


Abstract
Objectives: To evaluate the clinicopathological features and treatment outcomes of papillary thyroid carcinoma tall cell variant (PTC-TCV) in Saudi population.
Methods: This retrospective study were medical records of 776 treated PTC patients between December 2007 and 2015, at King Fahad Medical City and King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia was probed for PTC-TCV. Total 42 (5.4%) patients were found to have PTC-TCV, which were investigated for demographic, symptoms, histopathological features, and treatment outcomes locoregional control (LRC), distant metastasis control (DMC), disease free survival (DFS), and overall survival (OS) rates.
Results: Mean age of cohort was 52.3 years (range: 46-80), with female predominance (73.8%). Mean tumor size was 3.62 cm (range: 0.4-10). Rates of LVSI (59.5%), positive pathological lymph nodes (66.7%), multifocality (42.9%) and extrathyroidal extension, (45.3%). Median follow-up was 37.4 months (range: 6-60). Local recurrence rate were seen in 6/42 (14.2%) patients and 8/42 (19%) developed distant metastasis. The 5 year rates of LRC (82.3%), DMC (77.8%), DFS (69.2%), and OS (86.7%) multivariate analysis showed PTC-TVC as an important independent prognosticator (odds ratio: 4.2; 95% confidence interval: 1.79-7.3; p=0.03)
Conclusion: Papillary thyroid carcinoma tall cell variant is associated with aggressive biological behavior.
Most of papillary thyroid carcinoma (PTC) are associated with an exceptional long-term treatment outcomes including DFS and OS rates; however, some of histopathological variants of PTC have been found with more aggressive biologic behavior and poor perspective.1 Among these histopathological variants, tall cell variant (TCV) is considered the most aggressive variant of PTC.2 Mainly, PTC-TCV is characterized by a height greater than twice its width, eosinophilic cytoplasm, basaloid nuclei along with the conventional characteristics of PTC.3 In 2004, World Health Organization (WHO) defined a PTC as TCV if it contained 50% or more tall cells.4 Some controversies regarding the proportion of tall cell (30-75%) required for diagnosis of PTC-TCV still persist; however, most of institutes accept the threshold of > 30% to confirm PTC-TCV5 TCV has some distinctive differences with classic variant of PTC; A) frequent presence of lymphovascular space invasion (LVSI) and extrathyroidal extension (ETE), B) greater prevalence of pathological positive lymph nodes and distant metastases at the time of diagnosis, and C) its 10-year DFS and OS rates have been reported to be approximately 10-15% lower than that of classic PTC.6,7 However, data around PTC-TCV in Saudi population is very scanty. We undertook the present study to evaluate the various clinicopathological characteristics and treatment outcomes of PTC-TCV in Saudi population.
Methods
Patients were reviewed retrospectively. After an authorized approval from the institutional review committee, medical charts of 42 patients with PTC-TCV, who were treated at King Fahad Medical City and King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia between December 2007-2015, were investigated using database system. Inclusion criteria was patients PTC-TCV histopathology of all ages. Exclusion criteria was defined <10% proportion of tall cells in histopathological specimens. Patients with PTC-TCV were retrieved in the following fashion; clinical variables including age at the diagnosis, gender, and symptoms at the time of diagnosis were reviewed. Histopathological assessment was performed by a skilled histopathologist. Different histopathological variables including the size of primary tumor, presence of LVSI and ETE, multifocality, positive pathological lymph nodes, and tumor lymph node, and metastasis staging were collected. Data regarding different treatment modalities, including the type of thyroidectomy, neck dissection, and adjuvant radioactive iodine (RAI) ablation were also recalled.
Statistical analysis
The primary endpoint was DFS. Secondary endpoints were the locoregional control (LRC), distant metastasis control (DMC) and OS rates. The DFS was defined as, the duration between the date of thyroidectomy and the date of documented all-site disease recurrence, death from cancer and/or last follow-up (censored). All probabilities of LRC, DMC, DFS, and OS rates were shown using the Kaplan-Meier method (comparisons for different survival curves were performed using log rank). All statistical analyses were performed using the the Statistical package for Social Sciences (IBM Corp., Armonk, NY, USA) version 24.
Results
Among the 776 PTC patients managed in our centers between December 2007-2015, 42 patients (5.4%) were found to have PTC-TCV. Mean age of cohort was 52.3 years (range: 46-80), with female predominance (73.8%). Different attributes of cohort are shown in Table 1.
Characteristics of 42 patients with PTC-TCV, who were treated at King Fahad Medical City and King Khalid University Hospital, Riyadh, Kingdom of Saudi Arabia.
All patients underwent total thyroidectomy and near-total thyroidectomy. Most of cohort underwent central and lateral neck dissection (78.6%). Mean tumor size was 3.62 cm (range: 0.4-10). Lymphovascular space invasion was observed in 25/42 patients (59.5%), while positive pathological lymph node were seen in 28/42 patients (66.7%). Positive pathological lymph nodes were seen in 62.5% of patients with tumor size ≤ 2cm (16 patients) as compared with 28 patients with tumor size >2cm (64.3%) with p=0.20. Multifocality was seen in 18/42 patients (42.9%). No correlation was found between size of primary with multifocality, ETE (p=0.12, 0.17) and LVSI (p=0.21). Triiodothyronine (T3) and thyroxine (T4) stage was seen in 19 patients (45.3%). Two patients (4.8%) had distant metastasis at the time of diagnosis.
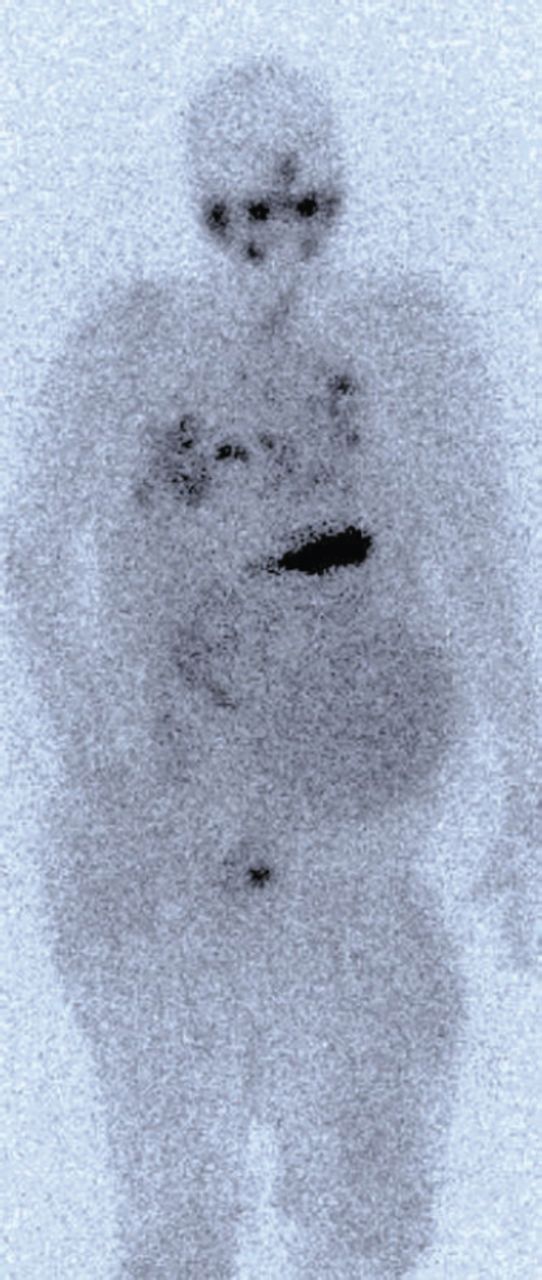
Adjuvant RAI was given to most of cases (39 patients, 92.8%). Median delay between surgery and adjuvant RAI was 8.5 weeks (range: 6-13). Doses were, 30 millicurie (mCi) in 5 patients (11.8%) for patients with primary size ≤2 cm without other risk factors; 100 mCi in 9 patients (21.4%) with positive margins, ETE and LVSI; 150 mCi in 23 patients (54.7%) with positive pathological lymph nodes and 200 mCi in 2 patients (4.8%) with distant metastasis. Postoperative radiation therapy (PORT) to thyroid bed and regional lymph nodes was given to 4 patients (3 patients with skeletal muscle invasion, one patient with tracheal invasion). Mean dose for PORT was 60 Gy (range: 60-66 Gy), given as daily 2 Gy/fraction, 5 days/week over 6-6.5 weeks (30-33 fractions). Median follow-up was 37.4 months (range: 6-60). Local recurrence rate (LRRs) were seen in 6/42 (14.2%) patients (Table 2). The LRRs were salvaged with neck resection (3 patients) followed by RAI (2 patients). Distant metastasis was seen in 8/42 (19%) patients. Among whom, 5 patients were treated with RAI, one patients with brain metastasis was managed with resection and radiation therapy and one patient with bone lesion was treated with palliative radiation therapy (Figure 1).
Treatment outcomes in our tall- cell variant papillary thyroid carcinoma.

Whole body scintigraphy showing iodine avid bilateral lungs, neck, and right femur uptake.
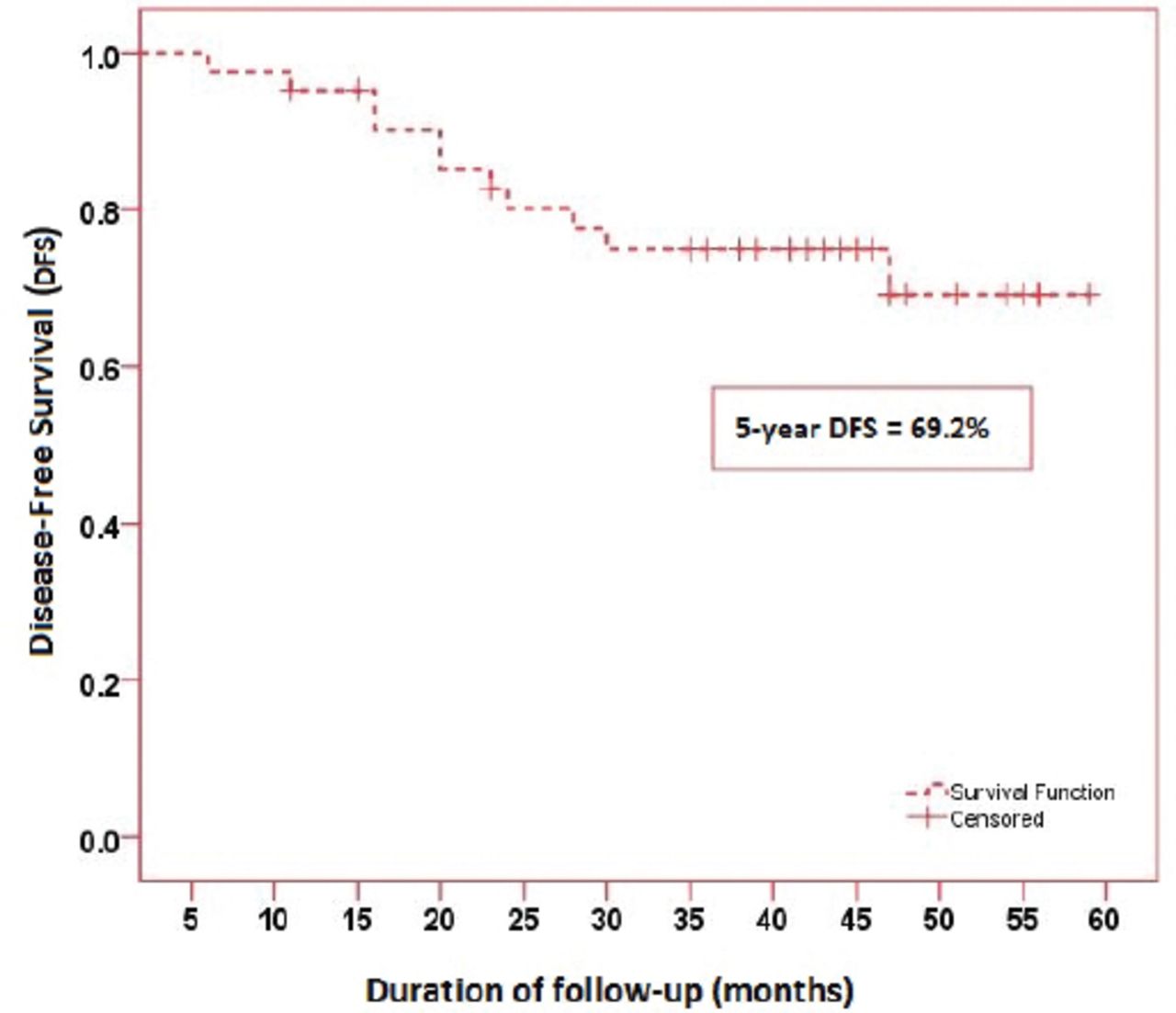
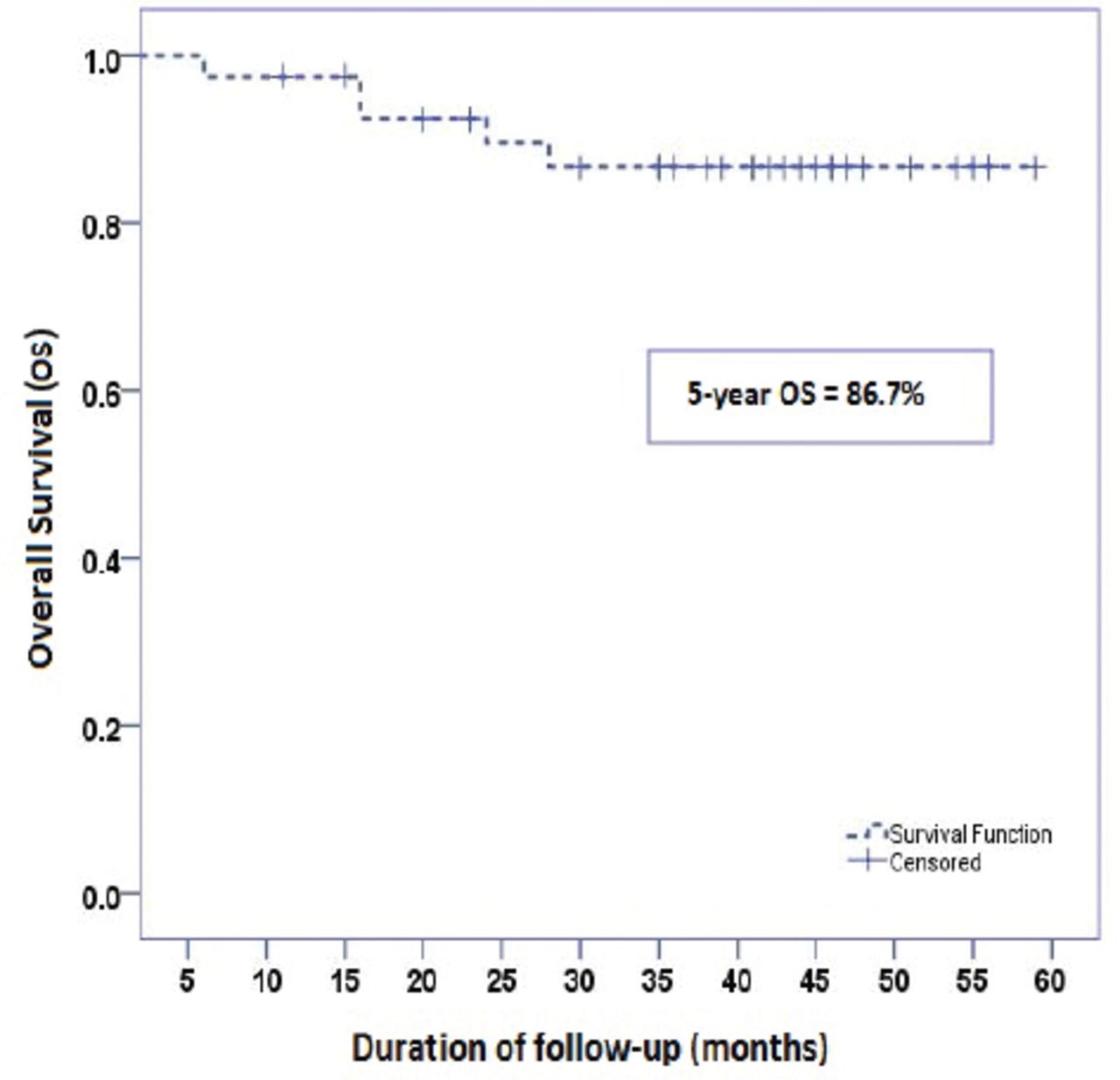
At the time of analysis, we found 5 year 82.3% LRC, 77.8% DMC, 69.2% DFS, and 86.7% OS (Figure 2 & 3). Further, univariate and multivariate analyses of different prognostic components for DFS and OS showed PTC-TVC as an important independent prognosticator (Odds ratio: 4.2; 95% confidence interval: 1.79-7.3; p=0.03).

Disease free survival of 42 cohort patients.
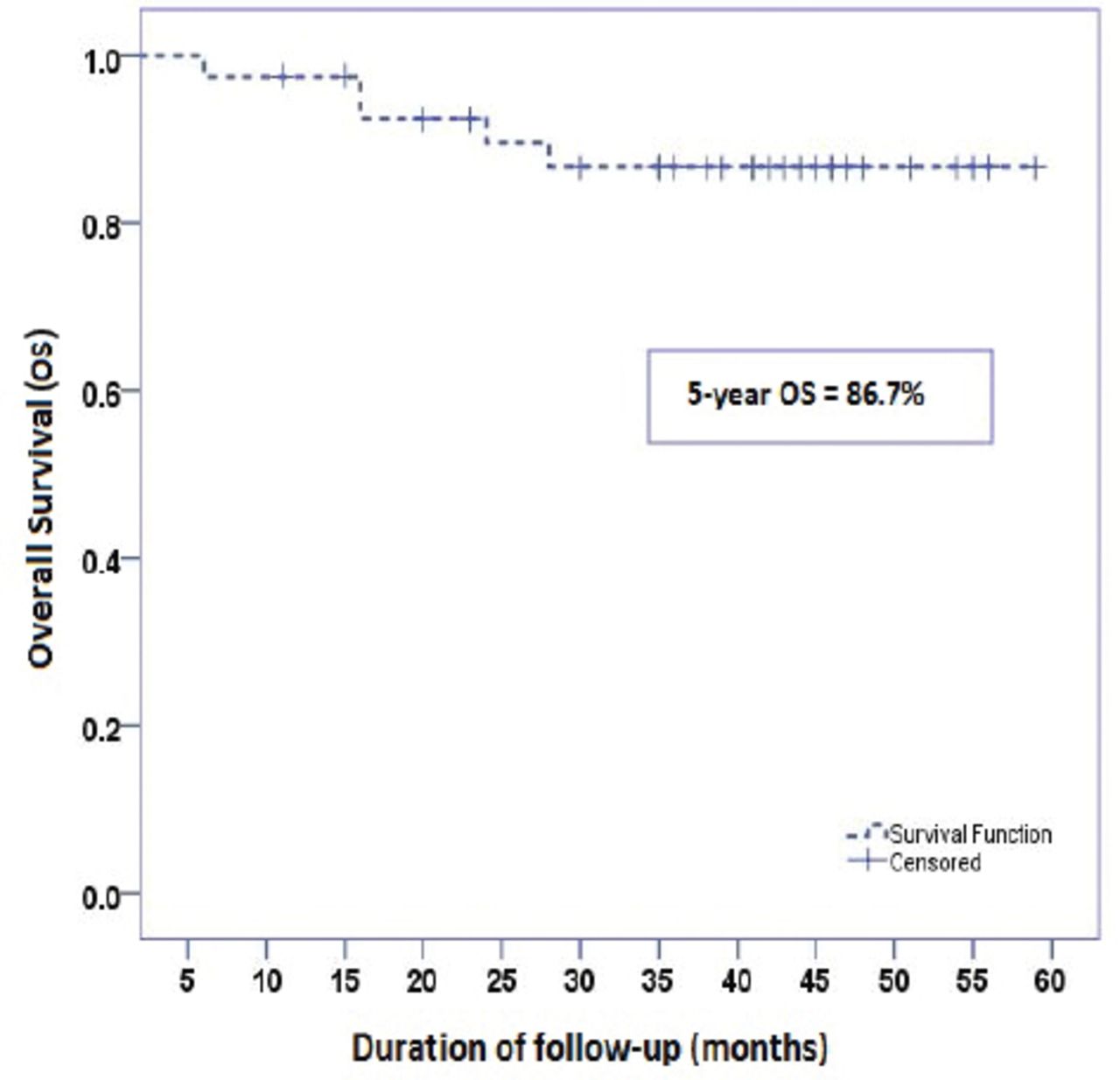
Overall survival of cohort 42 cohort patients.
Discussion
In the present study, PTC-TCV constituted 5.4% of all PTC cases, which is in agreement with the reported prevalence of 1.3-13% among of all PTC.1,8 The reason for this variation in reported prevalence can be explained by difficulty in distinguishing PTC-TCV from other histopathological variants, thus PTC-TCV is believed to be underdiagnosed in most of cases.9 In our cohort, women accounted for (73.8%) with the female to male ratio 3:1 is also in agreement with reported literature.10 Similarly, mean age of 52.3 years in our cohort study, is also in agreement with reported data.11 Further more, the multifocality (42.9%), pathological positive lymph nodes (66.7%) and distant metastasis (7.2%) at the time of diagnosis in our cohort were found to be similar to those reported in various studies.12 However, in disagreement with other studies, the percentage of ETE was comparatively low in our cohort (45.3% versus reported 63.9%). Mean primary tumor size was comparatively larger in our cohort (3.6 cm versus reported approximately 2.5-3 cm).1,5 Michels JJ et al13 also reported larger primary tumor size in their study of 56 patients with TCV. Due to these aggressive biological behavior, all patients in our cohort underwent total thyroidectomy. Although neck dissection (central and lateral) was performed in most of patients (78.6%), we recommend routine prophylactic central lymph node dissection at the time of thyroidectomy in PTC-TVC patients.1,13 Low occurrence of LRRs and distant metastasis in group, which received adjuvant RAI as part of management in our cohort, supports the notion that adjuvant RAI should be considered for all PTC-TVC patients, regardless of tumor size and lymph node status.6,14 In disagreement with similar reported data, PTC-TCV in our cohort had lower 5-year DFS rate (69.2%) after extensive treatment, which can be explained by our high risk cohort itself.15 In agreement with other related data, we found PTC-TVC as an important negative prognosticator.16
There were limitations in our study; A) small sample size, B) BRAF mutations were not analysed in our cohort, as current evidence suggests that PTC-TVC is associated with 80-100% BRAF mutations as compared with 63-83% in classic PTC,17 and C) rearranged during transcription/PTC (RET/PTC) gene rearrangements were also not examined. Among 13 different RET/PTC oncogenes, RET/PTC1 and RET/PTC3 represent the most common types.18 Recent data19 has shown a striking correlation between the RET/PTC3 rearrangement and the PTC-TCV phenotype (35.8% positive), which suggests that molecular pathogenesis in PTC-TCV may be different, which needs further investigations.
In conclusion, PTC-TVC is associated with aggressive biological behavior. Our results were found in agreement with previous studies. However, more molecular studies are warranted to address the role of BRAF mutations, and Rearranged during Transcription/PTC (RET/PTC) gene rearrangements in PTC-TVC.
Copyright
Whenever a manuscript contains material (tables, figures, etc.) which is protected by copyright (previously published), it is the obligation of the author to obtain written permission from the holder of the copyright (usually the publisher) to reproduce the material in Saudi Medical Journal. This also applies if the material is the authors own work. Please submit copies of the material from the source in which it was first published.
Footnotes
Disclosure. Authors have no conflict of interest, and the work was not supported or funded by any drug company.
- Received June 6, 2016.
- Accepted August 3, 2016.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.