


Abstract
Ureterocele is a congenital anomaly, in which there is mal-development of the caudal segments of the ureter. There is a female preponderance with most cases seen in Caucasians. Among the reported complications of this condition, chronic renal failure occurring in the setting of ureterocele has not been well documented. We report a case of a young girl with bilateral ureterocele presenting with chronic renal failure, whose management presented a diagnostic failure and inadequate treatment.
Ureterocele is a rare congenital cystic dilatation of the terminal segments of the ureter at its opening into the urinary bladder.1 The condition occurs almost exclusively in Caucasians.2 Ureterocele have been variously classified based on the anatomical and functional criteria. A simple and frequently used classification was developed by the American Academy of Paediatrics (AAP).3 There are controversies surrounding the etiology of ureterocele. However, the most commonly accepted theory in the pathogenesis of ureterocele is the incomplete dissolution of the Chwalla’s membrane during developmental stages. Other theories include incomplete masculinization and excessive dilation of the intramural ureter during the development of the bladder and trigone, and obstruction of the ureteral orifice. Commonly, ureteroceles are predisposed to urinary stasis and subsequent infection in neonatal periods. Ureterocele may manifest as failure to thrive in children, and abdominal or pelvic pain in adults. Other modes of presentation include; hematuria, purulent urine, and pyelonephritis. Urinary incontinence or retention may also be seen in the presence of obstruction at the level of the bladder. Ultrasonography is a useful diagnostic imaging tool in the prenatal and early childhood period.4 However, a voiding cystourethrography (VCU) and intravenous pyelography (IVP) for evaluation of the urinary tract and the voiding status are essential in the assessment of the excretory function. The degree of obstruction and the differential functions of the kidneys can be demonstrated with diuretic renograms. Cystoscopy, an endoscopic procedure that allows direct inspection and examination of the urinary tract is a helpful diagnostic procedure in the management of ureterocele. Management of ureterocele may not be generalized due to varied complications that may ensue. Endoscopically or surgically, unroofing of the ureterocele can be performed. The surgical procedures include excision of ureteroceles and reimplantation of ureters into the bladder for bladder level surgery, and partial heminephrectomy and ureterectomy for upper-level surgery. Endoscopic treatment includes transurethral puncture and transurethral incision, which are applicable mainly to the intravesical types. Despite the rarity of this condition among the Black race, there is a need for a high index of suspicion in order to prevent a possible irreversible renal failure among other associated complications. We report a rare case of chronic renal failure in an 18-year-old girl with bilateral ureterocele. Our objective in presenting this particular case is to highlight chronic renal failure requiring renal replacement therapy as a unique complication of ureterocele in a poor resource constrained developing country.
Case Report
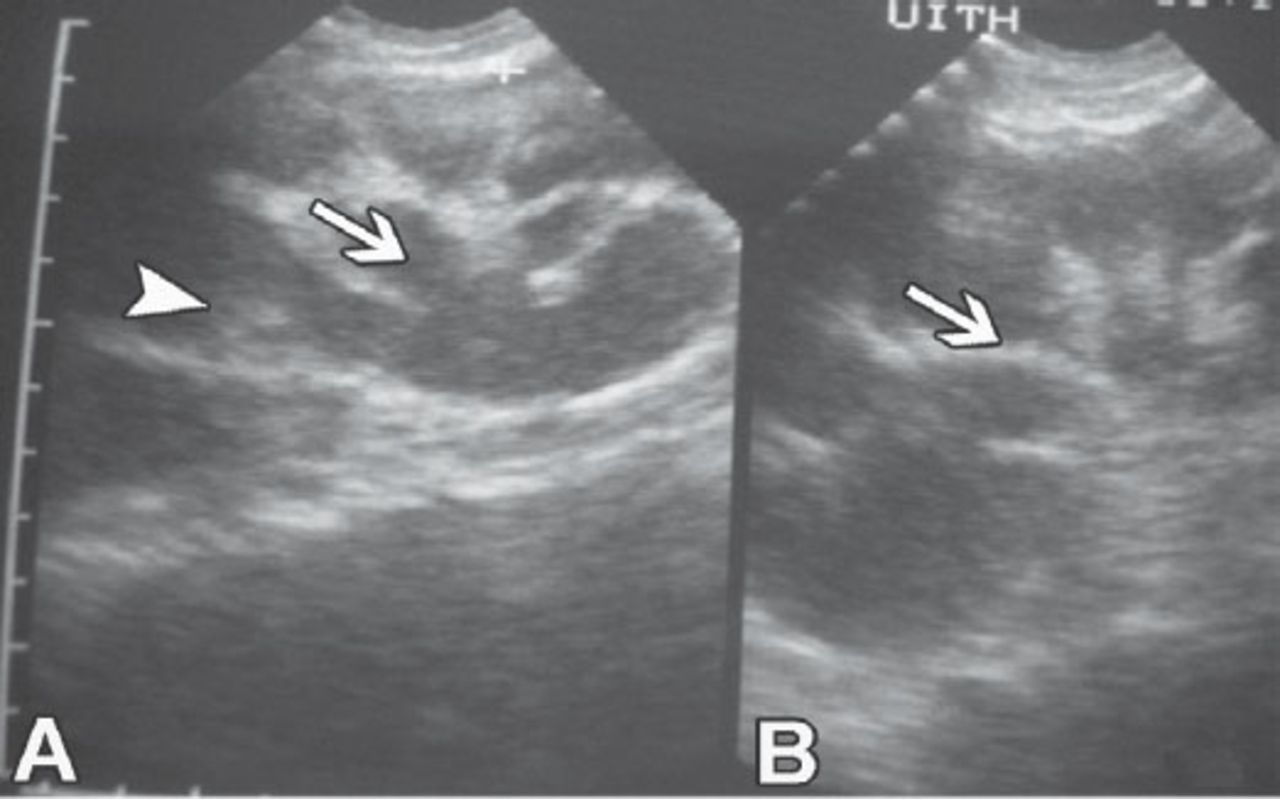
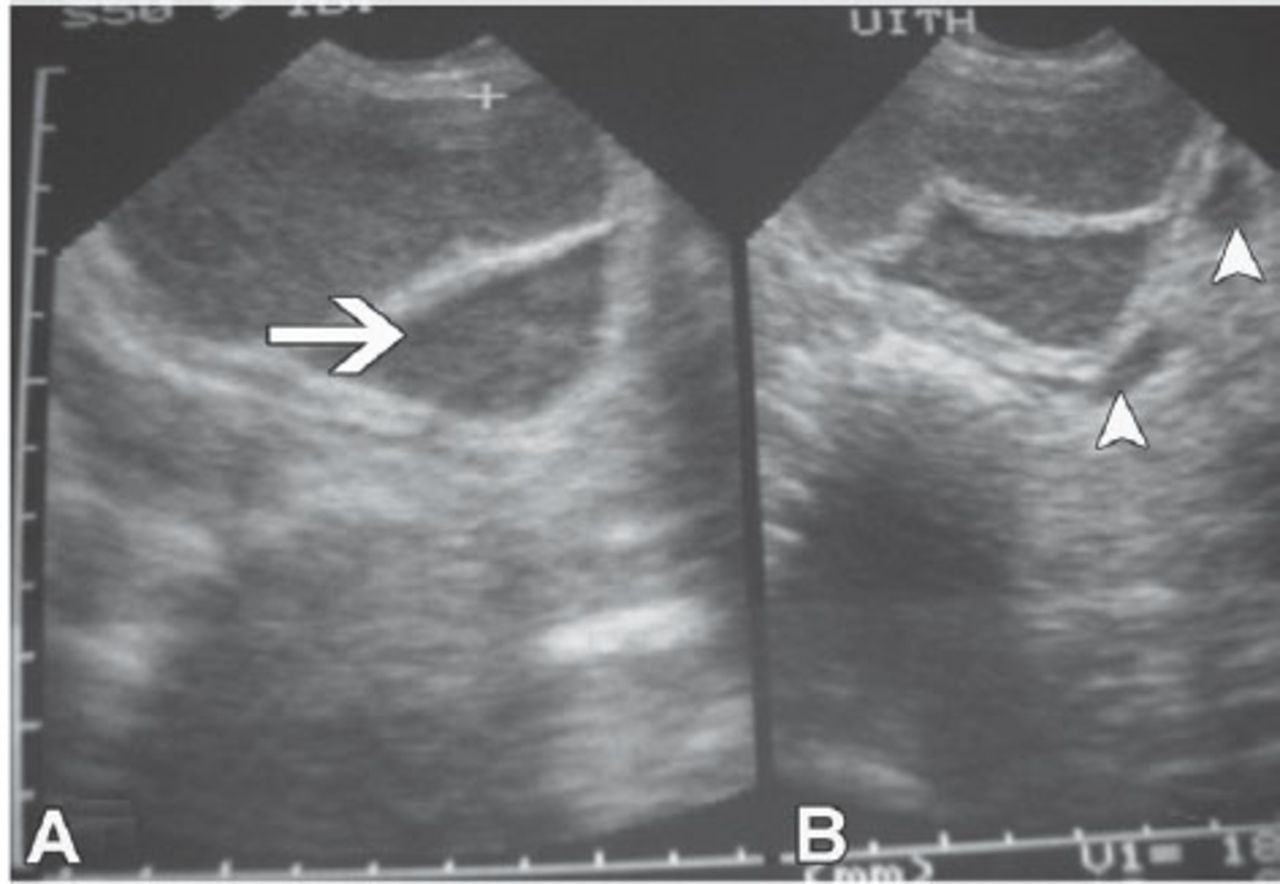
An 18-year-old girl was referred from a private health facility to the renal ward of the University of Ilorin Teaching Hospital, Ilorin, Nigeria. Her presenting complaints were 3 months history of recurrent facial and leg swelling, persistent vomiting, and reduction in urinary output. There was a history of hospital admission when she was 8-years-old in a health facility with complaints of lower abdominal pain and urinary retention. On examination, she was small for age with weight of 35 kg and a body mass index of 16.65 kg/m2. Initial results of investigation were as follows; sodium - 125 mmol/L (normal value [NV] - (135-145 mmol/L), potassium - 4.3 mmol/l, urea - 20.5mmol/l (2.5-7.1 mmol/L), and creatinine - 1006 µmol/L (53-106 µmol/L). Urinalysis showed protein 2+, blood 1+, pH - 6.0, and specific gravity of 1010. The estimated glomerular filtration (eGFR) was 6.3 mL/min/1.73m2. She was anemic with a pack cell volume of 17%. The serial serum electrolyte results showed persistent hyponatremia with azotaemia. The ultrasonography of the kidney, ureter, and bladder (KUB) revealed both kidneys were normal in position, they measured 13 cm on the right, and 12.5 cm on the left in their bipolar lengths. Both showed grossly dilated pelvicalyceal system filled with fluid, and cortical thinning, which confirmed grade IV bilateral hydronephrosis (Figures 1A and 1B). Both ureters were dilated and tortuous and they ended in cystic dilatation within the thickened wall of the urinary bladder giving a cyst within cyst appearance (Figures 2A and 2B). She had bilateral ureterostomy to relieve obstruction. Intra-operative finding by the urologists revealed a grossly dilated and bifid right ureter down to the ureterovesical junction, the left ureter was also dilated. After the surgery, the azotaemia persisted and conservative management for the chronic renal failure was ineffective in controlling the uremic symptoms as she could not afford dialysis because of financial constraints. She eventually requested to be discharge and was taken home by the parents on the sixteenth day of admission.
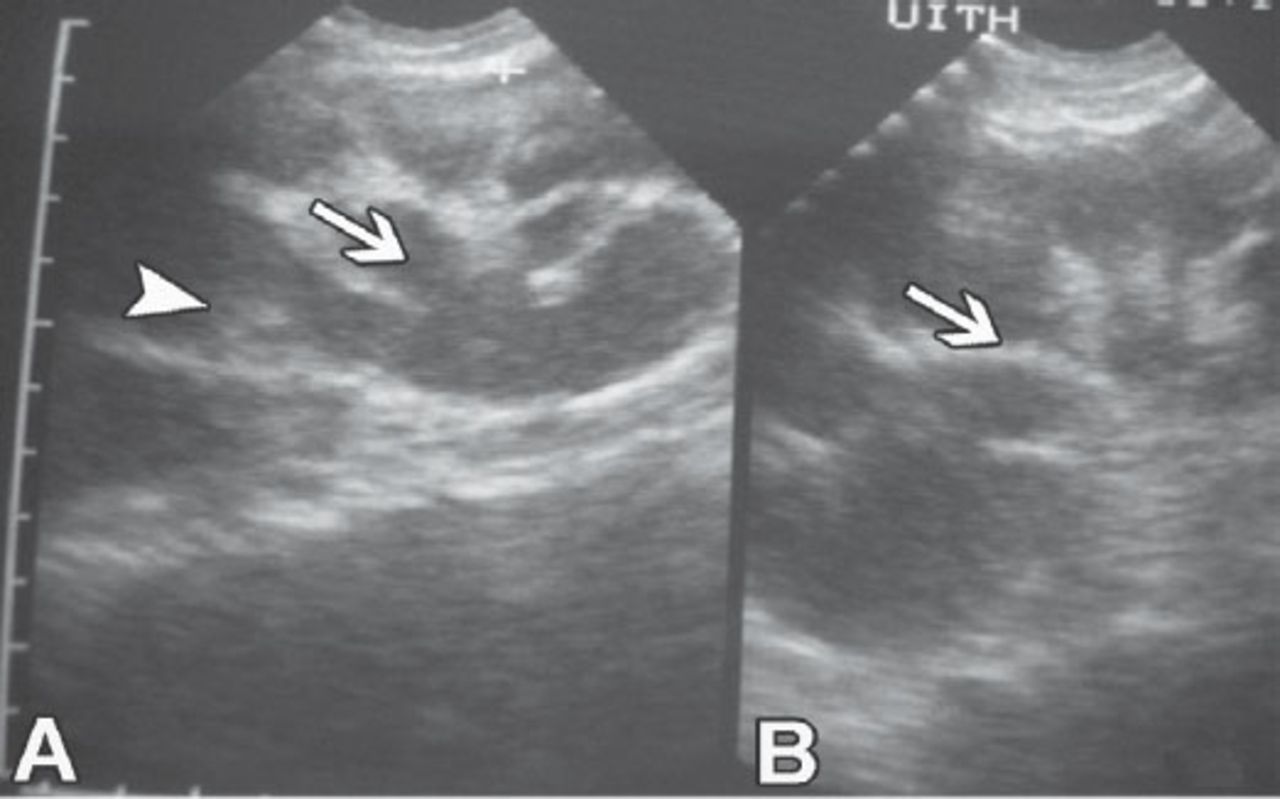
Ultrasound of the patient showing: A) bilateral dilated renal collecting system (arrow head), hydronephrosis (arrow), and B) cortical thinning (arrow).
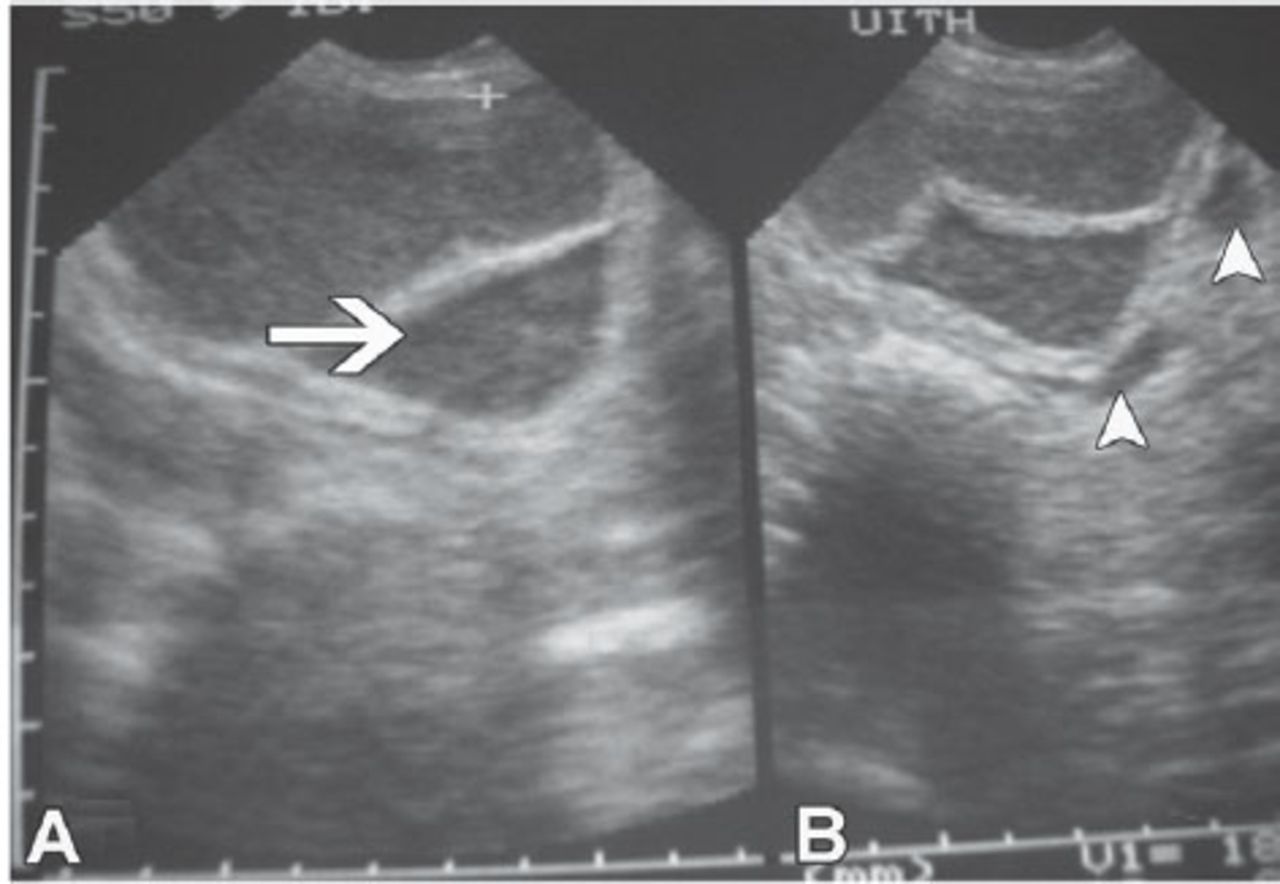
Ultrasound showing: A) dilated cystic distal portion of the ureters (arrow); and B) opening into the urinary bladder. Arrowheads indicating ureteroceles.
Discussion
This case illustrates a unique complication of ureterocele presenting with chronic renal failure requiring renal replacement therapy in a young Nigerian girl. Ureterocele is reported to affect one in 4000 individuals.5 Few cases of ureterocele have been documented in our country with none complicated with renal failure. It is bilateral in 10% of cases with female preponderance.1 The condition may be entirely asymptomatic and only incidentally detected during investigation for an unrelated illness. According to the American Academy of Pediatrics, ureterocele may be classified as intravesical (within the bladder) and ectopic (some portion in the bladder neck or urethra), simple or duplex system, and also may be described in term of orifices.3 Ureterocele is usually associated with a double collecting system whereby 2 ureters drain their respective kidney instead of one (duplex system ureterocele).6 A single collecting system has been documented in approximately 20% of cases.
Our patient had bifid right ureter and single ureter on the left side. Duplicated ureters are often associated with an obstructed upper pole moiety and a refluxing lower pole moiety; however, the degree of obstruction and functional impairment is variable depending on the type of ureterocele and the associated upper pole dysplasia. Ureterocele may also be associated with dysplastic or non-functioning kidneys predisposing such patient to the development of renal failure early in life. Such individuals will require renal replacement therapy for survival. In their case series, Chowdhary et al5 reported various complications of ureterocele including development of end stage renal failure. In a review of 305 children in a tertiary hospital, Hari et al7 documented a high proportion of renal failure due to obstructive uropathy. In some cases of ureterocele, a small upper portion of the kidney is congenitally non-functioning, which may necessitate the removal of this affected portion. Our patient had no developmental abnormality of the kidneys. Her presentation at the age of 18 years with chronic renal failure was sequel to prolonged obstruction of the bladder neck, by the large, cystic dilatation of the ureters. This is particularly possible in the ectopic, sphincteric, and sphincterostenotic types of ureterocele.8 Chronic incomplete obstruction resulting in back pressure effect on the bladder, ureter, renal pelvis, and the kidneys may account for the structural changes observed in the ultrasonographic scan and during surgery.
Our patient might have suffered recurrent episodes of clinical or subclinical urinary tract infection (UTI). Such infection in the setting of ureteral abnormalities might explain why she was small for age due to failure to thrive. Ureteric stones have been reported to be a common presentation in approximately 15-40% of adults with ureterocele.9 This was not found in this patient. The ureteral abnormality in our patient was detected at a time when irreversible structural and functional changes had occurred in the kidneys. Despite the surgery to temporarily relieve the obstruction, the azotaemia persisted. The electrolyte derangement observed in the patient was consistent with type III pseudohypoaldosteronism, which could be transiently induced by the combination of ureterocele, obstructive uropathy, and UTI.10 Type III pseudohypoaldosteronism is characterized by salt wasting, hyponatremia, hyperkalemia, elevated serum aldosterone, and decrease glomerular filtration rate.10 There was no facility to measure serum aldosterone in our center. If the ureterocele was detected early, endoscopic incision or surgical excision and reimplantation of the ureters may prevent progression to chronic renal failure.2,5
In conclusion, this case underscores the need for proper evaluation and follow-up of patients with childhood clinical features of urinary tract obstruction. This will allow for early detection of abnormalities of the urinary tract and treatment to prevent irreversible chronic renal failure. The case also illustrated the financial burden of chronic kidney disease being experienced by patients in resource-constrained developing country.
Acknowledgment
The authors gratefully acknowledge Dr. Chijoke Cosmas Achebe, Consultant Radiologist, Federal Teaching Hospital Ido Ekiti, Ekiti State, Nigeria for his assistance.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 18, 2015.
- Accepted May 7, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.