


Abstract
Objectives: To investigate and establish the relationship between the use of statin therapy and the risk of development of diabetes.
Methods: PubMed and the Cochrane Central Register of Controlled Trials was searched for randomized controlled end-point trials of statins, with more than 1000 subjects and a minimum of one-year follow-up period, published until August 2015. The odds ratio (OR) of diabetes incidence with overall statin therapy as well as with different statins in question was calculated through random effect meta-analysis model.
Results: Fourteen studies were included in the analysis with a total of 94,943 participants. Of these, 2392 subjects developed incident diabetes in the statin and 2167 in the placebo groups during a 4-year follow-up. The OR of diabetes incidence with statin therapy was significantly higher as compared with the placebo group (OR=1.11; 95% confidence interval = 1.0 to 1.2; p=0.007). There was an insignificant level of heterogeneity between the included trials (Cochran Q= 19.463, p=0.109, I2=33.20). Subgroup analysis showed that only 2 statins namely, atorvastatin (OR= 1.29; p=0.042) and rosuvastatin (OR = 1.17; px=0.01) were significantly associated.
Conclusion: Statin therapy can slightly increase risk of incident diabetes in subjects with hypercholesterolemia.
Statins are established drugs for the treatment and management of cardiovascular diseases (CVD) and revolutionized the treatment of high risk patients.1 Statins mainly reduce serum cholesterol content by inhibiting biosynthesis of 3-hydroxy-3-methyl-glutaryl-CoA reductase (HMG-CoA reductase) and isoprenoids.1,2 Other pleiotropic mechanisms of statins facilitating cardioprotective properties include improvement of endothelial dysfunction, increased nitric oxide bioavailability, antioxidant properties, inhibition of inflammatory responses, and stabilization of atherosclerotic plaques.3 Simvastatin and lovastatin are prescribed as lactone pro-drugs that are hydrolyzed enzymatically in vivo to their active hydroxy-acid form.4 Other statins are administered as the active hydroxy acid form.5-7
Focused management strategies for the regulation of higher levels of low density lipoprotein cholesterol (LDL-C) in populations at the risk for coronary heart disease (CHD) have been recommended by the Adult Treatment Panel (ATP) during 1988 (Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults [Adult Treatment Panel II] 1993). Critical limits for risk assessment of LDL-C have been categorized into 3 namely normal people (<3 mmol/l), high-risk people (<2.6 mmol/l) and very high-risk individuals (<1.8 mmol/l). Statins have been identified and employed as first-line therapeutics for treating high cholesterolemia since 1986. Multiple number of statins with variable therapeutic efficacies are available.8
Many clinical trials have demonstrated the safety and tolerability of the statins with appreciable risk/benefit ratio and transient and mild adverse effects such as headache, rashes, and gastrointestinal symptoms.9 However, there is an accumulation of clinical trial data observed on the adverse effects of statins comprising an asymptomatic increase in hepatic enzymes and musculoskeletal disorders. Pooled analysis of data involving 16,495 patients from 44 clinical trials has shown that withdrawal of statin in patients due to statin related adverse events was only 3-4%,10 and serious treatment associated effects were reported as <1% of patients. Recent evidence suggested that the use of statins may be associated with the emergence of new cases of diabetes prompting the U.S. Food and Drug Administration (FDA) to issue a safety label change for statins.11 Further, in 2013 the American College of Cardiology/American Heart Association (ACC/AHA) published cholesterol treatment guidelines indicating the risk of diabetes in relation to statin therapy.12 Post hoc studies, intervention trials, and statistical reviews on the diabetes risk associated with statin therapy proclaimed contradictory outcomes on this critical issue between 2000 and 2011.13-21 Heterogeneity among statins in inducing diabetes among patients undergoing statin therapy was apparent through different investigations on large populations from different regions.22,23 Dose and intensity of statin therapy are other aspects being explored for their influence on onset of diabetes among patients.19,24 However, the long-term effects of statin therapy induced diabetes yet to be understood.
Numerous studies conducted during recent years provide a multitude of evidence to help understand the link between statins and diabetes with debatable findings. The present systematic review makes an effort to summarize current knowledge and improve the understanding of this phenomenon, which sould help in designing a better clinical approach for statin therapy. The aim of this review is to evaluate the risk of diabetes mellitus under statin therapy, and to understand the impact of different statins on the odds of diabetes mellitus risk.
Methods
This study was conducted between March and August 2015. To retrieve all the published studies, an iterative search strategy was built up from a series of searches and thorough evaluation of the results. The strategy was built up through Population Intervention Comparison Outcomes Study Design (PICOS) methodology.
Inclusion and exclusion criteria
Randomized clinical trials examining the effects of statin therapy at an individual level with the objective of evaluating the risk of incident diabetes were included in this study. The studies, which employed placebo, or control comparison of different statins, or different doses of statins were used. In addition, studies where the sample size of patients with diabetes was more than 1000 with a mean follow-up of more than one year were included. Studies including patients on statin therapy with organ transplant, or hemodialysis were excluded for evaluation. Studies with single statin, or those in which diabetic patients on statin therapy with a sample size of less than 1000 were also excluded from the evaluation. Trials assessing change in surrogate markers of cardiovascular diseases and trials with a mean follow-up of one year, or less were also excluded. An exhaustive search strategy was developed to identify the studies for this review. The search strategies were developed for 2 major databases of Randomized Controlled Trials (RCTs) namely, the National Center for Biotechnology Information’s PubMed, and the Trials Registry of Cochrane Library.
Main outcomes of the study were analyzed by tabulation. Any significant differences in the comparison were recorded in the results section and interpreted logically. Risk of diabetes after statin therapy was the main result of this study.
An events rate with 95% confidence interval (CI) was chosen as most of the studies had reported events as well as sample size. The Cochran Q, a Chi square based test was used to assess the heterogeneity (between study variability) in the meta-analysis. A significance level of p<0.05 was used for statistical test of heterogeneity. While ‘Q’ statistic provided the qualitative information on the existence of heterogeneity, ‘I2’, that is calculated as the percentage of the total variability in a set of effect sizes due to true heterogeneity, was used to quantify the degree of heterogeneity.
High resolution forest plots were derived to estimate the pooled event rates corresponding to 95% CI and the p-value. Random effects model of meta-analysis was used for data analysis. Publication bias was investigated by using the funnel plots constructed based on the standard error by log odds ratio (OR). The report was prepared as per the standards of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.25
Results
Fourteen studies were found to provide the relevant data as per the criteria and were shortlisted (Figure 1).13-17,26-33 These studies provided data for 94,943 non-diabetic participants, of these, 4,599 developed incident diabetes. The mean study follow-up was 4 years (Table 1). The relative percentage reduction in blood cholesterol across the people subjected to statin therapy considered during the current review is presented in Table 2.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines flow diagram of literature search for identification of studies.
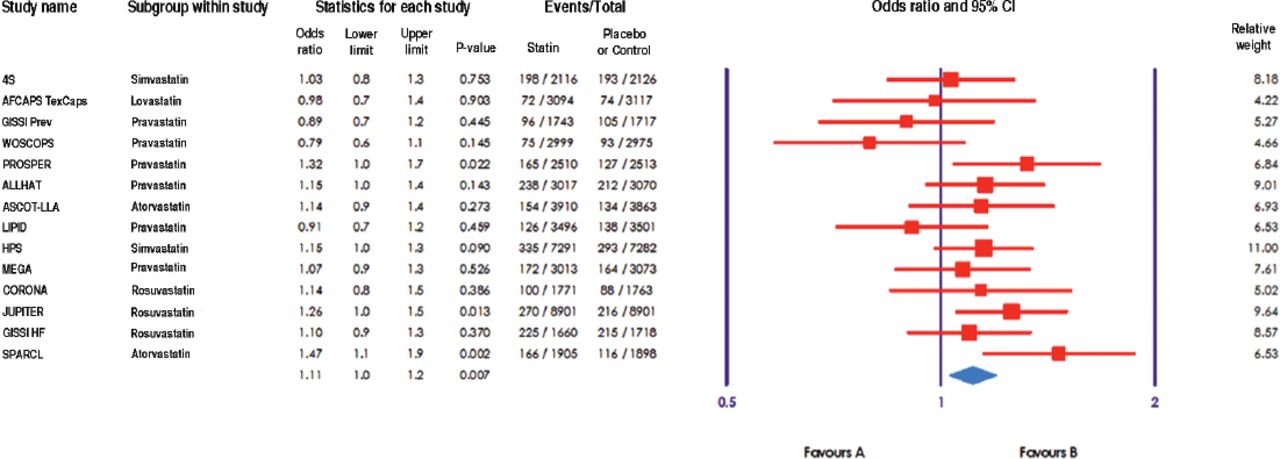
New onset of diabetes in non-diabetic participants in 14 placebo controlled and standard care controlled statin therapy trials.
Trends in LDL-C reduction in non-diabetic participants in 14 placebo controlled and standard care controlled statin therapy trials.
Heterogeneity test revealed that the included trials were homogeneous (Cochran Q = 19.463, p=0.109, I2 = 33.20). Rate of diabetes incidence in individual trials were found to be drastically varied (Figure 2). Of the 14 trials, 9 studies showed positive association between statin therapy and incident diabetes; however’ only 3 were significant (Pravastatin in elderly individuals at risk of vascular disease [JUPITER],14 Pravastatin in elderly individuals at risk of vascular disease, [PROSPER],32 and Stroke Prevention by Aggressive Reduction in Cholesterol Levels [SPARCL]).26 The overall OR of developing incident diabetes was significantly higher on statin use as compared with the control groups (OR = 1.11, p=0.007). Since the heterogeneity was very low, variation was not attributable to chance alone.

Association between statin therapy and incident diabetes in 14 major randomized controlled trials. 4S - Scandinavian Simvastatin Survival Study Group, AFCAPS/TexCAPS - Air Force/Texas Coronary Atherosclerosis Prevention Study, GISSI Prev - Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico Prevention, WOSCOPS - West of Scotland Coronary Prevention Study, PROSPER - Pravastatin in elderly individuals at risk of vascular disease, ALLHAT - Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial, ASCOT-LLA - Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm, LIPID - Long-Term Intervention with Pravastatin in Ischaemic Disease Group, HPS - Heart Protection Study, MEGA - Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese, CORONA - Controlled Rosuvastatin Multinational Trial in Heart Failure Trial, JUPITER - Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin trial, HR - heart failure, SPARCL - Stroke Prevention by Aggressive Reduction in Cholesterol Levels, 95% CI - 95% confidence interval
Cumulative analysis showed that the positive effect of statins on diabetes initiation appeared after sixth32 and significance after the eleventh30 (Figure 3). Funnel plot showed that publication bias was absent as the studies were distributed symmetrically on both sides of the combined effect size and no imputed studies were plotted (Figure 4).

Cumulative meta-analysis of the studied clinical trial by year of publication. 4S - Scandinavian Simvastatin Survival Study Group, AFCAPS/TexCAPS - Air Force/Texas Coronary Atherosclerosis Prevention Study, GISSI Prev - Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico Prevention, WOSCOPS - West of Scotland Coronary Prevention Study, PROSPER - Pravastatin in elderly individuals at risk of vascular disease, ALLHAT - Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial, ASCOT-LLA - Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm, LIPID - Long-Term Intervention with Pravastatin in Ischaemic Disease Group, HPS - Heart Protection Study, MEGA - Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese, CORONA - Controlled Rosuvastatin Multinational Trial in Heart Failure Trial, JUPITER - Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin trial, HR - heart failure, SPARCL - Stroke Prevention by Aggressive Reduction in Cholesterol Levels, 95% CI - 95% confidence interval

Funnel plot of standard error by log odds ratio for the included studies on statin induced diabetes.
The OR was further analyzed based on the type of statins (Figure 5). The tests revealed that only 2 statins, atorvastatin (OR = 1.29; 95% CI = 1.0-1.6; p=0.042) and rosuvastatin (OR = 1.17 95% CI = 1.0-1.3; p=0.01) were significantly associated with diabetes.

Association between individual statins and incidental diabetes mellitus. 95% CI - 95% confidence interval
The incidence of diabetes in the study population was highest in the placebo groups in the simvastatin trials (5.2%), followed by pravastatin (5%), atorvastatin (4.3%, p<0.05), rosuvastatin (4.2%, p<0.05), and lovastatin (2.4%). While this was lower than the treated groups in all statins, it was higher compared with the lovastatin treated subjects. The incidence was significant for atorvastatin and rosuvastatin as compared with the placebo group. Compared with lovastatin, the OR of developing incidental diabetes with pravastatin was 1.05 was times, simvastatin was 1.12 times, rosuvastatin 1.19 was times, and atorvastatin was 1.32 times.
Discussion
The present work is a meta-analysis of the incidence of diabetes mellitus upon chronic use of statins. The analysis of data showed that subjects treated with statins have a slightly higher chance of developing diabetes as compared to placebo, or standard care. Further analysis involving the comparison of different statins on diabetes incidence showed that only 2 statins, atorvastatin and rosuvastatin, showed significant association with diabetes whereas other 3 statins showed no significant incidence. Although no insights into the mechanism of these associations can be adjudged, one previous study34 conducted to evaluate the effects of statins on glucose transporters showed that except atorvastatin, other statins exert no detrimental effects. Therefore, the association of diabetes incidence with atorvastatin and rosuvastatin treatment was likely due to the inhibition of glucose transporters and needs further research. Statins affect insulin sensitivity through several mechanisms. A meta-analysis of 16 statin studies reporting insulin sensitivity data revealed that pravastatin can reduce the insulin secretion whereas other statins including atorvastatin, simvastatin and rosuvastatin has no such effect over insulin.35 Such alterations may affect insulin sensitivity and lead to diabetes.36
Other studies have suggested that altered glucose uptake by decreased glucose transporter type 4 expression or translocation might be the mechanism.34,37 In vitro studies have shown that atorvastatin, but not pravastatin show impaired glucose handling. This reflects the variation in clinical effects observed with different statins. Leptin, an adipocyte-secreted hormone is another pathway through which statins may act. Leptin resistance or lowered leptin levels are believed to promote insulin resistance, leading to diabetes through a complex mechanism, including lowered insulin secretion and beta-cell depletion.38,39
Other mechanisms proposed are inhibition of glucose-induced cytosolic calcium signaling and insulin secretion through blockage of L-type calcium channels,40 impaired insulin secretion through an indirect mechanism related to chronic cholesterol depletion,41 and statin associated weight gain. However, these findings need substantial future research to associate with the observed statin effects. Another potential explanation based on the residual confounding factors suggest that improved survival, or change in lifestyle with statin therapy may promote diabetes.42 However, overall survival with control therapy and statin use has been found to be similar. This meta-analysis included all available large studies; providing good statistical power to the conducted analysis. The meta-analysis was conducted using events rate and the results were expressed as OR, as hazard ratio was not provided by all the included studies. Different methods were employed for the diagnosis of diabetes by the included trials, which are expected in such studies. Furthermore, 2 studies,15,30 The Heart Protection Study, (HPS) and the Controlled Rosuvastatin Multinational Trial in Heart Failure Trial (CORONA) were used by some physicians in reporting for the diagnosis of diabetes, which could be unreliable as compared with diagnostic tests.
This meta-analysis studied the association between statin therapy and incidence of diabetes in 14 major randomized controlled trials. Out of 14 studies, only 9 showed a positive association between statin therapy and incident of diabetes with 3 studies (PROSPER [p=0.022], JUPITER [p=0.013], and SPARCL [p=0.002]) showing significant association (p<0.05). Further, a cumulative meta-analysis of these studied trials was carried out according to the year of publication, and it was found that positive effect of statins on diabetes mellitus initiation appeared after the sixth study, and significance after the eleventh study. All the types of statins analyzed exhibited good control over LDL-C, rosuvastatin was recorded as the highest percentage reduction over 12 months of treatment. However, its proved association with incidental diabetes, demands a reconsideration of this statin for use with cardioprotective purpose. A previous study45 evaluated the risk of statin drugs in incidental diabetes in identified women, elderly people, and the Asian population as the critical groups at higher chances of developing the problem. However, more studies are required for validating the higher risk of Asian people in statin therapy associated incidental diabetes.43
Our results suggest that it is essential to monitor patients receiving statins for the risk factors of diabetes. Prolonged durations of use of these drugs increase the requirement of regular monitoring. In-addition, the clinical use of atorvastatin and rosuvastatin should be reconsidered, as these 2 statins showed a strong and clear association with diabetes incidence. Furthermore, it is necessary to consider development of diabetes as one of the study parameter in all the future trials of statins. This will perhaps be highly useful in extracting valuable information especially from long-term studies with great clinical implications.
Although the present meta-analysis reports an association of statins with incident diabetes such as earlier studies, the benefits of statins cannot be outweighed based on the following points: i) Statins importance in protection of the hyperlipidemic patients from severe cardiac outcomes. ii) Although the meta-analysis is significant, the rate is low. iii) Away of these factors, the patient status and demonstration could have an impact on the incidence of diabetes mellitus
This analysis was based on studies that have been followed up for either 12 months, or more, it can also be suggested that statins may continue to be used in high risk cardiovascular patients for shorter, or medium duration treatments without a cause for concern. However, if the patients are in the low cardiovascular risk zone, it is better to reconsider the use of statins even for short term durations, especially atorvastatin and rosuvastatin. after comparing the statins OR atorvastatin was found to hold the highest OR at 1.29. After considering lovastatin, which holds the lowest OR as a reference, the association risk of diabetes mellitus for lovastatin is considered one, whereas pravastatin was found 1.05 times, simvastatin 1.12 times, rosuvastatin 1.19 times, atorvastatin 1.32 times greater for diabetes compared with lovastatin.
The study limitation of the current systematic review is that we screened only 2 databases (PubMed and Cochrane Central).
In conclusion, the current review has established the effectiveness of statins in cholesterol lowering on patients with hypercholesterolemia. The existence of positive association of statin therapy with incidental diabetes across the clinical trials has been confirmed. Comparative evaluation of different types of statins in eliciting new onset diabetes among patients has confirmed the role of atorvastatin and rosuastatin in inducing incidental diabetes.
- Received July 10, 2016.
- Accepted August 7, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.