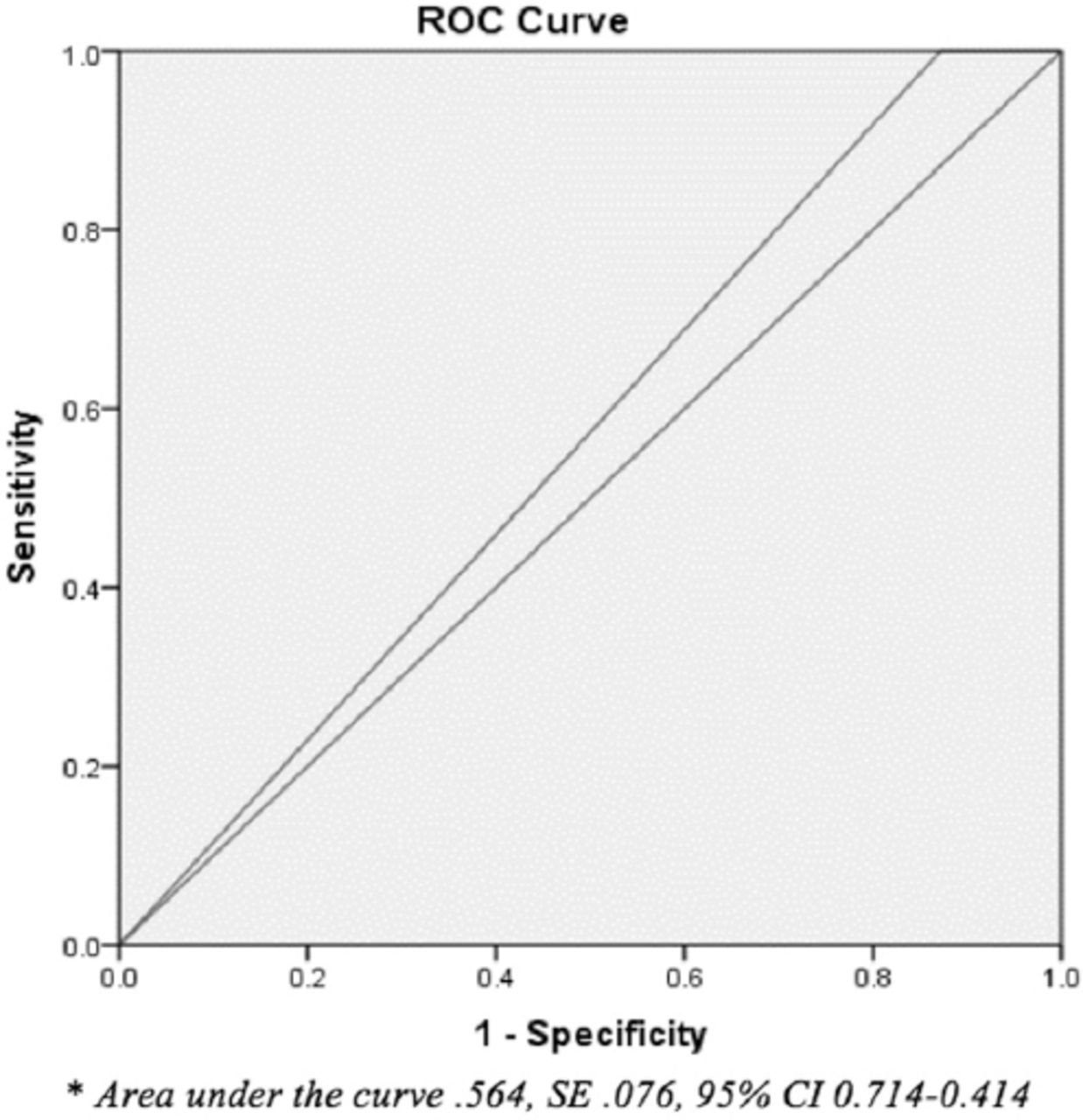
Our results revealed the sensitivity of CT for diagnosing acute appendicitis to be 86% and the specificity to be 16.7%. The sensitivity of US for diagnosing acute appendicitis was found to be 37%, and specificity was found to be 100% (Table 4).
Sensitivity and specificity of computed tomography (CT) and ultrasound (US) in diagnosing acute appendicitis.
Receiver operating characteristic curve for the sensitivity and 1-specificity of CT scan and ultrasonogram in diagnosing acute appendicitis is shown in Figures 1 and 2.

Receiver operating characteristic (ROC) curve showing the sensitivity and 1-specificity of CT scan in diagnosing acute appendicitis. (n=63).

Receiver operating characteristic (ROC) curve showing the sensitivity and 1-specificity of ultrasonogram in diagnosing acute appendicitis (n=59).
Discussion
Computed tomography and US remain the most effective and widely used radiological tests for the diagnosis of acute appendicitis. In the current study, the sensitivity of CT was found to be high in comparison to US. These findings are in line with previous study9 that found the accuracy of US to be lower than CT; however, US was found to be more specific than CT. The current study revealed the sensitivity of CT to be 86% and its specificity to be 16.7% when diagnosing acute appendicitis. On the other hand, the sensitivity of US was 37% and its specificity was 100%.
Due to the exclusion of equivocal tests in this study, the sensitivities and specificities of CT and US were found to be relatively lower than in previous reports. In addition, inherent bias, common whenever small sample sizes are studied (as in this retrospective study), has been found to alter the accuracy of tests.10 False positive results are prevalent with the use of CT, and, in this study, they amounted to 83.3% which have been negative for acute appendicitis in US. The study, on the other hand, was limited in that true sensitivity and specificity could not be determined. In order to avoid unnecessary radiation exposure, the patients diagnosed positively with US did not also undergo CT scans.11 Regardless of the major technological advances in radiographic imaging and continued advocacy for CT as a diagnostic tool, detecting appendicitis requires more than one diagnostic method. There is a need for all patients to undergo a comprehensive diagnosis before they undergo surgery or receive medication.
The sample size was smaller than expected. In patients with positive findings on US, CT was not performed to avoid radiation exposure.
In conclusion, the study underlined the sensitivity of CT was 86.0% against its specificity of 16.7% when diagnosing acute appendicitis. Furthermore, the sensitivity was marked at 37% and 100% specificity of US in diagnosing acute appendicitis. Therefore, detecting appendicitis radiologically necessitates using of CT to enhance all-inclusive diagnosis before undertaking medication or surgery. Ultrasound can be used to exclude gynecological disorders.
Acknowledgment
The authors would like to express their gratitude to Mr. Abdulaziz Alfawzan, Director, King Fahad Specialist Hospital, Buridah, Saudi Arabia for his support and to the staff of the medical files department for their cooperation. We would like to thank Editage by Cactus (www.editage.com) for the English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received November 22, 2018.
- Accepted March 19, 2019.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.