


Abstract
Objectives: To compare midazolam and propofol sedation in hypoalbuminemic geriatric patients under spinal anesthesia in hip surgery with bispectral index monitoring.
Methods: This prospective and randomized study was completed in the Department of Anesthesiology, Okmeydani Training and Research Hospital, Istanbul, Turkey between February 2013 and December 2014. Sixty patients undergoing elective hip surgery under spinal anesthesia in the geriatric age group with albumin levels below 3 g/dl were randomly divided into Group I and Group II. After administration of spinal block, Group I were given 0.05 mg/kg bolus midazolam, and then 0.02-0.1 mg/kg/hr dose infusion was begun. In Group II, 1 mg/kg bolus propofol was given within 10 minutes, and then 1-3 mg/kg/hr infusion was begun. The systolic arterial pressure, diastolic arterial pressure, mean arterial pressure, heart rate, peripheral oxygen saturation values, respiratory rate, and Wilson’s 5-stage sedation score were recorded at 15-minute intervals. At the end of the operation, the recovery time and surgeon satisfaction were recorded.
Results: The recovery times for patients in Group I were found to be longer than in Group II (p<0.05). The respiration rate in patients in Group I at the start of surgery, 15th minute of surgery, and after surgery were lower than in Group II (p<0.05).
Conclusion: We conclude that propofol is more reliable in terms of hemodynamic stability than midazolam, as it causes less respiratory depression and faster recovery in the propofol group.
Spinal anesthesia is used at very high rates in elderly patients, and is a well-tolerated anesthetic method. Even in geriatric patients with left ventricle failure and in spite of a clear reduction in systemic vascular resistance linked to spinal anesthesia, it is proven that stroke volume and cardiac output do not decrease much.1 Sedation is a very important component of patient management during regional anesthesia. As the patient is conscious during operation under regional anesthesia, the surgical environment may negatively affect the patient. These effects may be more obvious during orthopedic interventions due to the noise of tools used, long duration of tourniquet use, position given, and manipulation of patient extremities during the surgery. To remove the possibility of such effects, the most appropriate method is to administer sedation to the patient.2 It is very important that sedation administration be appropriate for the patient’s characteristics, as well as reliable, and effective. As a result, the appropriate dose of the correct sedative agent should be administered. In elderly patients especially, there is an increased sedative response to centrally effective agents.3,4 Midazolam and propofol are agents frequently used for sedation. Midazolam binds to plasma proteins, especially albumin at a rate of 98%. The free fraction increases in hypoalbuminemic patients.5,6 Propofol is significantly lipophilic and like medications, such as midazolam, 98% is carried bound to plasma proteins. As a result of pharmacokinetic changes due to advanced age, the same dose provides higher plasma concentrations, and this increase reduces the dose requirements. As maximal plasma concentrations are higher in the elderly, a situation occurs where the possibility of cardiorespiratory effects like hypotension, apnea, airway obstruction and/or oxygen desaturation is higher in these patients. Higher plasma levels reduce the distribution volume linked to age, and shows reduced clearance between compartments. As a result, lower doses of propofol are recommended for use in elderly patients at the start, and for maintenance, of sedation/anesthesia.7 In the elderly, hypoalbuminemia may occur linked to acute phase reaction, inflammation and trauma, in addition to malnutrition. Hypoalbuminemia is a frequent finding in geriatric hip surgery patients. Although there are many studies comparing propofol and midazolam sedation administered with spinal anesthesia,8-10 there is no study comparing the efficacy and reliability of midazolam and propofol for hypoalbuminemic geriatric patients. This study primarily aimed to prospectively and randomly compare the effects of midazolam and propofol on hemodynamic parameters and side effects in hypoalbuminemic geriatric patients undergoing hip surgery under spinal anesthesia. The secondary end points of this study were to compare the sedation levels of patients, postoperative recovery duration, and patient and surgeon satisfaction.
Methods
This study was approved by the ethical and research committee of Okmeydani Training and Research Hospital, and informed written consent was obtained from each subject. This prospective and randomized study was completed in the Department of Anesthesiology and Intensive Care, Okmeydani Training and Research Hospital, Istanbul, Turkey, between February 2013 and December 2014. Sixty hypoalbuminemic patients, undergoing elective hip surgery under spinal anesthesia, and in the geriatric age group with albumin levels below 3 g/dl were included in this study. The standard effect size of the study was determined as 0.83, with 80% power, and 5% error so the sample groups were calculated to require at least 26 individuals. According to calculations, the groups required at least 26 individuals, and taking into account losses during the study period, the decision was arrived at to include 30 individuals in each group. Before the operation, patients had routine systemic examinations completed, laboratory values were investigated, and patients joined the study groups. Patients with contraindications for spinal anesthesia (sepsis, bacteremia, regional skin infection, hypovolemia, coagulopathy, therapeutic anticoagulation, increased intracranial pressure, patient refusal of procedure), those with allergies to local anesthetics, and those with albumin levels above 3 g/dl were excluded from the study group. The patients were randomized using a closed envelope method into one of the 2 groups; midazolam (Dormicum,® Roche, Istanbul, Turkey) (Group I: n=30), and propofol (Propofol 1%, Fresenius,® Fresenius Kabi Medicine, Istanbul, Turkey) (Group II n=30). All methods were explained one day in advance and all cases provided written consent. They were not provided with solid food for at least 8 hours, and fluids for at least 4 hours before the operation. No case was given premedication. A vein was opened with a 20 G intravenous cannula, and before block prehydration was provided with 10 ml/kg 0.9% NaCl infusion for 30 minutes. The age, height, weight, and preoperative albumin values of the patients were noted. For monitoring, a Datex-Ohmeda S/5 Avance (General Electric Inc, Madison, WI, USA) monitor was used. Systolic arterial pressure (SAP), diastolic arterial pressure (DAP), mean arterial pressure (MAP), heart rate (HR), peripheral oxygen saturation values (SpO2), respiration rate (RR), and Wilson’s 5-stage sedation scores (1 - fully awake and oriented; 2 - drowsy; 3 - eyes closed but arousable to command; 4 - eyes closed but arousable to mild physical stimulation, and 5 - eyes closed but unarousable to mild physical stimulation)11 were recorded at the following times: initial values; after regional anesthesia; after bolus; start of surgery; 15th minute after the start of surgery; after the final suture; and on exit from the operating room (OR). In addition, the hemodynamic and respiratory parameters were observed during the whole operation time. Spinal block administration was completed in sitting position after skin cleansing with povidone iodine by entering the intrathecal interval at the L3-4, or L4-5 level with a 22 G spinal needle. As all patients were more than 50 years old, and post puncture headache is observed mostly in younger patients, a 22 G spinal needle was used. Hyperbaric bupivacaine (Marcaine®Spinal heavy, 0.5%, 4 mL ampule, AstraZeneca UK Ltd, Luton, Bedfordshire, UK) was administered into the spinal interval at the following rates; for cases 155-165 cm tall 12.5 mg; for cases 165-175 cm tall 13.5 mg; and for cases 175-190 cm tall 15 mg. After confirming the sensorial block had reached T 10 with a pin-prick test in the 10th minute, Group I was given 0.05 mg/kg bolus midazolam. Then infusion of midazolam was initiated with a dose of 0.02 mg/kg/hr, which was increased to a dose of 0.1 mg/kg/hr according to bispectral index (BIS) values. In Group II, 1 mg/kg bolus propofol was administered within 10 minutes. Then, 1 mg/kg/hr continuous infusion of propofol was started, and the dose was increased to 3 mg/kg/hr according to BIS values. To maintain BIS of 65-80%, infusion doses were raised or lowered by 50% in 5-minute intervals. A Braun McGaw infusion pump (Braun McGaw AG, Melsungen, Germany) was used for infusion. Sedation was continued until the first skin sutures in both groups. Perioperative side effects were assessed as hypotension, bradycardia, desaturation, and nausea-vomiting. The MAP falling below 70 mm Hg, or by more than 20% of the initial pressure was accepted as hypotension, HR falling below 50 beats/minute was bradycardia, and SpO2 falling below 90%, or RR <10/minute was accepted as respiratory depression. To regulate hypotension, colloid and crystalloid replacement, and if necessary ephedrine hydrochloride (5-25 mg IV) were administered. For bradycardia, atropine sulfate (0.5-1 mg IV) was used. It was planned that in cases with respiratory depression observed who did not respond to tactile and verbal stimuli, controlled respiration with a mask should be started. In situations of nausea or vomiting, 10 mg IV metoclopramide was given. For both groups, 2 one/min O2 was administered preoperatively and postoperatively through a mask. The recovery duration was accepted as the duration from the end of infusion to when the patient was fully awake, that is BIS >90, and Wilson’s 5-stage sedation score of 1. To assess the patient’s satisfaction with the anesthesia method used, in the 30th minute postoperatively while the effect of the spinal block continued, they were requested to use a 6 point scale (0 - very bad; 1 - bad; 2 - mild; 3 - good; 4 - very good; 5 - excellent). To assess surgeon’s satisfaction, the same scale was used. The patient and surgeon were blinded to the sedative drug used during this study by the anesthetists who assessed the outcomes.
Descriptive statistics of the data are given as mean, standard deviation, median, minimum, maximum, frequency, and percentage. The distribution of variables was measured with the Kolmogorov Smirnov test. Quantitative data were analyzed with the Mann-Whitney U test. Recurrent measurements were analyzed with the Wilcoxon test. For analysis of quantitative data, the chi square test was used, while the Fischer test was used when conditions for the chi-square test were not met. Statistical analysis was performed by Statistical Package for Social Sciences version 22 (IBM Corp, Armonk, NY, USA). Statistical significance was set at p<0.05.
Results
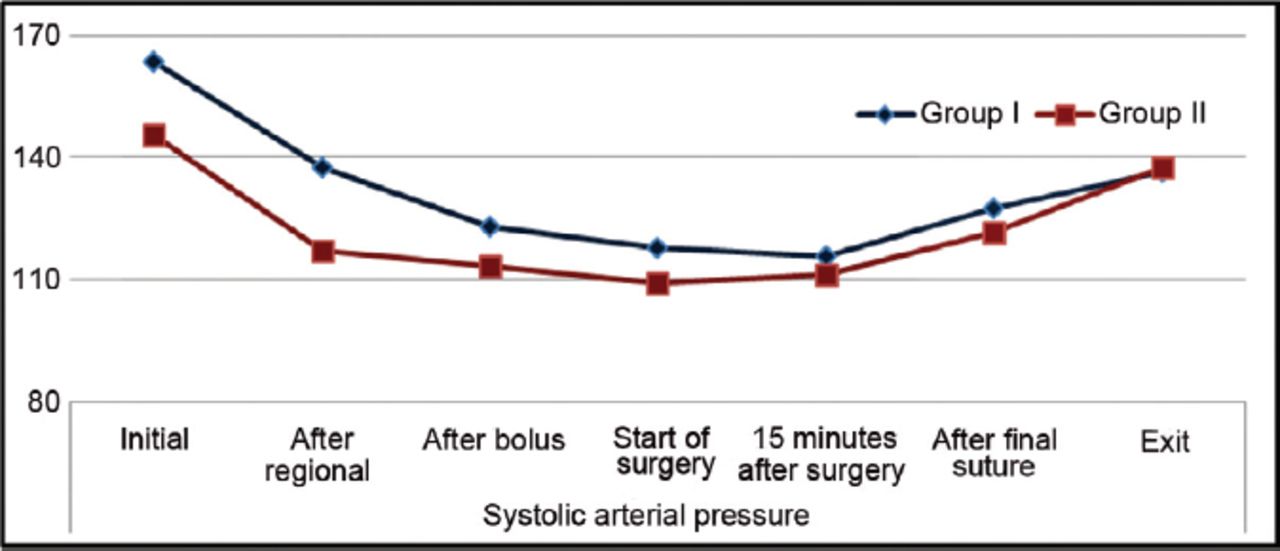
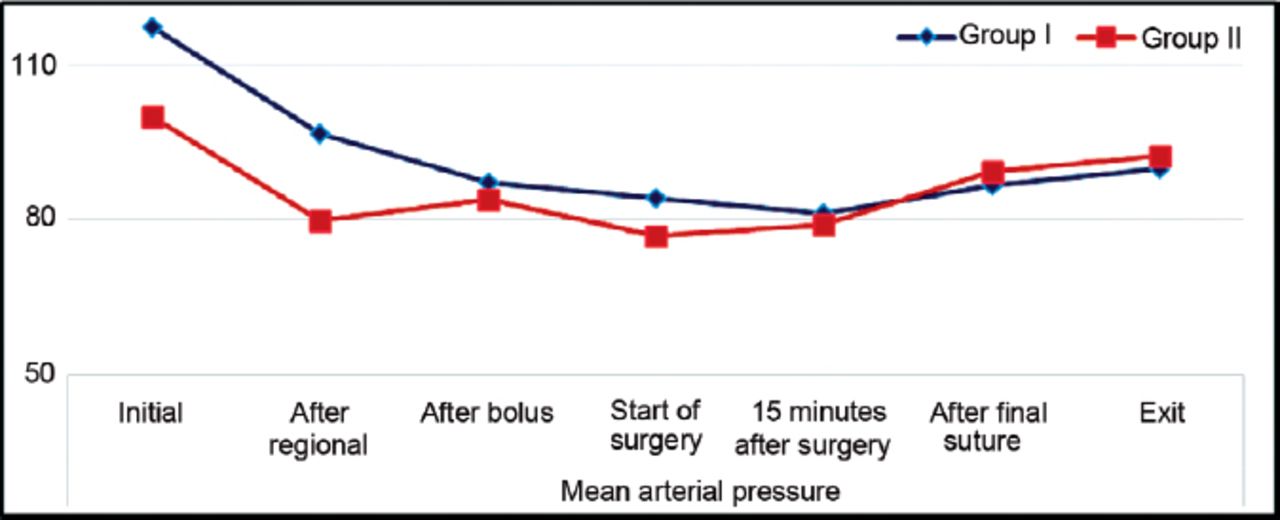
Spinal anesthesia was performed successfully for all patients. Failed or inadequate block was not seen in any patient. Patients in Group I and Group II showed no significant differences in terms of gender distribution, age, height, weight, operation duration, patient satisfaction score, surgeon satisfaction score, complication rates, and American Society of Anesthesiologists (ASA) distribution (p>0.05). The recovery duration for patients in Group I was significantly longer than in Group II (p<0.05) (Tables 1 - 3). There was no significant difference between the groups in terms of albumin values (p=0.267). While a significant fall was observed in SAP (p=0.003) and MAP (p=0.010) values at the exit from the OR compared with initial values in Group I, in Group II no significant change was observed compared with initial values (p>0.05) (Figures 1 & 2). In Group I after bolus, at the start of surgery, 15th minute of surgery, after surgery, and when leaving the OR, HR values showed a significant fall compared with initial values (p<0.05) (Figure 3). In Group I and Group II, initial, regional, after bolus, and exiting the OR, and sedation scores showed no significant difference (p>0.05). At the start of surgery, 15th minute of surgery, and at the end of surgery, the sedation score in Group I was significantly lower than in Group II (p<0.05) (Table 4).
Comparison of demographic values and ASA scores between groups using the Mann-Whitney U-test or Chi-square test.
Comparison of operation time, recovery period, patients and surgeon satisfaction, and between groups using the Mann-Whitney U-test, or Chi-square test.
The evaluation of complications between groups included in the study.

Comparison of the systolic arterial pressure of the 2 groups included in a study on sedation in Turkey.

Comparison of mean arterial pressure of the 2 groups included in a study on sedation in Turkey.
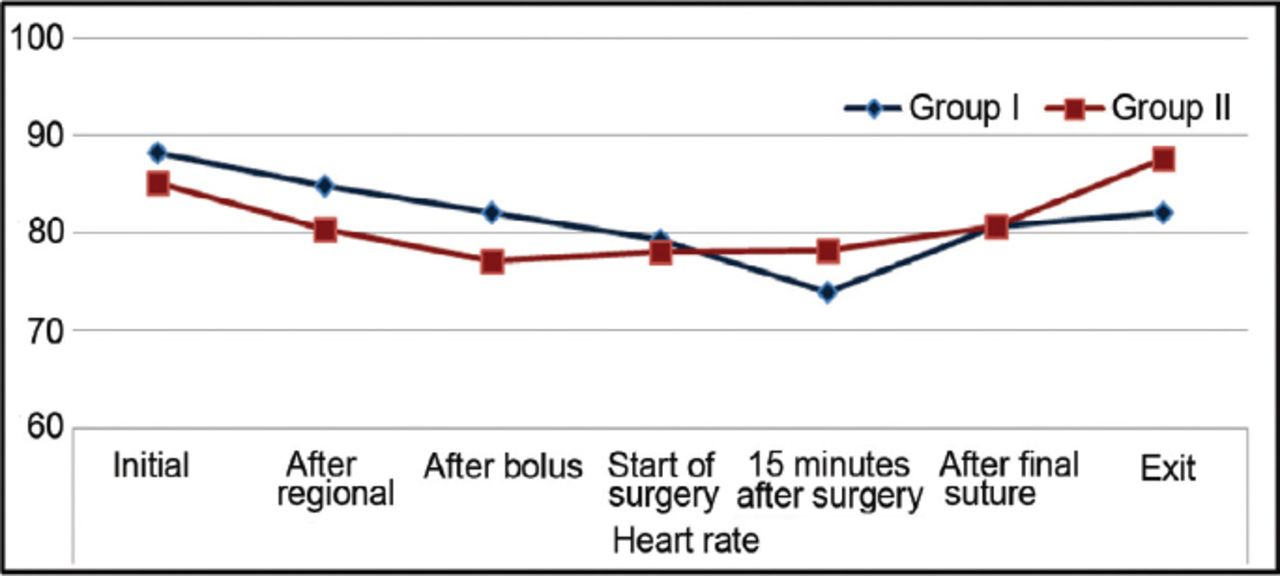
Comparison of heart rates of the 2 groups included in a study on sedation in Turkey.
Comparison of sedation score between the 2 groups using the Mann-Whitney U test and Wilcoxon test.
In Group I at the start of surgery, 15th minute of surgery, and after surgery, the increase in sedation score was significantly less than in Group II (p<0.05) (Table 4). In patients in Group I, RR at the start of surgery, 15th minute of surgery, and at the end of surgery was significantly lower than in Group II (p<0.05) (Table 5). In Group I, there was a significant fall in RR after bolus, at the start of surgery, and in the 15th minute of surgery compared with initial values (p<0.05). In Group II, there was no significant change in RR observed at regional, after surgery, and leaving the OR compared with initial values (p>0.05) (Table 5). There was no significant difference in the amount of change in RR at regional, 15th minute of surgery, after surgery, and leaving the OR between the 2 groups (p>0.05). In Group I, the reduction in RR after bolus, and at the start of surgery was significantly greater than the reduction in Group II (p<0.05) (Table 5).
Comparison of respiration rate between the 2 groups using the Mann-Whitney U test and Wilcoxon test.
Discussion
It has been stated in many publications that it is necessary to titrate the dose of sedative agents for geriatric patients. Hypoalbuminemia is frequently observed in geriatric patients. Albumin is used in the inflammation process, especially in elderly patients exposed to trauma and nutritional insufficiency, and accompanying infections may also cause hypoalbuminemia. The ideal sedative agent for use during regional anesthesia will provide sedation or sleep with reliable airway maintenance, have minimal circulatory and respiratory effects, and allow quick recovery without residual drowsiness.12 Serum albumin levels play an important role in providing physiological hemostasis. With reduced albumin level damage to homeostatic functions may be observed, and may cause progression of pathological processes.13 Hypoalbuminemia affects the pharmacokinetics of many medications, which bind to plasma proteins. It has been known for many years that propofol and midazolam bind to plasma proteins at rates of 96-98%.7,14 Midazolam, especially, is carried bound to albumin in plasma and in elderly patients, even low doses may have exaggerated effects due to hypoalbuminemia. Additionally, sedative doses inhibit the hypoxic ventilatory response, and may cause hypoxemia, hypoventilation, airway obstruction, apnea, arrhythmia, hypotension, and vasovagal reactions.15-17
Sedation should be planned in light of clinical assessment of each patient to determine possible complications.18-20 There is no study comparing the reliability and efficacy of midazolam and propofol as sedation agents for hypoalbuminemic geriatric patients undergoing hip surgery with spinal anesthesia. Hypoalbuminemia, frequently seen in the geriatric patient group is a factor that can change the effectiveness of sedation agents. In our study, we began by considering that the effects of agents, such as midazolam and propofol, which bind to plasma proteins, may change in hypoalbuminemic patients, and reliability may be reduced, and aimed to compare these 2 medications to determine the ideal sedation agent for these patients.
It is known that propofol and midazolam inhibit sympathetic activity and reduce systemic vascular resistance by an amount that may cause bradycardia and hypotension.21,22 It is reported that sedative doses of propofol and midazolam do not change initial cardiovascular parameters.23 In our study of the hypoalbuminemic geriatric patient group, in both groups while SAP and MAP values were reduced compared with initial values, the value on exit from the OR in the propofol group showed no difference from initial values. When compared with midazolam, although there are studies reporting greater hypotension-creating effects,24,25 in our study propofol appeared to be hemodynamically more reliable on exit from the OR postoperatively. Additionally, although no hypotension or bradycardia severe enough to disrupt hemodynamic stability was encountered, in the midazolam group, the HR values showed a greater reduction compared with initial values. When induction doses are given, both midazolam and propofol have effects that may create respiratory depression. The suppressive effect of propofol, especially on respiration is more apparent.25-29 During spinal anesthesia in a study comparing midazolam and propofol infusion for sedation purposes there was no difference found between the 2 medications in terms of effect on respiration rate.10 In our study, in the midazolam group after bolus injection respiratory depression was greater compared with the propofol group. As the operation progressed, the propofol group showed a reduction in RR; however, there was no significant difference observed in peripheral SO2 values in both groups given 2 one/min O2.
Our study found that with BIS used to standardize sedation levels, in geriatric and hypoalbuminemic patients in the midazolam and propofol groups after sedation was ceased, the recovery time to reach the same score was longer in the midazolam group. Similarly, in a study of 20-50 year old patients without hypoalbuminemia, the recovery time in the propofol group was shorter than the midazolam group.24
A limitation of this study was that, without considering sedation or cognitive disorders that may develop in geriatric patients, evaluation of patient satisfaction was completed 30 minutes after the end of operation. Longer monitoring duration in the postoperative period may provide more correct results. The effect of both medications on cognitive functions in hypoalbuminemic patients may also require further research.
In conclusion, in our study comparing midazolam and propofol sedation of hypoalbuminemic geriatric hip surgery cases with spinal anesthesia accompanied by BIS, both agents can be used for sedation without causing any serious complications. However, we conclude that propofol is more reliable than midazolam in terms of hemodynamic stability, causes less respiratory depression, and shorter recovery time. Further studies with different and newer sedation agents are needed to determine, which drug is more reliable in hypoalbuminemic geriatric patients for sedation.
Related Articles
Wang J, Pang L, Han W, Li G, Wang N. Effect of preemptive intravenous oxycodone on low-dose bupivacaine spinal anesthesia with intrathecal sufentanil. Saudi Med J 2015; 36: 437-441.
Hijazi OM, Ahmed AE, Anazi JA, Al-Hashemi HE, Al-Jeraisy MI. Chloral hydrate versus midazolam as sedative agents for diagnostic procedures in children. Saudi Med J 2014; 35: 123-131.
Topuz D, Postaci A, Sacan O, Yildiz N, Dikmen B. A comparison of sevoflurane induction versus propofol induction for laryngeal mask airway insertion in elderly patients. Saudi Med J 2010; 31: 1124-1129.
- Received May 18, 2015.
- Accepted August 3, 2015.
- Copyright: © Saudi Medical Journal
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.